



- Overview of Spinal Cord Disorders
- Acute Transverse Myelitis
- Cauda Equina Syndrome
- Cervical Spondylosis and Spondylotic Cervical Myelopathy
- Hereditary Spastic Paraplegia
- Spinal Cord Arteriovenous Malformations (AVMs)
- Spinal Cord Autonomic Dysreflexia
- Spinal Cord Compression
- Spinal Cord Infarction
- Spinal Epidural Abscess
- Spinal Subdural or Epidural Hematoma
- Subacute Combined Degeneration
- Syrinx of the Spinal Cord or Brain Stem
- HTLV-1–Associated Myelopathy/Tropical Spastic Paraparesis (HAM/TSP)
A syrinx is a fluid-filled cavity within the spinal cord (syringomyelia) or brain stem (syringobulbia). Predisposing factors include craniocervical junction abnormalities, previous spinal cord trauma, and spinal cord tumors. Symptoms include flaccid weakness of the hands and arms and deficits in pain and temperature sensation in a capelike distribution over the back and neck; light touch and position and vibration sensation are not affected. Diagnosis is by MRI. Treatment includes correction of the cause and surgical procedures to drain the syrinx or otherwise open the flow of cerebrospinal fluid.
Topic Resources

(See also Overview of Spinal Cord Disorders.)
Syrinxes usually result from lesions that partially obstruct flow of cerebrospinal fluid (CSF). At least half of syrinxes occur in patients with congenital abnormalities of the craniocervical junction (eg, herniation of cerebellar tissue into the spinal canal, called Chiari malformation), brain (eg, encephalocele), or spinal cord (eg, myelomeningocele). For unknown reasons, these congenital abnormalities often expand during the teen or young adult years.
A syrinx can also develop in patients who have a spinal cord tumor, scarring due to previous spinal trauma, or no known predisposing factors. About a third of people with a spinal cord tumor eventually develop a syrinx.
Syringomyelia is a paramedian, usually irregular, longitudinal cavity. It commonly begins in the cervical area but may extend downward along the entire length of the spinal cord.
Syringobulbia, which is rare, usually occurs as a slitlike gap within the lower brain stem and may disrupt or compress the lower cranial nerve nuclei or ascending sensory or descending motor pathways.
Symptoms and Signs of Syrinx
Symptoms of a syrinx usually begin insidiously between adolescence and age 45.
Syringomyelia develops in the center of the spinal cord, causing a central cord syndrome (see table Spinal Cord Syndromes). Pain and temperature sensory deficits occur early but may not be recognized for years. The first abnormality recognized may be a painless burn or cut. Syringomyelia typically causes weakness, atrophy, and often fasciculations and hyporeflexia of the hands and arms; a deficit in pain and temperature sensation in a capelike distribution over the shoulders, arms, and back is characteristic. Light touch and position and vibration sensation are not affected. Later, spastic leg weakness develops. Deficits may be asymmetric.
Syringobulbia may cause vertigo, nystagmus, unilateral or bilateral loss of facial sensation, lingual atrophy and weakness, dysarthria, dysphagia, hoarseness, and sometimes peripheral sensory or motor deficits due to medullary compression.
Diagnosis of Syrinx
MRI of spinal cord and brain with gadolinium
A syrinx is suggested by an unexplained central cord syndrome or other characteristic neurologic deficits, particularly pain and temperature sensory deficits in a capelike distribution.

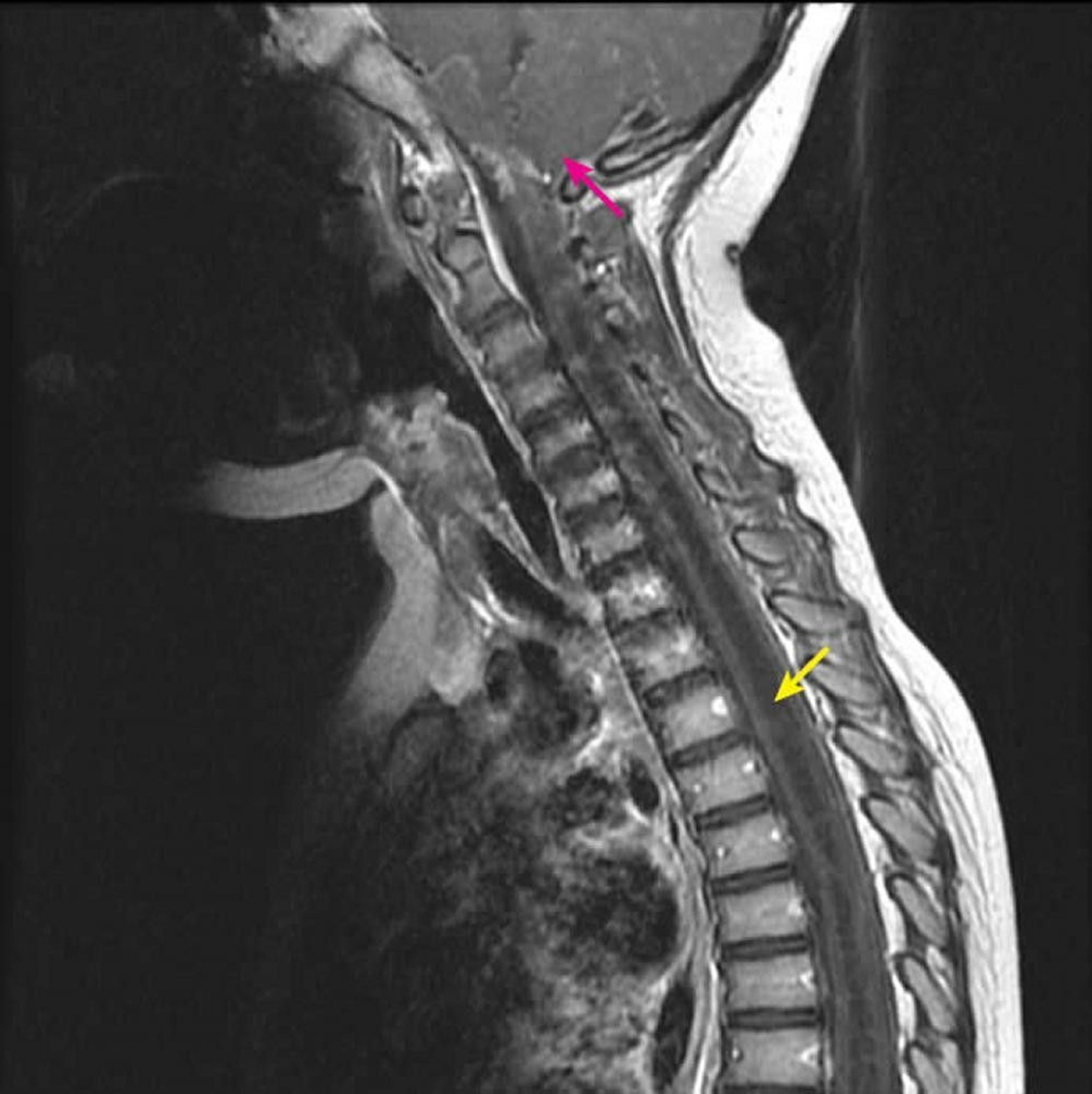
Courtesy of John Tsiouris, MD, Division of Neuroradiology, New York–Presbyterian Hospital/Weill Cornell Medical Center.
MRI of the entire spinal cord and brain is done. Gadolinium enhancement is useful for detecting any associated tumor.
Treatment of Syrinx
Sometimes surgical decompression
Underlying problems (eg, craniocervical junction abnormalities, postoperative scarring, spinal tumors) are corrected when possible.
Surgical decompression of the foramen magnum and upper cervical cord is the only useful treatment, but surgery usually cannot reverse severe neurologic deterioration, and the syrinx may recur.
Key Points
At least half of syrinxes occur in patients with congenital abnormalities of the craniocervical junction, brain, or spinal cord; syrinxes may also result from a spinal cord tumor or spinal trauma.
Syringomyelia (a syrinx within the spinal cord) causes central cord syndrome; symptoms include pain and temperature sensory deficits in a capelike distribution, weakness, atrophy, and, later, spastic leg weakness.
Syringobulbia (a syrinx in the brain stem), which is rare, may cause vertigo, nystagmus, unilateral or bilateral loss of facial sensation, lingual atrophy and weakness, dysarthria, dysphagia, hoarseness, and sometimes peripheral sensory or motor deficits.
Diagnose using MRI with gadolinium enhancement.
Treat with surgical decompression, and correct underlying problems when possible; usually, surgery cannot reverse severe neurologic deterioration.







