


Cystic fibrosis is an inherited disease of the exocrine glands affecting primarily the gastrointestinal and respiratory systems. It leads to chronic lung disease, exocrine pancreatic insufficiency, hepatobiliary disease, and abnormally high sweat electrolytes. Diagnosis is by sweat test or identification of 2 cystic fibrosis–causing gene variants in patients with a positive newborn screening test result or characteristic clinical features. Treatment is supportive through aggressive multidisciplinary care along with small-molecule correctors and potentiators targeting the cystic fibrosis transmembrane conductance regulator protein defect.
Cystic fibrosis (CF) is a life-threatening genetic disease, which in the United States occurs in about 1/3,300 White births, 1/15,300 Black births, and 1/32,000 Asian American births. There are approximately 40,000 people with CF living in the United States, and approximately 100,000 diagnosed with CF worldwide. Because of improved treatment and life expectancy, about 58% of patients in the United States with CF are now adults (1).
General reference
1. Cystic Fibrosis Foundation Patient Registry 2021 Annual Data Report Bethesda, Maryland 2022 Cystic Fibrosis Foundation. Accessed October 20, 2023.
Etiology of Cystic Fibrosis
Cystic fibrosis is carried as an autosomal recessive trait by about 3% of the White population. The responsible gene has been localized on the long arm of chromosome 7. It encodes a membrane-associated protein called the cystic fibrosis transmembrane conductance regulator (CFTR). The most common gene variant, F508del, occurs in about 85% of CF alleles; > 2000 less common CFTR variants have been identified.
CFTR is a cyclic adenosine monophosphate (cAMP)–regulated chloride channel, regulating chloride, sodium, and bicarbonate transport across epithelial membranes. A number of additional functions are considered likely. Disease manifests only in people who are homozygous. People who are heterozygous may show subtle abnormalities of epithelial electrolyte transport but are clinically unaffected.
The CFTR variants have been divided into 6 classes based on how the variant affects the function or processing of the CFTR protein. Patients with class I, II, or III variants are considered to have a more severe genotype that results in little or no CFTR function, whereas patients with 1 or 2 class IV, V, or VI variants are considered to have a milder genotype that results in residual CFTR function. However, there is no strict relationship between specific variants and disease manifestation, so clinical testing (ie, of organ function) rather than genotyping is a better guide to prognosis. CFTR variants can involve frameshift (a deletion or insertion in a DNA sequence that shifts the way a sequence is read) or nonsense (stop) mutations.

Pathophysiology of Cystic Fibrosis
Nearly all exocrine glands are affected in varying distribution and degree of severity. Glands may
Become obstructed by viscid mucus in the lumen (pancreas, intestinal glands, intrahepatic bile ducts, gallbladder, and submaxillary glands)
Appear histologically abnormal and produce excessive secretions (tracheobronchial and Brunner glands)
Appear histologically normal but secrete excessive sodium and chloride (sweat, parotid, and small salivary glands)
Respiratory
Although the lungs are generally histologically normal at birth, most patients develop signs of pulmonary disease beginning in infancy or early childhood. Mucus plugging and chronic bacterial infection, accompanied by a pronounced inflammatory response, damage the airways, ultimately leading to bronchiectasis and respiratory insufficiency. The course is characterized by episodic exacerbations with infection and progressive decline in pulmonary function.
Pulmonary damage is probably initiated by diffuse obstruction in the small airways by abnormally thick mucus secretions. Bronchiolitis and mucopurulent plugging of the airways occur secondary to obstruction and infection. Chronic inflammation secondary to the release of proteases and proinflammatory cytokines by cells in the airways also contributes to lung injury. Airway changes are more common than parenchymal changes, and emphysema is not prominent. About 50% of patients have bronchial hyperreactivity that may respond to bronchodilators.
In patients with advanced pulmonary disease, chronic hypoxemia results in muscular hypertrophy of the pulmonary arteries, pulmonary hypertension, and right ventricular hypertrophy.
The lungs of most patients are colonized by pathogenic bacteria. Early in the course, Staphylococcus aureus is the most common pathogen, but as the disease progresses, Pseudomonas aeruginosa, including multidrug-resistant strains, is frequently isolated. A mucoid variant of P. aeruginosa is uniquely associated with CF and results in a worse prognosis than nonmucoid P. aeruginosa.
In the United States, the prevalence of methicillin-resistant S. aureus (MRSA) in the respiratory tract is now about 25%; patients who are chronically infected with MRSA have more rapid decline in pulmonary function and lower survival rates than those who are not.
Colonization with Burkholderia cepacia complex occurs in about 2 to 3% of patients and may be associated with more rapid pulmonary deterioration.
Nontuberculous mycobacteria, including Mycobacterium avium complex and M. abscessus, are potential respiratory pathogens. Prevalence is around 14% and varies with age and geographic location. Differentiating infection from colonization can be challenging.
Other common respiratory pathogens include Stenotrophomonas maltophilia, Achromobacter xylosoxidans, and Aspergillus species.
Anaerobic bacteria and common respiratory viruses are frequently present in the respiratory tract of patients with CF, but their role in disease progression has not been well established.
Gastrointestinal
The pancreas, intestines, and hepatobiliary system are frequently affected. Exocrine pancreatic function is compromised in 85 to 95% of patients. An exception is a subset of patients who have certain CFTR variants with residual function, in whom pancreatic function is preserved. Patients with pancreatic insufficiency have malabsorption of fats, fat-soluble vitamins, and protein. Duodenal fluid is abnormally viscid and shows absence or diminution of enzyme activity and decreased bicarbonate concentration; stool trypsin and chymotrypsin are absent or diminished. Endocrine pancreatic dysfunction is less common, but impaired glucose tolerance or diabetes mellitus is present in about 2% of children, 20% of adolescents, and up to 50% of adults.
Bile duct involvement with bile stasis and biliary plugging leads to asymptomatic hepatic fibrosis in 30% of patients. About 3 to 4% of patients progress to irreversible multinodular biliary cirrhosis with varices and portal hypertension, usually by 12 years of age. Hepatocellular failure is a rare and late event. There is an increased incidence of cholelithiasis, which is usually asymptomatic.
Abnormally viscid intestinal secretions can cause meconium ileus in neonates and sometimes meconium plugging of the colon. Older children and adults also may have intermittent or chronic constipation and intestinal obstruction.
Other gastrointestinal (GI) problems include intussusception, volvulus, rectal prolapse, periappendiceal abscess, pancreatitis, an increased risk of cancer of the hepatobiliary tract and cancer of the GI tract (including of the pancreas), gastroesophageal reflux, esophagitis, and an increased prevalence of Crohn disease and celiac disease.
Other
Infertility occurs in 98% of adult men secondary to maldevelopment of the vas deferens or to other forms of obstructive azoospermia. In women, fertility is somewhat decreased secondary to viscid cervical secretions, although many women have carried pregnancies to term. Pregnancy outcome for both the mother and neonate is related to the mother's health.
Other complications include chronic rhinosinusitis, osteopenia/osteoporosis, depression and anxiety, chronic pain, obstructive sleep apnea, other sleep disorders, renal stones, dialysis-dependent chronic kidney disease (possibly related to treatments as well as to CF), iron deficiency anemia, sensorineural hearing loss and tinnitus caused by exposure to ototoxic medications (especially aminoglycosides), and episodic arthralgias/arthritis.
Symptoms and Signs of Cystic Fibrosis
Respiratory
Fifty percent of patients not diagnosed through newborn screening present with pulmonary manifestations, often beginning in infancy. Recurrent or chronic infections manifested by cough, sputum production, and wheezing are common. Cough is the most common chronic symptom, often accompanied by sputum production, vomiting, and disturbed sleep. Intercostal retractions, use of accessory muscles of respiration, a barrel-chest deformity, digital clubbing, cyanosis, and a declining tolerance for exercise occur with disease progression. Upper respiratory tract involvement includes nasal polyposis and chronic or recurrent rhinosinusitis.
Pulmonary complications include pneumothorax, nontuberculous mycobacterial infection, hemoptysis, allergic bronchopulmonary aspergillosis (ABPA), and right heart failure secondary to pulmonary hypertension.
Gastrointestinal
Meconium ileus due to obstruction of the ileum by viscid meconium may be the earliest sign and is present in about 10 to 20% of CF-affected neonates. It typically manifests with abdominal distention, vomiting, and failure to pass meconium. Some infants have intestinal perforation, with signs of peritonitis and shock. Infants with meconium plug syndrome have a delayed passage of meconium. They can have similar signs of obstruction or very mild and transient symptoms that go unnoticed. Older patients may have episodes of constipation or develop recurrent and sometimes chronic episodes of partial or complete small- or large-bowel obstruction (distal intestinal obstruction syndrome). Symptoms include crampy abdominal pain, change in stooling pattern, decreased appetite, and sometimes vomiting.
In infants without meconium ileus, disease onset may be heralded by a delay in regaining birth weight and inadequate weight gain at 4 to 6 weeks of age.
Occasionally, infants who are undernourished, especially if on hypoallergenic formula or soy formula, present with generalized edema secondary to protein malabsorption.
Pancreatic insufficiency is usually clinically apparent early in life and may be progressive. Manifestations include the frequent passage of bulky, foul-smelling, oily stools; abdominal protuberance; and poor growth pattern with decreased subcutaneous tissue and muscle mass despite a normal or voracious appetite. Clinical manifestations may occur secondary to deficiency of fat-soluble vitamins.
Rectal prolapse may occur in untreated infants and toddlers. Gastroesophageal reflux is relatively common among children and adults.
Other
Excessive sweating in hot weather or with fever may lead to episodes of hyponatremic/hypochloremic dehydration and circulatory failure. In arid climates, infants may present with chronic metabolic alkalosis. Salt crystal formation and a salty taste on the skin are highly suggestive of CF.
Adolescents may have retarded growth and delayed onset of puberty.
Diagnosis of Cystic Fibrosis
Newborn screening
May also be suggested by a positive prenatal screening test result, family history, or symptomatic presentation
Confirmed by a sweat test showing elevated sweat chloride on 2 occasions
Identifying 2 CF-causing variants (1 on each chromosome) is consistent with the diagnosis
May rarely be confirmed, in atypical cases, by demonstrating abnormal ion transport across the nasal epithelium or abnormal intestinal current measurements
Most cases of CF are first identified by newborn screening, but up to 10% are not diagnosed until adolescence or early adulthood. Despite advances in genetic testing, the sweat chloride test remains the standard for confirming a CF diagnosis in most cases because of its sensitivity and specificity, simplicity, and availability.
Newborn screening
Universal newborn screening for CF is now standard in the United States. Screening is based on detecting an elevated concentration of immunoreactive trypsinogen (IRT) in the blood.
There are 2 methods of following up on an elevated IRT level. In one method, a second IRT is done, which, if also elevated, is followed by a sweat test. In the other, more commonly used method, an elevated IRT level is followed by CFTR mutation testing, and, if 1 or 2 variants are identified, then a sweat test is done. For diagnosis, both methods have 90 to 95% sensitivity.
Sweat testing
In this test, localized sweating is stimulated with pilocarpine, the amount of sweat is measured, and the chloride concentration is determined. Although the sweat chloride concentration increases slightly with age, the sweat test is valid at all ages:In this test, localized sweating is stimulated with pilocarpine, the amount of sweat is measured, and the chloride concentration is determined. Although the sweat chloride concentration increases slightly with age, the sweat test is valid at all ages:
Normal: ≤ 30 mEq/L (≤ 30 mmol/L) (CF is unlikely.)
Intermediate: 30 to 59 mEq/L (30 to 59 mmol/L) (CF is possible.)
Abnormal: ≥ 60 mEq/L (≥ 60 mmol/L) (This result is consistent with CF.)
The results are valid after 48 hours of life, but an adequate sweat sample (> 75 mg on filter paper or > 15 mcL in microbore tubing) may be difficult to obtain before 2 weeks of age. False-negative results are rare but may occur in the presence of edema and hypoproteinemia or an inadequate quantity of sweat. False-positive results are usually due to technical error. Transient elevation of sweat chloride concentration can result from psychosocial deprivation (eg, child abuse, neglect) and can occur in patients with anorexia nervosa. A positive sweat test result should be confirmed by a second sweat test or by identification of 2 CF-causing variants.
Intermediate sweat test results
A small subset of patients have a mild or partial CF phenotype and sweat chloride values that are persistently in the intermediate or even normal range. In addition, there are patients who have single-organ manifestations such as chronic or recurrent pancreatitis, isolated bronchiectasis, or congenital bilateral absence of the vas deferens along with findings suggestive of abnormal CFTR function. They do not meet criteria for a CF diagnosis and are classified as having a CFTR-related disorder. In some of these patients, the diagnosis of CF can be confirmed by the identification of 2 CF-causing variants, 1 on each chromosome. If 2 CF-causing variants are not identified, ancillary evaluations such as pancreatic function testing and pancreatic imaging, high-resolution chest CT, sinus CT, pulmonary function testing, urogenital evaluation in males, and bronchoalveolar lavage including assessment of microbial flora may be useful.
Additional potentially helpful diagnostic tests include expanded CFTR genetic analysis and measurement of nasal transepithelial potential difference (based on the observation of increased sodium reabsorption across epithelium that is relatively impermeable to chloride in patients with CF) and measurement of intestinal currents.
CFTR-related metabolic syndrome and CF screen positive, inconclusive diagnosis
Infants who have a positive newborn screening result and evidence of possible CFTR dysfunction but do not meet the diagnostic criteria for CF are classified as having CFTR-related metabolic syndrome (CRMS), also called CF screen positive, inconclusive diagnosis (CFSPID). CRMS/CFSPID is diagnosed in infants who have a positive newborn screen, are asymptomatic, and have either of the following:
Sweat chloride concentrations in the intermediate range and 0 or 1 CF-causing variant
Sweat chloride concentrations in the normal range and 2 CFTR variants, at least 1 of which has unclear phenotypic consequences
Most children with CRMS/CFSPID remain healthy, but over time around 10% will develop symptoms and meet criteria for a diagnosis of CF or a CF-related disorder. Patients with CRMS/CFSPID should be evaluated and monitored regularly in a CF care center.
Pancreatic tests
Pancreatic function should be assessed at the time of diagnosis, usually by measuring the concentration of human pancreatic elastase in stool. Human pancreatic elastase measurement is valid even in the presence of exogenous pancreatic enzymes. Infants who are initially pancreatic sufficient and who carry 2 "severe" variants should have serial measurements to detect progression to pancreatic insufficiency.
Respiratory assessment
Chest imaging is done at times of pulmonary deterioration or exacerbations and routinely every 1 to 2 years. High-resolution chest CT may be helpful to more precisely define the extent of lung damage and to detect subtle airway abnormalities. Chest x-rays and CT may show hyperinflation, mucoid impaction, and bronchial wall thickening as the earliest findings. Subsequent changes include areas of infiltrate, atelectasis, and hilar adenopathy. With advanced disease, segmental or lobar atelectasis, cyst formation, bronchiectasis, and pulmonary artery and right ventricular hypertrophy occur. Branching, fingerlike opacifications that represent mucoid impaction of dilated bronchi are characteristic.
Sinus CT studies are indicated in patients with significant sinus symptoms or nasal polyps in whom endoscopic sinus surgery is being considered. These studies almost always show persistent opacification of the paranasal sinuses.


This chest x-ray shows right lower lobe collapse. Findings are typical for CF but not specific.
By permission of the publisher. From Berman L: Atlas of Anesthesia: Critical Care. Edited by R Miller (series editor) and RR Kirby. Philadelphia, Current Medicine, 1997.


This chest x-ray of a man with cystic fibrosis shows increased lung markings consistent with bronchiectasis.
PHOTOSTOCK-ISRAEL/SCIENCE PHOTO LIBRARY

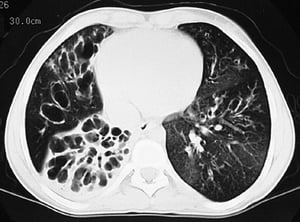
This CT scan shows greatly dilated bronchi throughout the lungs. Findings are typical for CF but not specific.
By permission of the publisher. From Berman L: Atlas of Anesthesia: Critical Care. Edited by R Miller (series editor) and RR Kirby. Philadelphia, Current Medicine, 1997.
This chest x-ray shows right lower lobe collapse. Findings are typical for CF but not specific.
By permission of the publisher. From Berman L: Atlas of Anesthesia: Critical Care. Edited by R Miller (series editor) and RR Kirby. Philadelphia, Current Medicine, 1997.
This chest x-ray of a man with cystic fibrosis shows increased lung markings consistent with bronchiectasis.
PHOTOSTOCK-ISRAEL/SCIENCE PHOTO LIBRARY
This CT scan shows greatly dilated bronchi throughout the lungs. Findings are typical for CF but not specific.
By permission of the publisher. From Berman L: Atlas of Anesthesia: Critical Care. Edited by R Miller (series editor) and RR Kirby. Philadelphia, Current Medicine, 1997.
Pulmonary function tests are the best indicators of clinical status and response to therapy. In patients over 5 years of age, spirometry should be done routinely and at times of clinical decline. In infants, respiratory status can be monitored by using a raised-volume rapid thoracoabdominal compression technique, which generates a partial flow-volume curve. In children 3 to 6 years of age, the multiple breath washout procedure can be used to generate a lung clearance index as a measure of ventilation inhomogeneity (1).
Pulmonary function tests done by spirometry indicate
A reduction in forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), forced expiratory flow between 25% and 75% expired volume (FEF25-75), and FEV1/FVC ratio
An increase in residual volume and the ratio of residual volume to total lung capacity
Fifty percent of patients have evidence of reversible airway obstruction as shown by improvement in pulmonary function after administration of an inhaled bronchodilator.
Screening oropharyngeal or sputum cultures should be done at least 4 times/year, especially in patients not yet colonized with P. aeruginosa. Bronchoscopy/bronchoalveolar lavage is indicated when it is important to precisely define the patient’s lower airway microbial flora (eg, to direct antibiotic selection) or to remove inspissated mucus plugs.
Carrier screening
CF carrier screening is available in the United States and is recommended for couples who are planning a pregnancy or seeking prenatal care. If both potential parents carry a CFTR variant, prenatal screening of the fetus can be done by chorionic villus sampling or amniocentesis. Prenatal counseling in such cases is complicated by the wide phenotypic variability of CF and incomplete information on the clinical consequences of many of the CFTR variants that are identified through screening.
Diagnosis reference
1. Stanojevic S, Davis SD, Retsch-Bogart G, et al: Progression of lung disease in preschool patients with cystic fibrosis. Am J Respir Crit Care Med 195:1216–1225, 2017. doi: 10.1164/rccm.201610-2158OC
Treatment of Cystic Fibrosis
Comprehensive, multidisciplinary support
Antibiotics, inhaled medications to thin airway secretions, and physical maneuvers to clear airway secretions
Inhaled bronchodilators and sometimes corticosteroids for responders
Usually pancreatic enzyme and vitamin supplementation
High-calorie diet (sometimes requiring supplemental enteral tube feedings)
In patients with specific variants, CFTR modulators consisting of a CFTR potentiator or combination of CFTR correctors and a CFTR potentiator
Comprehensive and intensive therapy should be directed by an experienced physician working with a multidisciplinary team that includes other physicians, nurses, dietitians, physical and respiratory therapists, mental health professionals, pharmacists, and social workers. The goals of therapy are maintenance of normal nutritional status, prevention or aggressive treatment of pulmonary and other complications, encouragement of physical activity, and provision of psychosocial support. The treatment regimen is complex and may take up to 2 hours each day. With appropriate support, most patients can make an age-appropriate adjustment at home and school.
(See also the Cystic Fibrosis Foundation's comprehensive treatment guidelines for all age groups.)
Treatment of respiratory manifestations
Treatment of pulmonary manifestations centers on prevention of airway obstruction and prophylaxis against and control of pulmonary infections. Prophylaxis against pulmonary infections includes maintenance of pertussis, Haemophilus influenzae, varicella, Streptococcus pneumoniae, and measles immunity; annual influenza vaccination; and COVID-19 vaccination in accordance with current recommendations from the Advisory Committee on Immunization Practices (ACIP). In patients exposed to influenza, a neuraminidase inhibitor can be used prophylactically or at the first signs of infection. Giving nirsevimab, or when not available, palivizumab, to infants with CF for from the Advisory Committee on Immunization Practices (ACIP). In patients exposed to influenza, a neuraminidase inhibitor can be used prophylactically or at the first signs of infection. Giving nirsevimab, or when not available, palivizumab, to infants with CF forprevention of respiratory syncytial virus infection has been shown to be safe, but efficacy has not been documented.
Long-term daily inhalation therapy with dornase alfa (recombinant human deoxyribonuclease) or with 7% hypertonic saline is recommended (Long-term daily inhalation therapy with dornase alfa (recombinant human deoxyribonuclease) or with 7% hypertonic saline is recommended (1, 2) and has been shown to slow the rate of decline in pulmonary function and to decrease the frequency of respiratory tract exacerbations (3).
Airway clearance measures consisting of postural drainage, percussion, vibration, and assisted coughing (chest physiotherapy) are recommended at the time of diagnosis and should be done on a regular basis. In older patients, alternative airway clearance measures, such as active cycle of breathing, autogenic drainage, positive expiratory pressure devices, and vest therapy (high-frequency chest wall oscillation), may be effective. Regular aerobic exercise is recommended; it may also help airway clearance. For patients with obstructive sleep apnea, continuous positive airway pressure may be beneficial.
For patients with reversible airway obstruction, bronchodilators may be given by inhalation. Corticosteroids by inhalation usually are not effective. Oxygen therapy is indicated for patients with severe pulmonary insufficiency and hypoxemia.
Mechanical ventilation or extracorporeal membrane oxygenation (ECMO) is typically not indicated for chronic respiratory failure. Their use is typically restricted to patients with good baseline status in whom acute reversible respiratory complications develop, in association with pulmonary surgery, or to patients in whom lung transplantation is imminent. Noninvasive positive pressure ventilation nasally or by face mask also can be beneficial.
Oral expectorants are sometimes used, but few data support their efficacy. Cough suppressants should be discouraged.
Pneumothorax can be treated with closed chest tube thoracostomy drainage. Open thoracotomy or thoracoscopy with resection of pleural blebs and mechanical abrasion of the pleural surfaces is effective in treating recurrent pneumothoraces.
Mild to moderate hemoptysis is treated with antibiotics (oral/aerosol or IV depending on severity of hemoptysis and severity of infection) and airway clearance. Massive or recurrent hemoptysis is treated by bronchial artery embolization or rarely by focal lung resection.
Oral corticosteroids are indicated in infants with prolonged bronchiolitis and in patients with refractory bronchospasm, allergic bronchopulmonary aspergillosis (ABPA), and inflammatory complications (eg, arthritis, vasculitis). Long-term use of alternate-day corticosteroid therapy can slow the decline in pulmonary function, but because of corticosteroid-related complications, it is not recommended for routine use. Patients receiving corticosteroids must be closely monitored for evidence of diabetes and linear growth retardation.
Allergic bronchopulmonary aspergillosis is also treated with systemic corticosteroids and an oral antifungal medication.
Ibuprofen, when given over several years at a dose sufficient to achieve a peak plasma concentration between 50 and 100 mcg/mL (242.4 and 484.8 micromol/L), has been shown to slow the rate of decline in pulmonary function, especially in children 5 to 13 years of age. The appropriate dose must be individualized based on pharmacokinetic studies.Ibuprofen, when given over several years at a dose sufficient to achieve a peak plasma concentration between 50 and 100 mcg/mL (242.4 and 484.8 micromol/L), has been shown to slow the rate of decline in pulmonary function, especially in children 5 to 13 years of age. The appropriate dose must be individualized based on pharmacokinetic studies.
Chronic rhinosinusitis is very common. Treatment options include nasal saline irrigation, low-pressure isotonic nasal irrigation, intranasal dornase alfa nebulization, and sinonasal topical antibiotics. Sinus surgery may be helpful in cases refractory to medical management. An intranasal corticosteroid spray is recommended to treat allergic rhinitis.Chronic rhinosinusitis is very common. Treatment options include nasal saline irrigation, low-pressure isotonic nasal irrigation, intranasal dornase alfa nebulization, and sinonasal topical antibiotics. Sinus surgery may be helpful in cases refractory to medical management. An intranasal corticosteroid spray is recommended to treat allergic rhinitis.
CFTR modulators
CFTR corrector and potentiator medications are indicated for about 90% of the variants carried by patients with CF. CFTR modulators are not available for patients with class I frameshift and nonsense mutations.
Ivacaftor is a small-molecule oral medication given chronically that potentiates the CFTR ion channel in patients with specific Ivacaftor is a small-molecule oral medication given chronically that potentiates the CFTR ion channel in patients with specificCFTR variants. It may be used in patients 1 month of age and older who carry at least 1 copy of a specific variant potentiated by ivacaftor.
Lumacaftor, tezacaftor, and elexacaftor are small-molecule oral medications that partially correct the defective CFTR protein by altering protein misfolding in patients who carry the F508del variant or other specified variants.
The combination of lumacaftor and ivacaftor can be given to patients 1 year of age and older who carry 2 copies of the F508del variant.
The combination of tezacaftor and ivacaftor can be given to patients 6 years of age and older who carry 2 copies of the F508del variant or other specified variants.
The triple combination of elexacaftor, tezacaftor, and ivacaftor can be given to patients 2 years of age and older who carry at least 1 copy of the F508del variant or 1 copy of certain rare variants (4, 5).
These medications can improve pulmonary function, increase weight, improve exocrine pancreatic function, decrease the frequency of pulmonary exacerbations and hospitalizations, improve quality of life, and reduce and sometimes normalize sweat chloride concentrations (6). The indications for ivacaftor, lumacaftor/ivacaftor, tezacaftor/ivacaftor, and elexacaftor/tezacaftor/ivacaftor are based on the patient's ). The indications for ivacaftor, lumacaftor/ivacaftor, tezacaftor/ivacaftor, and elexacaftor/tezacaftor/ivacaftor are based on the patient'sCFTR variants and age and are changing rapidly. Although all of these medications can be helpful, only ivacaftor and the combination of elexacaftor, tezacaftor, and variants and age and are changing rapidly. Although all of these medications can be helpful, only ivacaftor and the combination of elexacaftor, tezacaftor, andivacaftor are considered to be highly effective modulator therapy.
Treatment and prevention of infections
For mild pulmonary exacerbations, a short course of oral antibiotics should be given based on culture and sensitivity testing. The medications of choice for methicillin-sensitive staphylococcus are a penicillinase-resistant penicillin (eg, dicloxacillin), a cephalosporin (eg, cephalexin), or trimethoprim/sulfamethoxazole. Erythromycin, amoxicillin/clavulanate, a tetracycline, or linezolid may be used. For patients colonized with methicillin-resistant a short course of oral antibiotics should be given based on culture and sensitivity testing. The medications of choice for methicillin-sensitive staphylococcus are a penicillinase-resistant penicillin (eg, dicloxacillin), a cephalosporin (eg, cephalexin), or trimethoprim/sulfamethoxazole. Erythromycin, amoxicillin/clavulanate, a tetracycline, or linezolid may be used. For patients colonized with methicillin-resistantS. aureus (MRSA), a course of oral trimethoprim/sulfamethoxazole, clindamycin, linezolid, or a tetracycline may be effective. For patients colonized with /sulfamethoxazole, clindamycin, linezolid, or a tetracycline may be effective. For patients colonized withP. aeruginosa, a short course of inhaled tobramycin or aztreonam (eg, 4 weeks) and/or an oral fluoroquinolone (eg, 2 to 3 weeks) may be effective. Fluoroquinolones have been used safely in young children., a short course of inhaled tobramycin or aztreonam (eg, 4 weeks) and/or an oral fluoroquinolone (eg, 2 to 3 weeks) may be effective. Fluoroquinolones have been used safely in young children.
For moderate-to-severe pulmonary exacerbations, especially in patients colonized with P. aeruginosa, IV antibiotic therapy is advised. Patients often require hospital admission, but carefully selected patients can safely receive some of the therapy at home. Combinations of the aminoglycoside tobramycin (or sometimes amikacin) plus a cephalosporin, extended-spectrum penicillin, fluoroquinolone, or monobactam with antipseudomonal activity are given IV, usually for 2 weeks. Higher doses may be required to achieve acceptable serum concentrations. Because of enhanced renal clearance in patients with CF, large doses of some penicillins may be required to achieve adequate serum levels. For patients colonized with MRSA, vancomycin or linezolid can be added to the IV regimen. , IV antibiotic therapy is advised. Patients often require hospital admission, but carefully selected patients can safely receive some of the therapy at home. Combinations of the aminoglycoside tobramycin (or sometimes amikacin) plus a cephalosporin, extended-spectrum penicillin, fluoroquinolone, or monobactam with antipseudomonal activity are given IV, usually for 2 weeks. Higher doses may be required to achieve acceptable serum concentrations. Because of enhanced renal clearance in patients with CF, large doses of some penicillins may be required to achieve adequate serum levels. For patients colonized with MRSA, vancomycin or linezolid can be added to the IV regimen.
Eradication of chronic P. aeruginosa colonization is difficult. It has been shown, however, that early antibiotic treatment around the time the airways are initially infected with P. aeruginosa may be effective in eradicating the organism for some period of time. In patients who are chronically colonized with P. aeruginosa, antibiotics delivered by inhalation improve clinical parameters and possibly reduce the bacterial burden in the airways (7). The long-term use of alternate-month inhaled tobramycin or aztreonam therapy along with continuous (every month) oral azithromycin given 3 times a week may be effective in improving or stabilizing pulmonary function and decreasing the frequency of pulmonary exacerbations. ). The long-term use of alternate-month inhaled tobramycin or aztreonam therapy along with continuous (every month) oral azithromycin given 3 times a week may be effective in improving or stabilizing pulmonary function and decreasing the frequency of pulmonary exacerbations.
Patients who have a clinically significant nontuberculous mycobacterium infection may require long-term therapy with a combination of oral, inhaled, and IV antibiotics.
Patients with allergic bronchopulmonary aspergillosis (ABPA) or lower airways aspergillus infection may require prolonged oral or IV therapy with an antifungal azole and/or systemic corticosteroids.
Treatment of gastrointestinal manifestations
Neonatal intestinal obstruction can sometimes be relieved by enemas containing a hyperosmolar or iso-osmolar radiopaque contrast material; otherwise, surgical enterostomy to flush out the viscid meconium in the intestinal lumen may be necessary. After the neonatal period, episodes of partial intestinal obstruction (distal intestinal obstruction syndrome) can be treated with enemas containing a hyperosmolar or iso-osmolar radiopaque contrast material or acetylcysteine, or by oral administration of a balanced intestinal lavage solution. A stool softener such as dioctyl sodium sulfosuccinate (docusate) or lactulose may help prevent such episodes.Neonatal intestinal obstruction can sometimes be relieved by enemas containing a hyperosmolar or iso-osmolar radiopaque contrast material; otherwise, surgical enterostomy to flush out the viscid meconium in the intestinal lumen may be necessary. After the neonatal period, episodes of partial intestinal obstruction (distal intestinal obstruction syndrome) can be treated with enemas containing a hyperosmolar or iso-osmolar radiopaque contrast material or acetylcysteine, or by oral administration of a balanced intestinal lavage solution. A stool softener such as dioctyl sodium sulfosuccinate (docusate) or lactulose may help prevent such episodes.
Ursodeoxycholic acid, a hydrophilic bile acid, is often used in patients with liver disease caused by CF, but there is little evidence to support its efficacy in preventing progression from bile stasis to cirrhosis.Ursodeoxycholic acid, a hydrophilic bile acid, is often used in patients with liver disease caused by CF, but there is little evidence to support its efficacy in preventing progression from bile stasis to cirrhosis.
Pancreatic enzyme replacement should be given with all meals and snacks to patients with pancreatic insufficiency. The most effective enzyme preparations contain pancrelipase in pH-sensitive, enteric-coated microspheres or microtablets. For infants, the capsules are opened and the contents are mixed with acidic food. After infancy, weight-based dosing is used. Doses should be given with all meals and snacks to patients with pancreatic insufficiency. The most effective enzyme preparations contain pancrelipase in pH-sensitive, enteric-coated microspheres or microtablets. For infants, the capsules are opened and the contents are mixed with acidic food. After infancy, weight-based dosing is used. Doses> 2,500 IU lipase/kg/meal or > 10,000 IU lipase/kg/day should be avoided because high enzyme dosages have been associated with fibrosing colonopathy. In patients with high enzyme requirements, acid suppression with an H2 blocker or proton pump inhibitor may improve enzyme effectiveness.
Diet therapy includes sufficient calories and protein to promote normal growth—30 to 50% more than the usual recommended dietary allowances may be required (see table Recommended Dietary Reference Intakes for Some Macronutrients). Diet therapy also includes a normal-to-high total fat intake to increase the caloric density of the diet, a water-miscible multivitamin supplement in double the recommended daily allowance, supplementation with vitamin D3 (cholecalciferol) in patients with vitamin D deficiency or insufficiency, and salt supplementation during infancy and periods of thermal stress and increased sweating. Infants receiving broad-spectrum antibiotics and patients with liver disease and hemoptysis should be given additional supplemental vitamin K. Formulas containing protein hydrolysates and medium-chain triglycerides may be used instead of modified whole-milk formulas for infants with severe malabsorption. Glucose polymers and medium-chain triglyceride supplements can be used to increase caloric intake.
In patients who fail to maintain adequate nutritional status, enteral supplementation via gastrostomy or jejunostomy may improve growth and stabilize pulmonary function (see Overview of Nutritional Support). The use of appetite stimulants to enhance growth may be helpful in some patients.
Treatment of other manifestations
Cystic fibrosis–related diabetes (CFRD) is caused by insulin insufficiency and shares features of both type 1 and type 2 diabetes. Insulin is the only recommended treatment. Management includes an insufficiency and shares features of both type 1 and type 2 diabetes. Insulin is the only recommended treatment. Management includes aninsulin regimen, nutrition counseling, a diabetes self-management education program, and monitoring for microvascular complications. The plan should be carried out in conjunction with an endocrinologist and a dietitian with experience in treating both CF and diabetes.
Patients with symptomatic right heart failure should be treated with diuretics, salt restriction, and oxygen.
Recombinant human growth hormone (rhGH) may improve pulmonary function, increase height and weight and bone mineral content, and reduce the rate of hospitalization. However, because of the added cost and inconvenience, rhGH is not commonly used.
Surgery may be indicated for localized bronchiectasis or atelectasis that cannot be treated effectively with medications, nasal polyps, chronic rhinosinusitis, bleeding from esophageal varices secondary to portal hypertension, gallbladder disease, and intestinal obstruction due to a volvulus or an intussusception that cannot be medically reduced.
Liver transplantation has been done successfully in patients with end-stage liver disease.
Often, discussion of lung transplantation is needed. In considering transplantation, patients need to weigh the merits of longer survival with a transplant against the uncertainty of getting a transplant and the ongoing (but different) burden of living with an organ transplant. Bilateral cadaveric lung and live donor lobar transplantation has been done successfully in patients with advanced pulmonary disease. Combined liver-lung transplantation has been done for patients with end-stage liver and lung disease.
Bilateral lung transplantation for severe lung disease is becoming more routine and more successful with experience and improved techniques. Among adults with CF, median survival posttransplant is about 9 years.
Treatment references
1. Flume PA, O'Sullivan BP, Robinson KA, et al. Cystic fibrosis pulmonary guidelines: chronic medications for maintenance of lung health. Am J Respir Crit Care Med 2007;176(10):957-969. doi:10.1164/rccm.200705-664OC
2. Mogayzel PJ Jr, Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med 2013;187(7):680-689. doi:10.1164/rccm.201207-1160oe
3. Stahl M, Wielpütz MO, Ricklefs I, et al. Preventive Inhalation of Hypertonic Saline in Infants with Cystic Fibrosis (PRESIS). A Randomized, Double-Blind, Controlled Study. Am J Respir Crit Care Med 2019;199(10):1238-1248. doi:10.1164/rccm.201807-1203OC
4. Heijerman HGM, McKone EF, Downey DG, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial [published correction appears in Lancet 2020 May 30;395(10238):1694]. Lancet 2019;394(10212):1940-1948. doi:10.1016/S0140-6736(19)32597-8
5. Middleton PG, Mall MA, Dřevínek P, et al. Elexacaftor-Tezacaftor-Ivacaftor for Cystic Fibrosis with a Single Phe508del Allele. N Engl J Med 2019;381(19):1809-1819. doi:10.1056/NEJMoa1908639
6. Taylor-Cousar JL, Robinson PD, Shteinberg M, Downey DG. CFTR modulator therapy: transforming the landscape of clinical care in cystic fibrosis. Lancet 2023;402(10408):1171-1184. doi:10.1016/S0140-6736(23)01609-4
7. Mogayzel PJ Jr, Naureckas ET, Robinson KA, et al. Cystic Fibrosis Foundation pulmonary guideline. pharmacologic approaches to prevention and eradication of initial Pseudomonas aeruginosa infection. Ann Am Thorac Soc 2014;11(10):1640-1650. doi:10.1513/AnnalsATS.201404-166OC
Prognosis for Cystic Fibrosis
The course is largely determined by the degree of pulmonary involvement. Deterioration of pulmonary function over time, generally characterized by progressive bronchiectasis, leads to debilitation and eventually increases the risk for death, usually due to a combination of respiratory failure and cor pulmonale.
Prognosis has improved steadily over the past 5 decades, mainly because of early diagnosis and aggressive treatment before the onset of irreversible pulmonary changes. Median age at death in 2021 was 33.9 years. However, median predicted survival in the United States for children born in 2021 is age 65.6 years. Long-term survival is significantly better in patients without pancreatic insufficiency (1). Outcomes are also affected by CFTR variant profile, modifier genes, airway microbiology, sex, ambient temperature, exposure to air pollutants (including tobacco smoke), adherence to prescribed therapies, and socioeconomic status. The FEV1, adjusted for age and sex, is the best predictor of survival. If health outcomes with CFTR modulator therapy are sustained, life expectancy can potentially increase even further.
End-of-life care
Patients and their families deserve sensitive discussions of prognosis and preferences for care throughout the course of illness, especially if pulmonary function progressively declines.
One mark of respect for patients living with CF is to ensure that they are given the information and opportunity to make life choices, including having a substantial hand in determining how and when to accept dying.
When appropriate, palliative care, including sufficient symptom management, should be offered to ensure peaceful end-of-life care. A useful strategy for the patient to consider is to accept a time-limited trial of fully aggressive treatment when needed, but to agree in advance to parameters that indicate when to stop aggressive measures (see Do-Not-Resuscitate (DNR) Orders and Portable Medical Orders).
Prognosis reference
1. Cystic Fibrosis Foundation Patient Registry 2021 Annual Data Report Bethesda, Maryland 2022 Cystic Fibrosis Foundation. Accessed October 20, 2023.
Key Points
Cystic fibrosis is caused by carrying 2 variants of the gene for a protein called the cystic fibrosis transmembrane conductance regulator (CFTR), which regulates chloride, sodium, and bicarbonate transport across epithelial membranes.
The main complications involve the lungs, with damage to the small and large airways, chronic inflammation, and chronic and recurrent bacterial infections, particularly by Pseudomonas aeruginosa.
Other major consequences include pancreatic insufficiency, leading to malabsorption of nutrients and vitamins with consequent impaired growth and development, and, in older patients, a risk for developing diabetes.
Airway clearance measures (eg, postural drainage, percussion, vibration, assisted coughing), mucolytics, and airway hydrators are often started in early childhood; regular aerobic exercise is recommended.
Medications that correct or potentiate CFTR (CFTR modulators) can improve health outcomes for patients who have certain CFTR variants.
Antibiotics are given early in any pulmonary exacerbation; medication selection may be based on culture and sensitivity testing.
Diet should be supplemented with pancreatic enzymes, high-dose vitamins, and 30 to 50% more calories derived primarily from fat.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Cystic Fibrosis Foundation: Age-specific care guidelines for cystic fibrosis




