


- Overview of Congenital Cardiovascular Anomalies
- Aortopulmonary Window
- Atrial Septal Defect (ASD)
- Atrioventricular Septal Defect
- Bicuspid Aortic Valve
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Double Outlet Right Ventricle
- Ebstein Anomaly
- Eisenmenger Syndrome
- Hypoplastic Left Heart Syndrome
- Patent Ductus Arteriosus (PDA)
- Persistent Truncus Arteriosus
- Tetralogy of Fallot
- Total Anomalous Pulmonary Venous Return (TAPVR)
- Transposition of the Great Arteries (TGA)
- Tricuspid Atresia
- Ventricular Septal Defect (VSD)
- Other Congenital Cardiac Anomalies
Tetralogy of Fallot consists of 4 features: a large ventricular septal defect, right ventricular outflow tract obstruction and pulmonic valve stenosis, right ventricular hypertrophy, and over-riding of the aorta. Symptoms include cyanosis, dyspnea with feeding, poor growth, and hypercyanotic "tet" spells (sudden, potentially lethal episodes of severe cyanosis). A harsh systolic murmur at the left upper sternal border with a single second heart sound (S2) is common. Diagnosis is by echocardiography. Definitive treatment is surgical repair.


(See also Overview of Congenital Cardiovascular Anomalies.)
Tetralogy of Fallot (see figure Tetralogy of Fallot) accounts for 7 to 10% of congenital heart anomalies. Associated anomalies include right aortic arch (25%), abnormal coronary artery anatomy (5 to 10%), stenosis of the pulmonary artery branches, presence of aorticopulmonary collateral vessels, patent ductus arteriosus, complete atrioventricular septal defect, atrial septal defect, additional muscular ventricular septal defects (VSDs), and aortic valve regurgitation.
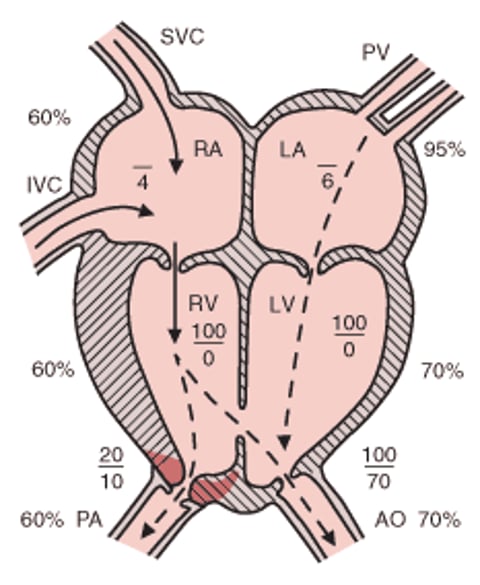
Tetralogy of Fallot
Pulmonary blood flow is decreased, the RV is hypertrophied, and unoxygenated blood enters the AO. Systolic pressures in the RV, LV, and AO are identical. Level of arterial desaturation is related to severity of the RV outflow tract obstruction. Atrial pressures are mean pressures. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |

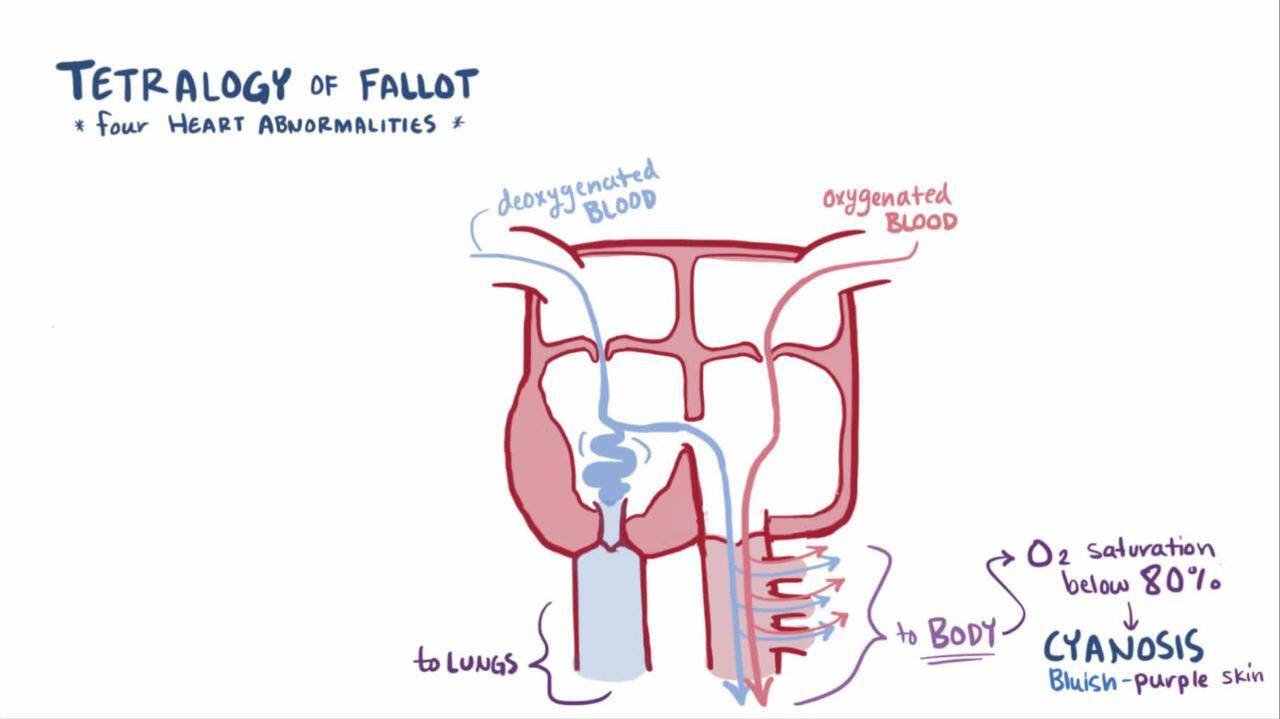
Pathophysiology of Tetralogy of Fallot
The ventricular septal defect in tetralogy of Fallot is often described as a malalignment type, since the conal septum is displaced anteriorly. This displaced septum protrudes into the pulmonary outflow tract, often resulting in obstruction and hypoplasia of the downstream structures, including the pulmonary valve, main pulmonary artery, and branch pulmonary arteries. The ventricular septal defect (VSD) is typically large; thus, systolic pressures in the right and left ventricles (and in the aorta) are the same. Pathophysiology depends on the degree of right ventricular outflow obstruction. A mild obstruction may result in a net left-to-right shunt through the VSD; a severe obstruction causes a right-to-left shunt, resulting in low systemic arterial saturation (cyanosis) that is unresponsive to supplemental oxygen.

Hypercyanotic spells
In some children with unrepaired tetralogy of Fallot, most often those several months up to 2 years of age, sudden episodes of profound cyanosis and hypoxia (hypercyanotic or "tet" spells) may occur, which may be lethal. A spell may be triggered by any event that slightly decreases oxygen saturation (eg, crying, defecating) or that suddenly decreases systemic vascular resistance (eg, playing, kicking legs when awakening) or by sudden onset of tachycardia or hypovolemia.
The mechanism of a hypercyanotic spell remains uncertain, but several factors are probably important in causing an increase in right-to-left shunting and a fall in arterial oxygen saturation. Factors include
An increase in right ventricular outflow tract obstruction
An increase in pulmonary vascular resistance
A decrease in systemic resistance
These factors lead to a vicious circle caused by the initial fall in arterial PO2, which stimulates the respiratory center and causes hyperpnea and increased adrenergic tone. The increased circulating catecholamines then stimulate increased contractility, which increases outflow tract obstruction.
Symptoms and Signs of Tetralogy of Fallot
Neonates with severe right ventricular outflow obstruction (or atresia) have severe cyanosis and dyspnea during feeding, leading to poor weight gain. Neonates with mild obstruction may not have cyanosis at rest.
Hypercyanotic spells may be precipitated by activity and are characterized by paroxysms of hyperpnea (rapid and deep respirations), irritability and prolonged crying, increasing cyanosis, and decreasing intensity or disappearance of the heart murmur. The spells occur most often in young infants; peak incidence is age 2 to 4 months. A severe spell may lead to limpness, seizures, and occasionally death. During play, some toddlers may intermittently squat, a position that increases systemic vascular resistance and aortic pressure, which decreases right-to-left ventricular shunting and thus raises arterial oxygen saturation.
Auscultation detects a harsh grade 3 to 5/6 systolic ejection murmur at the left mid and upper sternal border (see table Heart Murmur Intensity). The murmur in tetralogy is due to the pulmonic stenosis; the ventricular septal defect is usually silent because it is large and has no pressure gradient. Therefore, as the pulmonary outflow obstruction becomes more severe, the murmur becomes softer. The second heart sound (S2) is usually single because the pulmonary component is markedly reduced. A prominent right ventricular impulse and a systolic thrill may be present.
Diagnosis of Tetralogy of Fallot
Chest x-ray and ECG
Echocardiography
Diagnosis of tetralogy of Fallot is suggested by history and clinical examination, supported by chest x-ray and ECG, and established by 2-dimensional echocardiography with color flow and Doppler studies.
Chest x-ray shows a boot-shaped heart with a concave main pulmonary artery segment and diminished pulmonary vascular markings. A right aortic arch is present in 25%.
ECG shows right ventricular hypertrophy and right axis deviation and may also show right atrial enlargement.
Cardiac catheterization is rarely needed, unless there is suspicion of a coronary artery anomaly that might affect the surgical approach (eg, anterior descending arising from the right coronary artery) that cannot be clarified with echocardiography. MRI or CT may also be used to demonstrate coronary artery anatomy.
Treatment of Tetralogy of Fallot
For symptomatic neonates, prostaglandin E1 infusion
For hypercyanotic spells, knee-chest positioning, calming, oxygen, IV fluids, and sometimes drugs
Surgical repair
Neonates with severe cyanosis may be palliated with an infusion of prostaglandin E1 (beginning at 0.05 to 0.1 mcg/kg/minute IV) to open the ductus arteriosus and thereby increase pulmonary blood flow.
Hypercyanotic spells
Hypercyanotic spells require immediate intervention. The first steps are to
Place infants in a knee-chest position (older children usually squat spontaneously and do not develop hypercyanotic spells)
Establish a calm environment
Give supplemental oxygen
Give IV fluids for volume expansion
If the spell persists, standard medical therapy includes morphine, phenylephrine, and beta-blockers (propranolol or esmolol): see table If the spell persists, standard medical therapy includes morphine, phenylephrine, and beta-blockers (propranolol or esmolol): see tableMedications for Hypercyanotic Spells.
Medications for Hypercyanotic Spells
Medication | Route | Initial Dose | Maximum Dose |
|---|---|---|---|
EsmololEsmolol | IV | 100–500 mcg/kg over 1 minute Follow with infusion 25–100 mcg/kg/minute | 500 mcg/kg/minute |
MorphineMorphine | IV, intramuscular, or subcutaneous | 0.1 mg/kg | 0.1 mg/kg |
PhenylephrinePhenylephrine | IV | 5–20 mcg/kg every 10 to 15 minutes as needed Follow with infusion 0.1–0.5 mcg/kg/minute | Max bolus 500 mcg Max infusion 5 mcg/kg/minute |
PropranololPropranolol | IV | 0.015–0.02 mg/kg, titrate to effect | 0.1–0.2 mg/kg |
If standard measures do not control the spell, systemic blood pressure can be increased with ketamine 0.5 to 2 mg/kg IV or 2 to 3 mg /kg intramuscular injection (ketamine also has a beneficial sedating effect). If standard measures do not control the spell, systemic blood pressure can be increased with ketamine 0.5 to 2 mg/kg IV or 2 to 3 mg /kg intramuscular injection (ketamine also has a beneficial sedating effect).
Case reports describe the use of intranasal midazolam and intranasal fentanyl as alternatives to morphine for management of hypercyanotic spells. These medications have the advantage of not requiring IV access (Case reports describe the use of intranasal midazolam and intranasal fentanyl as alternatives to morphine for management of hypercyanotic spells. These medications have the advantage of not requiring IV access (1, 2).
Sodium bicarbonate, 1 mEq/kg IV, may be given if Sodium bicarbonate, 1 mEq/kg IV, may be given ifmetabolic acidosis is present.
Ultimately, if positioning and medications do not relieve the spell or if the infant is rapidly deteriorating, tracheal intubation with muscle paralysis and general anesthesia, extracorporeal membrane oxygenation (ECMO), or urgent surgical intervention may be necessary.
Propranolol 0.25 to 1 mg/kg orally every 6 hours (given until surgical repair) may prevent recurrences. Most experts think that even one significant spell indicates the need for expeditious surgical repair.Propranolol 0.25 to 1 mg/kg orally every 6 hours (given until surgical repair) may prevent recurrences. Most experts think that even one significant spell indicates the need for expeditious surgical repair.
Definitive management
Complete repair of tetralogy of Fallot consists of patch closure of the ventricular septal defect, widening of the right ventricular outflow tract with muscle resection, pulmonic valvuloplasty and, when warranted, patch augmentation of the main pulmonary artery. If there is significant hypoplasia of the pulmonic valve annulus, a transannular patch is placed. Surgery is usually done electively at age 2 to 6 months but can be done at any time if symptoms are present or right ventricular outflow tract obstruction is severe.
In some neonates with low birth weight or complex anatomy, initial palliation may be preferred to complete repair; the usual procedure is a modified Blalock-Taussig-Thomas shunt, in which the subclavian artery is connected to the ipsilateral pulmonary artery with a synthetic graft. More recently, transcatheter intervention to stent the right ventricular outflow tract or PDA has been used as an alternative palliative procedure with good outcomes (3).

Perioperative mortality rate for complete repair is < 5% for uncomplicated tetralogy of Fallot. For untreated patients, survival rates are 55% at 5 years and 30% at 10 years.
Endocarditis prophylaxis is recommended preoperatively but is required only for the first 6 months after repair unless there is a residual defect adjacent to a surgical patch or prosthetic material.
Treatment references
1. Montero JV, Nieto EM, Vallejo IR, et al: Intranasal midazolam for the emergency management of hypercyanotic spells in tetralogy of Fallot. Pediatr Emerg Care 31(4): 269–271, 2015.
2. Tsze DS, Vitberg YM, Berezow J, et al: Treatment of tetralogy of Fallot hypoxic spell with intranasal fentanyl. Pediatrics 134(1): e266–e269, 2014.
3. Sandoval JP, Chaturvedi RR, Benson L, et al: Right ventricular outflow tract stenting in tetralogy of Fallot infants with risk factors for early primary repair. Circ Cardiovasc Interv 9(12): pii: e003979, 2016.
Key Points
Tetralogy of Fallot involves a large ventricular septal defect (VSD), right ventricular outflow tract and pulmonary valve obstruction, and over-riding of the aorta.
Pulmonary blood flow is decreased, the right ventricle hypertrophies, and unoxygenated blood enters the aorta via the VSD.
Manifestations depend on the degree of right ventricle outflow obstruction; severely affected neonates have marked cyanosis, dyspnea with feeding, poor weight gain, and a harsh grade 3 to 5/6 systolic ejection murmur. The murmur comes from the pulmonary stenosis; the VSD shunt is silent.
Hypercyanotic spells are sudden episodes of profound cyanosis and hypoxia that may be triggered by a fall in oxygen saturation (eg, during crying, defecating), decreased systemic vascular resistance (eg, during playing, kicking legs), or sudden tachycardia or hypovolemia. The murmur diminishes or disappears during a spell.
Give neonates with severe cyanosis an infusion of prostaglandin E1 to open the ductus arteriosus.
Place infants with hypercyanotic spells in the knee-chest position and give oxygen; sometimes, opioids (morphine or fentanyl), volume expansion, sodium bicarbonate, beta-blockers (propranolol or esmolol), or phenylephrine may help. Place infants with hypercyanotic spells in the knee-chest position and give oxygen; sometimes, opioids (morphine or fentanyl), volume expansion, sodium bicarbonate, beta-blockers (propranolol or esmolol), or phenylephrine may help.
Repair surgically at 2 to 6 months or earlier if symptoms are severe.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers







