



Topic Resources


Most intracerebral hemorrhages occur in the basal ganglia, cerebral lobes, cerebellum, or pons. The most common location for hemorrhage due to hypertension is the putamen. Intracerebral hemorrhage may also occur in other parts of the brain stem or in the midbrain.
Etiology of Intracerebral Hemorrhage
Intracerebral hemorrhage usually results from rupture of an arteriosclerotic small artery that has been weakened, primarily by chronic arterial hypertension. Such hemorrhages are usually large, single, and catastrophic. Other modifiable risk factors that contribute to arteriosclerotic hypertensive intracerebral hemorrhages include cigarette smoking, obesity, and a high-risk diet (eg, high in saturated fats, trans fats, and calories). Use of cocaine or, occasionally, other sympathomimetic drugs or medications can cause transient severe hypertension leading to hemorrhage. , and a high-risk diet (eg, high in saturated fats, trans fats, and calories). Use of cocaine or, occasionally, other sympathomimetic drugs or medications can cause transient severe hypertension leading to hemorrhage.
Less often, intracerebral hemorrhage results from congenital aneurysm, arteriovenous malformations, other vascular malformations, trauma, mycotic aneurysm, brain infarct (hemorrhagic infarction), primary or metastatic brain tumor, excessive anticoagulation, blood dyscrasia, intracranial arterial dissection, Moyamoya disease, or a bleeding or vasculitic disorder. The most common causes of metastatic intracerebral hemorrhage include melanoma, renal cell carcinoma, and choriocarcinoma.
Lobar intracerebral hemorrhages (hematomas in the cerebral lobes, outside the basal ganglia) usually result from angiopathy due to amyloid deposition in cerebral arteries (cerebral amyloid angiopathy), which affects primarily older adults. Lobar hemorrhages may be multiple and recurrent.
Pathophysiology of Intracerebral Hemorrhage
Chronic arterial hypertension leads to formation of microaneurysms (Charcot-Bouchard aneurysms) in small perforating arteries which may rupture and cause intracerebral hemorrhage.
Blood from an intracerebral hemorrhage accumulates as a mass that can dissect through and compress adjacent brain tissues, causing neuronal dysfunction. Large hematomas increase intracranial pressure. Pressure from supratentorial hematomas and the accompanying edema may cause transtentorial brain herniation, compressing the brain stem and often causing secondary hemorrhages in the midbrain and pons.
If the hemorrhage ruptures into the ventricular system (intraventricular hemorrhage), blood may cause acute hydrocephalus, an independent predictor for a worse outcome after intracerebral hemorrhage. Cerebellar hematomas can expand to block the 4th ventricle, also causing acute hydrocephalus, or they can dissect into the brain stem. Cerebellar hematomas that are > 3 cm in diameter may cause midline shift or herniation.
Herniation, midbrain or pontine hemorrhage, intraventricular hemorrhage, acute hydrocephalus, or dissection into the brain stem can impair consciousness and cause coma and death.
Symptoms and Signs of Intracerebral Hemorrhage
Symptoms of intracerebral hemorrhage typically begin with sudden headache, often during activity. However, headache may be mild or absent in older adults. Loss of consciousness is common, often within seconds or a few minutes. Nausea, vomiting, delirium, and focal or generalized seizures are also common.
Neurologic deficits are usually sudden and progressive. Large hemorrhages, when located in the hemispheres, cause hemiparesis; when located in the posterior fossa, they cause cerebellar or brain stem deficits (eg, conjugate eye deviation or ophthalmoplegia, stertorous breathing, pinpoint pupils, coma).
Large hemorrhages are fatal within a few days in approximately half of patients. In survivors, consciousness returns and neurologic deficits gradually diminish to various degrees as the extravasated blood is resorbed. Some patients have surprisingly few neurologic deficits because hemorrhage is less destructive to brain tissue than infarction.
Small hemorrhages may cause focal deficits without impairment of consciousness and with minimal or no headache and nausea. Small hemorrhages may mimic ischemic stroke.
Diagnosis of Intracerebral Hemorrhage
Neuroimaging
Diagnosis of intracerebral hemorrhage is suggested by sudden onset of headache, focal neurologic deficits, and impaired consciousness, particularly in patients with risk factors.
Intracerebral hemorrhage must be distinguished from
Other causes of acute neurologic deficits (eg, seizure, hypoglycemia)
Blood glucose level should be measured at the bedside immediately.
A complete blood count (CBC) and coagulation studies (international normalized ratio [INR], partial thromboplastin time [PTT]) are performed.
Immediate CT or MRI is necessary. Neuroimaging is usually diagnostic. If neuroimaging shows no hemorrhage but subarachnoid hemorrhage is suspected clinically, lumbar puncture is necessary to look for xanthochromia.
CT angiography (CTA), performed within hours of bleeding onset, may show areas where contrast extravasates into the clot (spot sign); this finding indicates that bleeding is continuing and suggests that the hematoma will expand and the outcome will be poor.

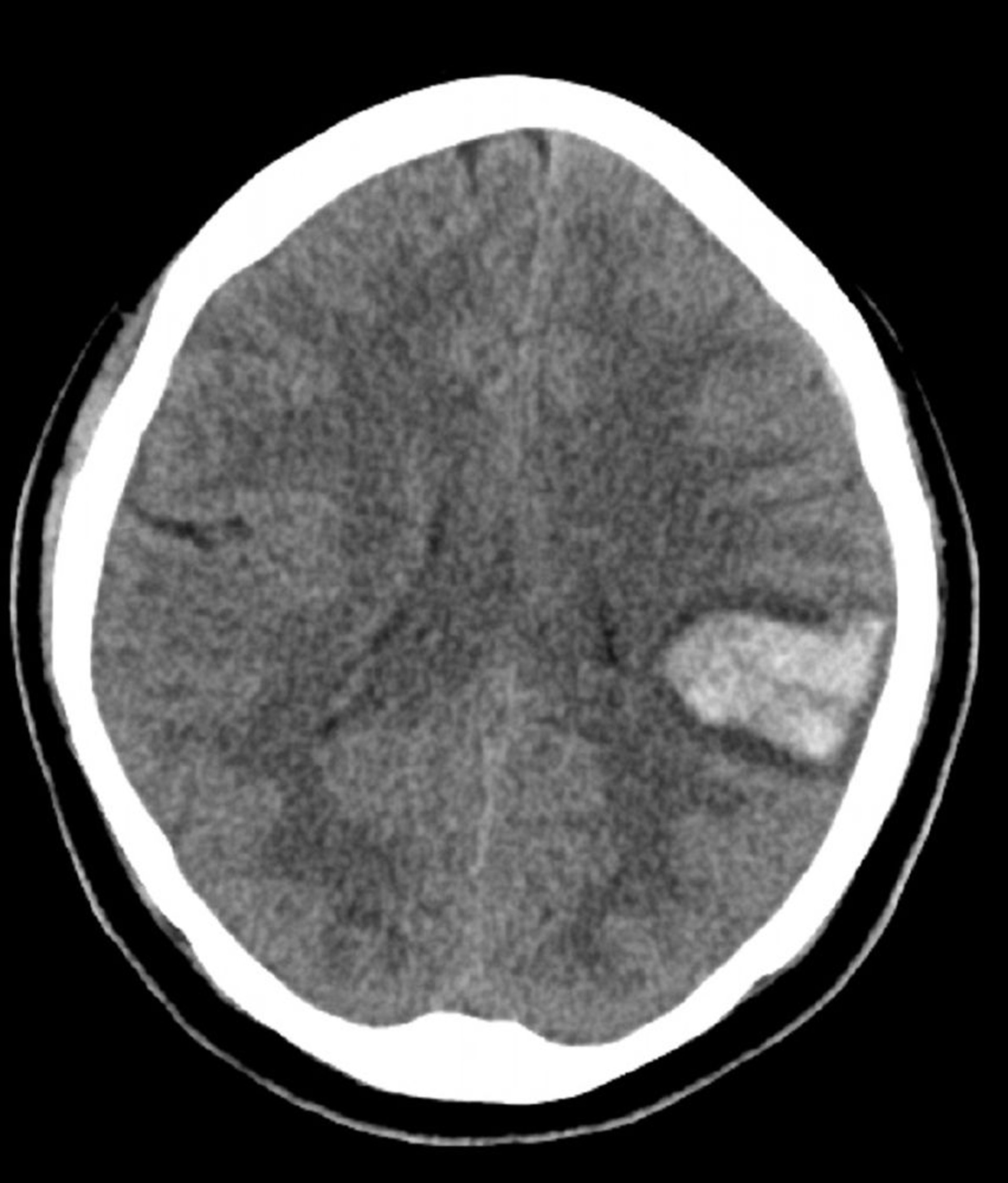
© 2017 Elliot K. Fishman, MD.

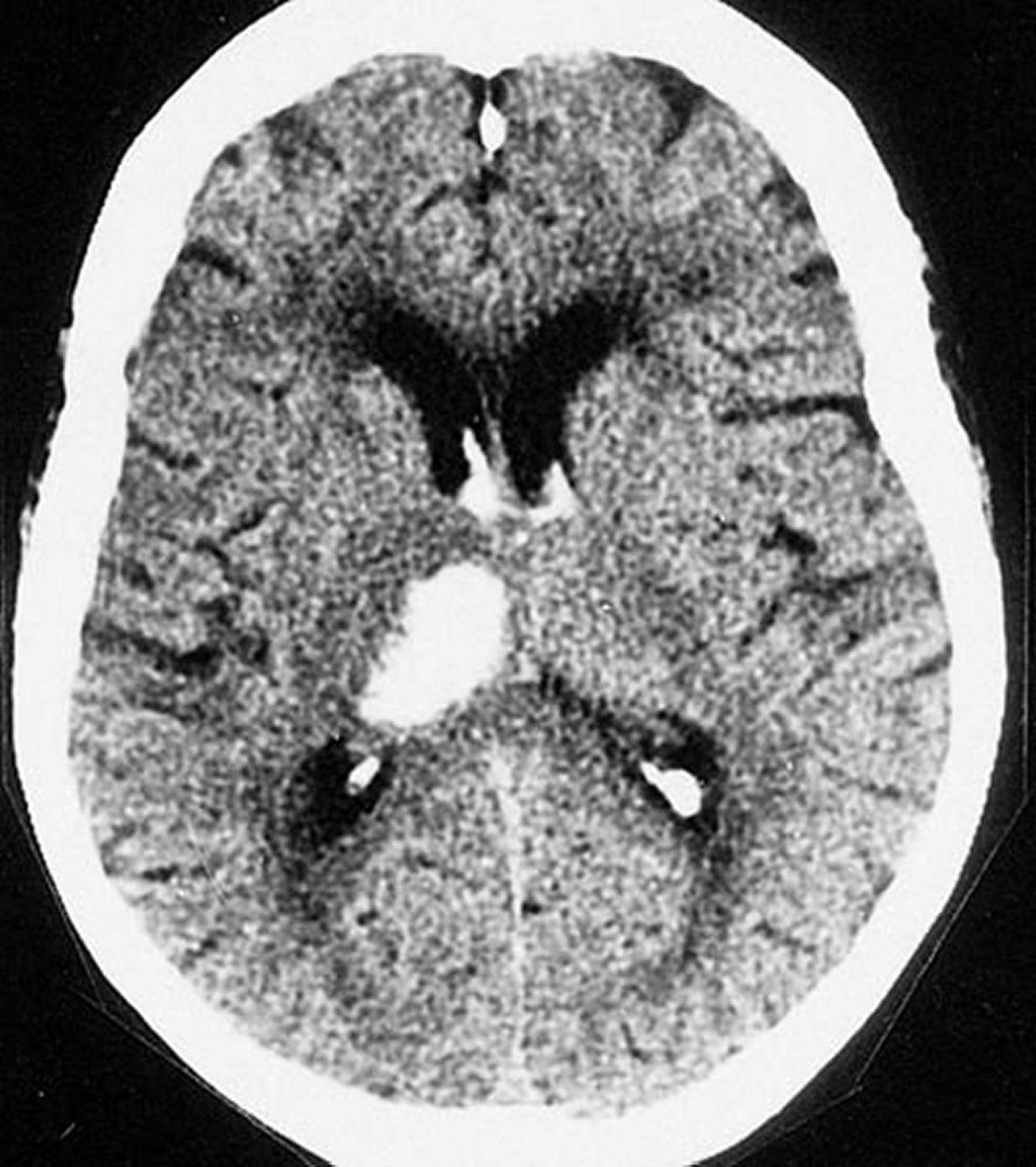
By permission of the publisher. From Furie K, et al. In Atlas of Clinical Neurology. Edited by RN Rosenberg. Philadelphia, Current Medicine, 2002.
Treatment of Intracerebral Hemorrhage
Supportive measures
Control of modifiable risk factors
Sometimes surgical evacuation (eg, for many cerebellar hematomas > 3 cm)
Treatment of intracerebral hemorrhage includes supportive measures and control of modifiable risk factors.
Anticoagulants and antiplatelet medications are contraindicated. If patients have used anticoagulants, the effects are reversed when possible by giving fresh frozen plasma, prothrombin complex concentrate, vitamin K, or platelet transfusions as indicated. Antidotes for direct oral anticoagulants are idarucizumab for dabigatran and andexanet alfa for apixaban and rivaroxaban.Anticoagulants and antiplatelet medications are contraindicated. If patients have used anticoagulants, the effects are reversed when possible by giving fresh frozen plasma, prothrombin complex concentrate, vitamin K, or platelet transfusions as indicated. Antidotes for direct oral anticoagulants are idarucizumab for dabigatran and andexanet alfa for apixaban and rivaroxaban.
As recommended by the American Heart Association and American Stroke Association 2022 guidelines, hypertension can be safely lowered to systolic blood pressure (BP) 140 mm Hg if systolic BP is between 150 mm Hg and 220 mm Hg and if acute antihypertensive treatment is not contraindicated (1). If systolic BP is > 220 mm Hg, hypertension can be treated aggressively with a continuous IV infusion of nicardipine, with doses carefully titrated and frequent monitoring of systolic BP to decrease it by 10 to 15%. The goal is to avoid high blood pressure peaks and variability, thus ensuring sustained BP control and improving functional outcomes. Maintaining BP close to 140/80 mm Hg and frequent monitoring to avoid hypotensive episodes are recommended. In patients presenting with systolic BP> 150 mm Hg, sudden lowering to levels < 120 mm Hg can lead to poor outcomes (eg, acute kidney injury). ). If systolic BP is > 220 mm Hg, hypertension can be treated aggressively with a continuous IV infusion of nicardipine, with doses carefully titrated and frequent monitoring of systolic BP to decrease it by 10 to 15%. The goal is to avoid high blood pressure peaks and variability, thus ensuring sustained BP control and improving functional outcomes. Maintaining BP close to 140/80 mm Hg and frequent monitoring to avoid hypotensive episodes are recommended. In patients presenting with systolic BP> 150 mm Hg, sudden lowering to levels < 120 mm Hg can lead to poor outcomes (eg, acute kidney injury).
Cerebellar hemisphere hematomas that are > 3 cm in diameter may cause midline shift or herniation, so surgical evacuation is often lifesaving. Early evacuation of large lobar cerebral hematomas may also be lifesaving, but rebleeding occurs frequently, sometimes increasing neurologic deficits. Early evacuation of deep cerebral hematomas is seldom indicated because surgical mortality is high and neurologic deficits are usually severe.
Because the presence of hydrocephalus predicts a worse outcome after intracerebral hemorrhage, surgeons may place an external ventricular drain to rapidly decrease intracranial pressure. This procedure can be lifesaving.
Antiseizure medications are used only if patients have had a seizure, but are not typically given prophylactically..
Treatment reference
1. Greenberg SM, Ziai WC, Cordonnier C, et al. 2022 Guideline for the management of patients with spontaneous intracerebral hemorrhage: A guideline from the American Heart Association/American Stroke Association. Stroke. 53 (7):e282–e361, 2022. doi: 10.1161/STR.0000000000000407 Epub 2022 May 17.
Key Points
With intracerebral hemorrhage, sudden, severe symptoms (eg, sudden severe headache, loss of consciousness, vomiting) are common, but headache may be absent or mild (particularly in older adults), and small hemorrhages may mimic ischemic stroke.
Do CT or MRI and a bedside glucose test immediately.
Essential supportive care may include reversing anticoagulation and decreasing BP to 140 mm Hg if systolic BP is between 150 mm Hg and 220 mm Hg; if systolic BP is > 220 mm Hg, consider aggressively reducing BP by continuously infusing nicardipine IV. Essential supportive care may include reversing anticoagulation and decreasing BP to 140 mm Hg if systolic BP is between 150 mm Hg and 220 mm Hg; if systolic BP is > 220 mm Hg, consider aggressively reducing BP by continuously infusing nicardipine IV.
Avoid BP fluctuations, and maintain systolic BP < 140 mm Hg, but not lower than 130 mm Hg.
Consider surgical evacuation for large lobar cerebral hematomas and hematomas > 3 cm in a cerebellar hemisphere.
Consider placing an external ventricular drain for select patients with signs of hydrocephalus and increased intracerebral pressure.
Drugs Mentioned In This Article






