



Lung carcinoma is the leading cause of cancer-related death in men and women worldwide. About 85% of cases are related to cigarette smoking. Symptoms can include cough, chest discomfort or pain, weight loss, and, less commonly, hemoptysis; however, many patients present with metastatic disease with or without any clinical symptoms. The diagnosis is typically made by chest x-ray or CT and confirmed by biopsy. Depending on the stage of the disease, treatment includes surgery, chemotherapy, radiation therapy, or a combination. For the past several decades, the prognosis for a lung cancer patient was poor, with only 15% of patients surviving > 5 years from the time of diagnosis. For patients with stage IV (metastatic) disease, the 5-year overall survival rate was < 1%. However, outcomes have improved because of the identification of certain mutations that can be targeted for therapy, and current 5-year survival rates are 19% (23% for women and 16% for men).

")



In 2023, an estimated 238,340 new cases of lung cancer will be diagnosed in the United States (120,790 in women and 117,550 in men), and 127,070 people will die from the disease (1).
General reference
1. Siegel RL, Miller KD, Wagle NS, Jemal A: Cancer statistics, 2023. CA Cancer J Clin 73(1):17-48, 2023. doi:10.3322/caac.21763
Etiology of Lung Carcinoma
The most important cause of lung cancer, accounting for about 85% of cases, is
Cigarette smoking (1)
The risk of cancer differs by age, smoking intensity, and smoking duration.
The risk of lung cancer increases with combined exposure to toxins and cigarette smoking. Other confirmed or possible risk factors include air pollution, marijuana smoking, exposure to cigar smoke and second-hand cigarette smoke, and exposure to carcinogens (eg, asbestos, radiation, radon, arsenic, chromates, nickel, chloromethyl ethers, polycyclic aromatic hydrocarbons, mustard gas, coke-oven emissions, smoke from primitive cooking or heating fires in huts). The lung cancer risk associated with electronic nicotine delivery systems (eg, e-cigarettes) remains to be determined, although it is thought that the products of combustion of tobacco are the primary carcinogens.
The risk of cancer declines after smoking cessation, but it never returns to the baseline risk in people who have never smoked. About 15 to 20% of people who develop lung cancer have never smoked or have smoked minimally.
Exposure to household radon increases lung cancer risk and is the second leading cause of lung cancer in the United States (2).
Chronic inflammation increases the risk of many cancers, including lung cancer. For example, COPD (chronic obstructive pulmonary disease), alpha-1 antitrypsin deficiency, and pulmonary fibrosis increase susceptibility to lung cancer. People whose lungs are scarred by other lung diseases (eg, tuberculosis) are potentially at increased risk of lung cancer. Also, people who are active smokers and also take beta-carotene supplements may have an increased risk of developing lung cancer.

Genetic factors
Respiratory epithelial cells require prolonged exposure to cancer-promoting agents and accumulation of multiple genetic mutations before becoming neoplastic (an effect called field carcinogenesis).
In some patients with lung cancer, secondary or additional mutations in genes that stimulate cell growth (KRAS, MYC) or cause abnormalities in growth factor receptor signaling (EGFR, HER2) can contribute to the uncontrolled proliferation of abnormal cells.
In addition, mutations that inhibit tumor-suppressor genes (eg, TP53, APC) can lead to cancer. Other mutations that may be responsible include the EML4-ALK translocation and mutations in ROS1, BRAF, and PIK3CA.
Genes such as these that are primarily responsible for lung cancer are called oncogenic driver mutations. Although oncogenic driver mutations can cause or contribute to lung cancer among people who smoke, these mutations are particularly likely to be a cause of lung cancer among people who have never smoked. In 2014, the Lung Cancer Mutation Consortium (LCMC) found driver mutations in 64% of 733 lung cancers. This group included people who smoke and people who do not smoke (25% KRAS mutations, 17% EGFR mutations, 8% EML-4-ALK mutations, and 2% BRAF mutations [3]). The second LCMC study accrued 904 patients with stage IV lung cancer who had at least one 14 cancer-related gene tested for and found that oncogenic driver mutations were present in more than half of the patients with adenocarcinoma and that targeted therapies improved survival (4). Additional mutations are being reported, and novel therapies aimed at oncogenic driver mutations are an area of active research.
Etiology references
1. Division of Cancer Prevention and Control, Centers for Disease Control and Prevention: What Are the Risk Factors for Lung Cancer? Reviewed October 25, 2022. Accessed April 24, 2023
2. U.S. Cancer Statistics Working Group: U.S. Cancer Statistics Data Visualizations Tool, based on 2021 submission data (1999-2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; https://www.cdc.gov/cancer/dataviz, released in November 2022
3. Kris MG, Johnson BE, Berry LD, et al: Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA 311 (19):1998–2006, 2014. doi: 10.1001/jama.2014.3741
4. Aisner DL, Sholl LM, Berry LD, et al: The Impact of Smoking and TP53 Mutations in Lung Adenocarcinoma Patients with Targetable Mutations-The Lung Cancer Mutation Consortium (LCMC2). Clin Cancer Res 24(5):1038-1047, 2018. doi:10.1158/1078-0432.CCR-17-2289
Classification of Lung Carcinoma
Lung cancer is classified into 2 major categories:
Small cell lung cancer (SCLC), about 15% of cases
Non–small cell lung cancer (NSCLC), about 85% of cases
SCLC is highly aggressive and almost always occurs in people who smoke. It is rapidly growing, and roughly 80% of patients have metastatic disease at the time of diagnosis.
The clinical behavior of NSCLC is more variable and depends on histologic type, but about 40% of patients will have metastatic disease outside of the chest at the time of diagnosis. Oncogenic driver mutations have been identified primarily in adenocarcinoma, and attempts are being made to identify similar mutations in squamous cell carcinoma (eg, KRAS, EGFR, FGFR1, DDR2, PIK3CA).
Other features of the 2 categories (eg, location, risks, treatment, complications) also vary (see table Features of Lung Cancer).
Features of Lung Cancer
Feature | Small Cell | Non–Small Cell | ||
|---|---|---|---|---|
Adenocarcinoma | Squamous Cell | Large Cell | ||
% of lung cancers | 13–15% | 35–40% | 25–30% | 10–15% |
Location | Submucosa of airways, perihilar mass | Peripheral nodule or mass | Central, endobronchial | Peripheral nodule or mass |
Risk factors | Smoking | Smoking (for 80‒85% of patients; 15‒20% never smoked or smoked only minimally); patients particularly those who never smoked often have oncogenic driver mutations Environmental and occupational exposures (mainly to radon, asbestos, radiation, secondhand smoke, polycyclic aromatic hydrocarbons, arsenic, chromates, or nickel) | ||
Treatment | Etoposide plus cisplatin or carboplatinEtoposide plus cisplatin or carboplatin Sometimes irinotecan or topotecan rather than etoposide in extensive-stage diseaseSometimes irinotecan or topotecan rather than etoposide in extensive-stage disease Immunotherapy for extensive stage SCLC Concurrent radiation therapy in limited-stage disease No role for surgery unless patient presented with a solitary pulmonary nodule without apparent lymph node or distant spread | Stage I and II: Surgery with or without neoadjuvant or adjuvant chemotherapy; many trials are examining neoadjuvant (chemotherapy +/- immunotherapy) followed by definitive surgical resection Stage IIIA: Choice of therapy depends on the extent and localization of disease and may include: surgery with adjuvant therapy (chemotherapy and/or radiation therapy); neoadjuvant therapy (chemotherapy and/or radiation therapy) followed by surgery if there is a response; chemotherapy plus radiation therapy without surgery; immunotherapy is typically added to these regimens Stage IIIB: Radiation therapy and/or chemotherapy; immunotherapy may be added Stage IV: Systemic targeted therapy, chemotherapy, or immunotherapy —each with or without palliative radiation therapy Factors that influence the treatment modality and sequence of therapies include histology (adenocarcinoma vs squamous vs other), presence of driver mutations, PD-L1 expression (for immunotherapy), and patient-specific factors (age, co-morbid diseases, treatment preferences) Advanced NSCLC generally requires the sequential use of multiple systemic therapies (chemotherapy, radiation therapy, immunotherapy, targeted (biologic) therapy to improve overall survival | ||
Complications | SVC syndrome Paraneoplastic syndromes | Hemoptysis, airway obstruction, pneumonia, pleuritic involvement with pain, pleural effusion, SVC syndrome, Pancoast tumor (causing shoulder or arm pain), hoarseness due to laryngeal nerve involvement, neurologic symptoms due to brain metastasis, pathologic fractures due to bone metastasis, jaundice due to liver metastasis | ||
5-year survival with treatment | Limited: 20% Extensive: < 1% | Stage I: 68–92% Stage II: 53–65% Stage III: 12–41% Stage IV: 0–10% | ||
Non-small cell lung cancer survival data derived from Goldstraw P, Chansky K, Crowley J, et al: The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 11(1):39-51, 2016. doi:10.1016/j.jtho.2015.09.009 | ||||
NSCLC = non–small cell lung cancer; PD-L1 = programmed death-ligand 1; SCLC = small cell lung cancer; SVC = superior vena cava. | ||||
Symptoms and Signs of Lung Carcinoma
About 25% of lung cancers are asymptomatic and are detected incidentally with chest imaging obtained for another reason. Symptoms and signs can result from local tumor progression, regional spread, or distant metastases. Paraneoplastic syndromes and constitutional symptoms may occur at any stage of the disease. Although symptoms are not specific to the classification or histology of the cancer, certain complications may be more likely with different types (see table Features of Lung Cancer).
Local tumor
The local tumor can cause cough. Less commonly, local tumor causes dyspnea due to airway obstruction, postobstructive atelectasis, or pneumonia and parenchymal loss due to lymphangitic spread. Fever may occur with postobstructive pneumonia. Up to half of patients report vague or localized chest pain. Hemoptysis is less common, and blood loss is minimal, except in rare instances when the tumor erodes into a major artery, causing massive hemorrhage and often death by asphyxiation or exsanguination. Hemoptysis is the presenting symptom in about 10% of patients; 20% of patients experience it during the course of their illness.
Regional spread
Regional spread of tumor may cause pleuritic chest pain or dyspnea due to development of a pleural effusion, hoarseness due to tumor encroachment on the recurrent laryngeal nerve, and dyspnea and hypoxia from diaphragmatic paralysis due to involvement of the phrenic nerve.
Superior vena cava (SVC) syndrome results from compression or invasion of the SVC and can cause headache or a sensation of head fullness, facial or upper-extremity swelling, breathlessness when supine, dilated veins in the neck, face, and upper trunk, and facial and truncal flushing (plethora).
Pancoast syndrome occurs when apical tumors, usually NSCLC (Pancoast tumor), invade the brachial plexus, pleura, or ribs, causing shoulder and upper-extremity pain and weakness or atrophy of the ipsilateral hand. Pancoast syndrome can also include Horner syndrome.
Horner syndrome results when the paravertebral sympathetic chain or the cervical stellate ganglion is involved, causing ptosis, miosis, and anhidrosis.
Spread of the tumor to the pericardium may be asymptomatic or lead to constrictive pericarditis or cardiac tamponade.
In rare cases, esophageal compression by the tumor leads to dysphagia.


© Springer Science+Business Media
Metastases
Metastases eventually cause symptoms that vary by location. Metastases can spread to the
Liver, causing pain, nausea, early satiety, and ultimately hepatic insufficiency
Brain, causing behavioral changes, confusion, aphasia, seizures, paresis or paralysis, nausea and vomiting, and ultimately coma and death
Bones, causing severe pain and pathologic fractures
Adrenal glands, rarely causing adrenal insufficiency
Paraneoplastic syndromes
Paraneoplastic syndromes are symptoms that occur at sites distant from a tumor or its metastases. Common paraneoplastic syndromes in patients with lung cancer include
Hypercalcemia (in patients with squamous cell carcinoma, which results from the tumor producing parathyroid hormone–related protein, or because of extensive bone metastases that cause production of osteoclast-activating factors )
Syndrome of inappropriate antidiuretic hormone (SIADH) secretion
Finger clubbing with or without hypertrophic pulmonary osteoarthropathy
Hypercoagulability with migratory superficial thrombophlebitis (Trousseau syndrome)
Myasthenia-like symptoms (Eaton-Lambert syndrome)
Various other neurologic syndromes
Other neurologic syndromes include neuropathies, encephalopathies, encephalitides, myelopathies, and cerebellar disease. Mechanisms for neuromuscular syndromes involve tumor expression of autoantigens with production of autoantibodies, but the cause of most other syndromes is unknown.
Diagnosis of Lung Carcinoma
Chest x-ray
CT or combined positron emission tomography (PET)–CT
Cytopathology examination of pleural fluid or sputum
Bronchoscopy-guided or percutaneous transthoracic biopsy and core biopsy
Sometimes surgical lung biopsy
Imaging
Chest x-ray is often the initial imaging test. It may show clearly defined abnormalities, such as a single mass, multifocal masses, a solitary pulmonary nodule, an enlarged hilum, a widened mediastinum, tracheobronchial narrowing, atelectasis, nonresolving parenchymal infiltrates, cavitary lesions, or unexplained pleural thickening or effusion. These findings are suggestive but not diagnostic of lung cancer and require follow-up with CT scans or combined PET–CT scans and cytopathologic confirmation.

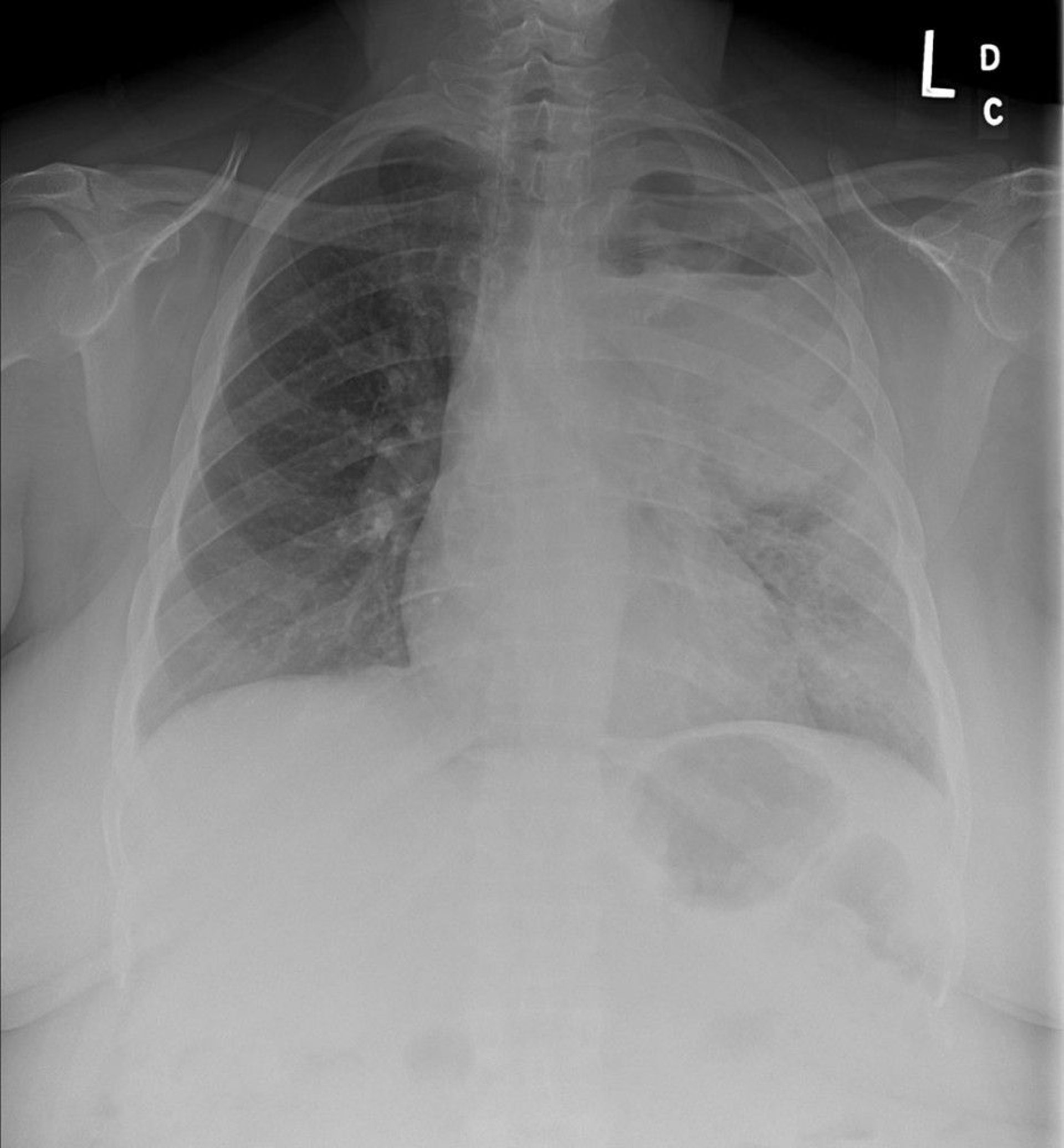
Image courtesy of Anne S. Tsao, MD.
CT shows many characteristic anatomic patterns and appearances that may strongly suggest the diagnosis. If a lesion found on a plain x-ray is highly suggestive of lung cancer (ie, based on risk factors such as age, tobacco use, symptoms), PET–CT may be done to assist in directing the diagnostic evaluation and staging. This study combines anatomic imaging from CT with functional imaging from PET. The PET images can help differentiate inflammatory and malignant processes. Both CT and PET–CT can help direct core needle biopsy of lesions not amenable to bronchoscopic biopsy. These PET images may also detect regional or distant metastatic disease.
Cytology
The method used to obtain cells or tissue for confirmation depends on the accessibility of tissue and the location of lesions. Cytology of a sputum or pleural fluid sample is the least invasive method to confirm lung cancer diagnosis.
In patients with productive cough, sputum specimens obtained on awakening may contain high concentrations of malignant cells, but yield for this method is < 50% overall.
Pleural fluid is another convenient source of cells; a malignant effusion is a poor prognostic sign and indicates advanced stage disease.
In general, false-negative cytology readings can be minimized by obtaining as large a volume of sputum or pleural fluid as possible early in the day (for sputum samples) and sending the sample to the pathology laboratory immediately to minimize delays in processing because such delays lead to cell breakdown.
Molecular (genetic) studies can be done on paraffin-embedded tumor cell pellets from pleural fluid if the fluid is spun down and the cell pellet preserved in a timely fashion.
Procedures
Percutaneous biopsy is the next least invasive procedure. It is more useful for metastatic sites (eg, supraclavicular or other peripheral lymph nodes, pleura, liver, adrenals) than for lung lesions. Risks include a 20 to 25% chance of pneumothorax (primarily in patients with significant emphysema) and the risk of obtaining a false-negative result.
A core biopsy is preferable to a fine-needle biopsy because the latter retrieves too little tissue for accurate genetic studies.
Bronchoscopy is the procedure most often used for diagnosing lung cancer. In theory, the procedure of choice for obtaining tissue is the one that is least invasive; however, in practice, bronchoscopy is often done in addition to or instead of less invasive procedures because diagnostic yields are greater and because bronchoscopy is also important for staging. A combination of washings, brushings, and biopsies of visible endobronchial lesions and of paratracheal, subcarinal, mediastinal, and hilar lymph nodes often yields a tissue diagnosis.
Advances in techniques to guide the bronchoscope have increased the diagnostic yield and the accuracy of sampling more peripheral lesions. Endobronchial ultrasound-guided biopsy (EBUS) can be done during bronchoscopy and has an excellent yield. EBUS is currently the preferred method for staging the mediastinum, except in cases where the lymph nodes cannot be sampled due to anatomic considerations. Navigational bronchoscopy is also used to sample more peripheral lesions with improved diagnostic accuracy. Robotic bronchoscopy is also being implemented at certain centers to improve the diagnostic yield and limit the number of thoracic surgical procedures.
Mediastinoscopy had been the standard test for evaluating mediastinal lymph nodes but is a higher risk procedure that is typically used before more extensive thoracic surgical procedures to confirm or exclude the presence of tumor in those few patients with enlarged mediastinal lymph nodes that cannot be sampled by EBUS.
Surgical lung biopsy, done via open thoracotomy or using video or robotic assistance, is indicated when less invasive methods do not provide a diagnosis in patients whose clinical characteristics and radiographic features strongly suggest that the tumor is resectable.
Staging of Lung Carcinoma
SCLC has 2 stages:
Limited
Extensive
Limited-stage SCLC disease is cancer confined to one hemithorax (including ipsilateral lymph nodes) that can be encompassed within one tolerable radiation therapy port, unless there is a pleural or pericardial effusion.
Extensive-stage disease is cancer outside a single hemithorax or the presence of malignant cells detected in pleural or pericardial effusions. Less than one third of patients with SCLC will present with limited-stage disease; the remainder of patients often have extensive distant metastases.
NSCLC has 4 stages, I through IV (using the TNM system). TNM staging is based on tumor size, tumor and lymph node location, and the presence or absence of distant metastases (see table International Staging System for Lung Cancer).
Tests for initial evaluation and staging
Some components of staging are part of the typical diagnostic evaluation, for example, endobronchial ultrasound-guided biopsy (EBUS) can be used to sample enlarged lymph nodes at the same time a lung lesion is biopsied.
All lung cancer patients need imaging to determine whether the disease has spread. Different combinations of tests can be done. Some tests are done routinely, and others are done depending on whether the results would impact treatment decisions:
PET or integrated PET–CT
CT from neck to pelvis and bone scan (done if PET–CT is not available)
MRI of chest (for tumors near apex or diaphragm to evaluate vascular supply)
Biopsy of questionable nodes (if PET is indeterminate)
Head CT or brain MRI
PET scanning is a reasonably accurate, noninvasive test used to identify malignant mediastinal lymph nodes and other distant metastases (metabolic staging). Integrated PET–CT scanning, in which PET and CT images are combined into a single image by scanners in a single gantry, is more accurate for NSCLC staging than CT or PET alone or than visual correlation of the 2 tests. The use of PET and integrated PET–CT is limited by cost, availability, and specificity (ie, the test is quite sensitive and has an excellent negative predictive value, but its positive predictive value is not as high). PET-CT may be used after a procedure such as bronchoscopy or needle biopsy fails to make a diagnosis when clinical suspicion for lung cancer remains high.
If PET–CT is not available, thin-section high-resolution CT (HRCT) from the neck to the upper abdomen (to detect cervical and supraclavicular and hepatic and adrenal metastases) is one of the first staging tests for both SCLC and NSCLC. However, CT often cannot distinguish postinflammatory changes from malignant intrathoracic lymph node enlargement or benign lesions from malignant hepatic or adrenal lesions (distinctions that determine stage). Thus, other tests are usually done when abnormalities are present in these areas.
When PET scan results are indeterminate, bronchoscopy with endobronchial ultrasonography, mediastinoscopy, or video-assisted thoracoscopic surgery (VATS) can be used to biopsy questionable mediastinal lymph nodes. Without PET scanning, hepatic or adrenal lesions must be evaluated by needle biopsy.
MRI of the chest is slightly more accurate than high-chest HRCT for staging apical (Pancoast) tumors and cancers close to the diaphragm (eg, mesothelioma) and provides an evaluation of the vasculature surrounding the tumors. MRI can also help determine if surgical resection can be considered.
Blood tests are usually done. Calcium and alkaline phosphatase levels, if elevated, suggest possible bone metastases. Other blood tests, such as complete blood count, aspartate aminotransferase, alanine aminotransferase, total bilirubin, electrolytes, serum albumin, and creatinine levels, have no role in staging but provide important prognostic information about the patient’s ability to tolerate treatment and may demonstrate the presence of paraneoplastic syndromes.
After diagnosis, all patients with lung cancer should undergo brain imaging; MRI is preferred to CT. Brain imaging is especially necessary in patients with headache or neurologic abnormalities.
Patients with bone pain or elevated serum calcium or alkaline phosphatase levels should undergo PET–CT or radionuclide bone scanning if PET–CT is not available.
International Staging System for Lung Cancer
Category | Description | |
|---|---|---|
Primary tumor (T) | ||
Tis | Carcinoma in situ | |
T1 | Tumor ≤ 3 cm without invasion more proximal than the lobar bronchus | |
T1mi | Minimally invasive adenocarcinoma | |
T1a | Tumor ≤ 1 cm | |
T1b | Tumor > 1 cm but ≤ 2 cm | |
T1c | Tumor > 2 cm but ≤ 3 cm | |
T2 | Tumor > 3 cm but ≤ 5 cm or with any of the following:
| |
T2a | Tumor > 3 but ≤ 4 cm | |
T2b | Tumor > 4 but ≤ 5 cm | |
T3 | Tumor > 5 cm but ≤ 7 cm or with any of the following:
| |
T4 | Tumor > 7 cm or with either of the following:
| |
Regional lymph nodes (N) | ||
N0 | No regional lymph node metastasis | |
N1 | Metastasis to ipsilateral peribronchial or ipsilateral hilar lymph node or both and to intrapulmonary nodes, including that by direct extension of the primary tumor | |
N2 | Metastasis to ipsilateral mediastinal or subcarinal lymph node or both | |
N3 | Metastasis to contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node or a combination | |
Distant metastasis (M) | ||
M0 | No distant metastasis | |
M1 | Distant metastasis | |
M1a | Tumor with any of the following:
| |
M1b | Single extrathoracic metastasis in a single organ | |
M1c | Multiple extrathoracic metastases in one or several organs | |
Stage groupings | ||
| ||
Adapted from American Joint Committee on Cancer (AJCC): AJCC Cancer Staging Form Supplement updated June 5, 2018, accessed online 2020 and Detterbeck FC: The eighth edition TNM stage classification for lung cancer: What does it mean on main street? J Thorac Cardiovasc Surg 155:356–359, 2018. doi: 10.1016/j.jtcvs.2017.08.138 | ||
Screening for Lung Cancer
Screening for lung cancer benefits patients with early disease, especially early NSCLC treatable with surgical resection, and is recommended in high-risk populations. A large study (1) has shown that annual screening using low-dose helical CT (LDCT) resulted in a 20% decrease in lung cancer deaths compared to screening using chest x-ray. The study defined the high-risk population as people who formerly or are currently smoking (mainly ages 55 to 74) with at least 30 pack-years of cigarette smoking, and, if they are no longer smoking, had quit within the previous 15 years). A recent study of screening in high-risk patients showed improved survival in patients receiving LDCT screening based on nodule volume and volume-doubling time (2). However, screening LDCT may not be appropriate for patients not at high risk.
The U.S. Preventive Services Task Force (USPSTF) updated the recommendations for annual LDCT screening of asymptomatic people age 50 to 80 years with a ≥ 20 pack-year history who currently smoke or have quit for less than 15 years (3). Shared decision making discussions between a clinician and the patient should occur before screening. Shared decision making regarding screening should include discussions to exclude patients who would not benefit from early detection, such as those who would refuse treatment or be unable to complete treatment due to other serious medical conditions. Additionally, it is recommended that LDCT screening be done at facilities with demonstrated LDCT proficiency and adherence to established protocols for follow-up diagnosis and treatment.
In the future, lung cancer screening may involve some combination of molecular analysis for genetic markers (eg, KRAS, TP53, EGFR), sputum cytometry, and detection of cancer-related volatile organic compounds (eg, alkane, benzene) in exhaled breath.
Screening references
1. National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al: Reduced lung-cancer mortality with low-dose computed tomographic screening. New Engl J Med 365 (5):395–409, 2011. doi: 10.1056/NEJMoa1102873.
2. de Koning HJ, van der Aalst CM, de Jong PA, et al: Reduced lung-cancer mortality With volume CT screening in a randomized trial. New Engl J Med 382:503–513, 2020. doi: 10.1056/NEJMoa1911793
3. US Preventive Services Task Force: Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. JAMA 325(10):962-970, 2021. doi: 10.1001/jama.2021.1117
Treatment of Lung Carcinoma
Surgery (depending on cell type and stage)
Chemotherapy
Radiation therapy
Immunotherapy
Treatment of lung cancer varies by cell type and by stage of disease. Many patient factors not related to the tumor affect treatment choice. Poor cardiopulmonary reserve, undernutrition, frailty or poor physical performance status (assessed by, eg, Karnofsky performance status [KPS] or Eastern Cooperative Oncology Group performance status [ECOGPS]), comorbidities, including cytopenias, and psychiatric or cognitive illness all may lead to a decision for palliative over curative treatment or for no treatment at all, even though a cure with aggressive therapy might technically be possible.
Radiation therapy carries the risk of radiation pneumonitis when large areas of the lung are exposed to high doses of radiation over time. Radiation pneumonitis can occur from 1 to 12 months after treatment is completed. Cough, dyspnea, low-grade fever, or pleuritic chest pain may signal the condition, as may crackles or a pleural friction rub detected on chest auscultation. Chest x-ray may have nonspecific findings; CT may show a nonspecific infiltrate without an obvious mass. The diagnosis is often one of exclusion. Radiation pneumonitis can be treated with a corticosteroid taper over several weeks and bronchodilators for symptom relief.
Radiofrequency ablation, in which high-frequency electrical current is used to destroy tumor cells, is a technique that can sometimes be used in patients who have small, early-stage tumors or small tumors that have recurred in a previously irradiated chest. This procedure may preserve more lung function than open surgery does and, because it is less invasive, may be appropriate for patients who are not candidates for open surgery.
Immunotherapy harnesses the body's immune system to eliminate the cancer, and is used to treat advanced stage (IV) non-small cell lung cancer if there is high programmed cell death protein 1 (PD-1) or PDL-1 expression (see table Some Targeted Therapy Drugs for Non–Small Cell Lung Cancer).
SCLC
SCLC of any stage is typically initially responsive to treatment, but responses are usually short-lived. Chemotherapy, with or without radiation therapy, is given depending on the stage of disease. Immunotherapy may also be used in extensive SCLC. In many patients, chemotherapy prolongs survival and improves quality of life enough to warrant its use. Surgery generally plays no role in treatment of SCLC, although it may be curative in the rare patient who has a small focal tumor without spread (such as a solitary pulmonary nodule) who underwent surgical resection before the tumor was identified as SCLC.
Pearls & Pitfalls
|
Chemotherapy regimens of etoposide and a platinum compound (either cisplatin or carboplatin) are commonly used, as are other drugs, such as irinotecan, topotecan, vinca alkaloids (vinblastine, vincristine, vinorelbine), alkylating agents (cyclophosphamide, ifosfamide), doxorubicin, taxanes (docetaxel, paclitaxel), and gemcitabine. Chemotherapy regimens of etoposide and a platinum compound (either cisplatin or carboplatin) are commonly used, as are other drugs, such as irinotecan, topotecan, vinca alkaloids (vinblastine, vincristine, vinorelbine), alkylating agents (cyclophosphamide, ifosfamide), doxorubicin, taxanes (docetaxel, paclitaxel), and gemcitabine.
In limited-stage disease, when disease is confined to a hemithorax, radiation therapy further improves clinical outcomes; such response to radiation therapy was the basis for the definition of limited-stage disease. The use of prophylactic cranial irradiation to prevent brain metastases is also advocated in certain cases; micrometastases are common in SCLC, and chemotherapy has less ability to cross the blood-brain barrier.
In extensive-stage disease, treatment is based on chemotherapy rather than radiation therapy, although radiation therapy is often used as palliative treatment for metastases to bone or brain. In patients with an excellent response to chemotherapy, prophylactic cranial irradiation is sometimes used as in limited-stage SCLC to prevent growth of SCLC in the brain. In rare, selected patients who have a near-complete response to chemotherapy, thoracic radiation therapy is sometimes thought to improve disease control. It is unclear whether replacing etoposide with topoisomerase inhibitors (irinotecan or topotecan) improves survival. These drugs alone or in combination with other drugs are also commonly used in refractory disease and in cancer of either stage that has recurred. Immunotherapy may also be used in extensive SCLC.treatment is based on chemotherapy rather than radiation therapy, although radiation therapy is often used as palliative treatment for metastases to bone or brain. In patients with an excellent response to chemotherapy, prophylactic cranial irradiation is sometimes used as in limited-stage SCLC to prevent growth of SCLC in the brain. In rare, selected patients who have a near-complete response to chemotherapy, thoracic radiation therapy is sometimes thought to improve disease control. It is unclear whether replacing etoposide with topoisomerase inhibitors (irinotecan or topotecan) improves survival. These drugs alone or in combination with other drugs are also commonly used in refractory disease and in cancer of either stage that has recurred. Immunotherapy may also be used in extensive SCLC.
In general, recurrent SCLC carries a poor prognosis, although patients who maintain a good performance status should be offered further treatment in a clinical trial.
NSCLC
Treatment for NSCLC typically involves assessment of eligibility for surgery followed by choice of surgery, chemotherapy (including targeted therapy and immunotherapy), radiation therapy, or a combination of modalities as appropriate, depending on tumor type and stage.
For stage I and II disease, the standard approach is surgical resection with either lobectomy or pneumonectomy combined with mediastinal lymph node sampling or complete lymph node dissection. Lesser resections, including segmentectomy and wedge resection, are considered for patients with poor pulmonary reserve. Surgery is curative in about 55 to 70% of patients with stage I and in 35 to 55% of patients with stage II disease. Outcomes appear better when surgical resection is done by a thoracic oncologic surgeon with expertise in lung cancer (1, 2). Patients with early-stage disease for whom surgery is high risk may instead have local, non-surgical treatment, such as radiation therapy (stereotactic or conventional) or radiofrequency ablation.
Preoperative pulmonary function is assessed. Surgery is done only if patients with NSCLC will have adequate pulmonary reserve once a lobe or lung is resected. Patients with preoperative forced expiratory volume in 1 second (FEV1) > 2 L generally tolerate pneumonectomy. Patients with FEV1 < 2 L should have a quantitative xenon radionuclide perfusion scan to determine the proportion of function they can expect to lose as a result of resection. Postoperative FEV1 can be predicted by multiplying percent perfusion of the nonresected lung by the preoperative FEV1. A predicted FEV1 > 800 mL or > 40% of the predicted normal FEV1 suggests adequate postoperative lung function, although studies of lung volume reduction surgery in patients with COPD (chronic obstructive pulmonary disease) suggest that patients with FEV1 < 800 mL can tolerate resection if the cancer is located in poorly functional, bullous (generally apical) lung regions.
Neoadjuvant (preoperative) chemotherapy in early-stage NSCLC is also commonly used and consists of 4 cycles of a cisplatin-doublet (combination of a cisplatin and another chemotherapy drug, such as vinorelbine, docetaxel, paclitaxel). In patients who cannot receive cisplatin, carboplatin can be substituted. Combining neoadjuvant chemotherapy and immunotherapy is an area of active investigation; the treatment is well tolerated in certain populations and improves survival.in early-stage NSCLC is also commonly used and consists of 4 cycles of a cisplatin-doublet (combination of a cisplatin and another chemotherapy drug, such as vinorelbine, docetaxel, paclitaxel). In patients who cannot receive cisplatin, carboplatin can be substituted. Combining neoadjuvant chemotherapy and immunotherapy is an area of active investigation; the treatment is well tolerated in certain populations and improves survival.
Adjuvant chemotherapy after surgery is now standard practice for patients with stage II or stage III disease and possibly also for patients with stage IB disease and tumors > 4 cm. Adjuvant chemotherapy increases 5-year survival rates. However, the decision to use adjuvant chemotherapy depends on the patient’s comorbidities and risk assessment. A commonly used chemotherapy regimen is a cisplatin-based doublet. 4 cm. Adjuvant chemotherapy increases 5-year survival rates. However, the decision to use adjuvant chemotherapy depends on the patient’s comorbidities and risk assessment. A commonly used chemotherapy regimen is a cisplatin-based doublet.
Stage III disease is treated with either chemotherapy, radiation therapy, surgery, or a combination of therapies; the sequence and choice of treatment depend on the location of the patient's disease and comorbidities. In general, concurrent chemotherapy, immunotherapy, and radiation therapy are considered standard treatment for unresectable clinically staged IIIA disease, but the survival remains poor (median survival, 10 to 14 months). Patients with stage IIIB disease with contralateral mediastinal nodal disease or supraclavicular nodal disease are offered either radiation therapy or chemotherapy or both. Patients with locally advanced tumors invading the heart, great vessels, mediastinum, or spine usually receive radiation therapy. In some patients (ie, those with T4 N0 M0 tumors), surgical resection with either neoadjuvant or adjuvant combined chemotherapy and radiation therapy may be feasible.
In stage IV disease, prolonging survival and palliation of symptoms are the goals. Chemotherapy, targeted drugs, and radiation therapy may be used to reduce tumor burden, relieve symptoms, and improve quality of life. However, if no mutation treatable with a targeted drug is identified, median survival is only 9 months, and < 25% of patients survive 1 year. Surgical palliative procedures may be required and may include thoracentesis and pleurodesis of recurrent effusions, placement of indwelling pleural drainage catheters, bronchoscopic fulguration of tumors involving the trachea and mainstem bronchi, placement of stents to prevent airway occlusion, and, in some cases, spinal stabilization for impending spinal cord compression.
Targeted therapy for NSCLC
NSCLC treatment is based on precision medicine. Molecular analysis is done on adenocarcinomas to look for specific mutations that can direct therapy (see table Some Targeted Therapy Drugs for Non–Small Cell Lung Cancer). Several immune oncology drugs (nivolumab, pembrolizumab, durvalumab, and atezolizumab) are available for NSCLC treatment. These drugs stimulate immune responsiveness, assist in the cancer being recognized as foreign, and inhibit the tumor's ability to block the natural immune system response. These drugs are used if the tumor advances despite chemotherapy (most often platinum-based doublets), and extensive work is being done to determine which tumors will respond to this treatment. For example, tumors that have high expression of the PD-L1 protein are responsive to pembrolizumab treatment.). Several immune oncology drugs (nivolumab, pembrolizumab, durvalumab, and atezolizumab) are available for NSCLC treatment. These drugs stimulate immune responsiveness, assist in the cancer being recognized as foreign, and inhibit the tumor's ability to block the natural immune system response. These drugs are used if the tumor advances despite chemotherapy (most often platinum-based doublets), and extensive work is being done to determine which tumors will respond to this treatment. For example, tumors that have high expression of the PD-L1 protein are responsive to pembrolizumab treatment.
For tumors bearing an oncogenic driver mutation, targeted treatments are used first. In patients with stage IV disease and sensitive EGFR mutations (ie, deletion exon 19, exon 21 L858 mutation), EGFR tyrosine kinase inhibitors (TKIs) may be given as first-line therapy; response rates and progression-free survival are better than those obtained using standard chemotherapy. EGFR TKIs include gefitinib, erlotinib, afatinib, and brigatinib. mutations (ie, deletion exon 19, exon 21 L858 mutation), EGFR tyrosine kinase inhibitors (TKIs) may be given as first-line therapy; response rates and progression-free survival are better than those obtained using standard chemotherapy. EGFR TKIs include gefitinib, erlotinib, afatinib, and brigatinib.
Osimertinib is the treatment of choice for EGFR-mutant NSCLC that has an acquired T790M mutation. In patients with nonsquamous NSCLC without an oncogenic driver mutation, bevacizumab, a vascular endothelial growth factor inhibitor, can be used in combination with standard chemotherapy (eg, a platinum-based doublet, such as carboplatin plus paclitaxel) to improve outcomes. Necitumumab can be used in combination with cisplatin plus gemcitabine for first-line treatment of NSCLC squamous cell carcinoma. Osimertinib is the treatment of choice for EGFR-mutant NSCLC that has an acquired T790M mutation. In patients with nonsquamous NSCLC without an oncogenic driver mutation, bevacizumab, a vascular endothelial growth factor inhibitor, can be used in combination with standard chemotherapy (eg, a platinum-based doublet, such as carboplatin plus paclitaxel) to improve outcomes. Necitumumab can be used in combination with cisplatin plus gemcitabine for first-line treatment of NSCLC squamous cell carcinoma.
Patients who have EML -4-ALK translocations should receive an ALK and ROS1 inhibitor (crizotinib, ceritinib, or alectinib). Patients with inhibitor (crizotinib, ceritinib, or alectinib). Patients withALK mutations can be given alectinib or ceritinib. mutations can be given alectinib or ceritinib.
Patients with BRAF mutations benefit from the BRAF inhibitors (eg, dabrafenib, trametinib). Many other targeted biologic agents are under investigation, including some that specifically target cancer cell signal transduction pathways or the angiogenesis pathways that supply oxygen and nutrition to growing tumor cells.inhibitors (eg, dabrafenib, trametinib). Many other targeted biologic agents are under investigation, including some that specifically target cancer cell signal transduction pathways or the angiogenesis pathways that supply oxygen and nutrition to growing tumor cells.
Some Targeted Therapy Drugs for Non–Small Cell Lung Cancer
Target | Drug | NSCLC |
|---|---|---|
ALK rearrangement | AlectinibAlectinib BrigatinibBrigatinib CeritinibCeritinib CrizotinibCrizotinib | Adenocarcinoma |
BRAF mutation | DabrafenibDabrafenib Trametinib Trametinib | Adenocarcinoma Squamous cell carcinoma |
EGFR mutation | AfatinibAfatinib ErlotinibErlotinib GefitinibGefitinib Necitumumab Necitumumab | Adenocarcinoma Squamous cell carcinoma |
EGFR (T790M mutation) | Osimertinib Osimertinib | Adenocarcinoma |
Inhibit blood vessel growth | BevacizumabBevacizumab Ramucirumab Ramucirumab | Adenocarcinoma |
Immune activation (checkpoint inhibitors) | AtezolizumabAtezolizumab CemiplimabCemiplimab DurvalumabDurvalumab IpilimumabIpilimumab NivolumabNivolumab PembrolizumabPembrolizumab | Adenocarcinoma Squamous cell carcinoma |
NSCLC = Non–small cell lung cancer. | ||
Recurrent lung cancer
Treatment options for lung cancer that recurs after definitive treatment vary by location and include repeat chemotherapy or targeted drugs for metastases, radiation therapy for local recurrence or pain caused by metastases, and brachytherapy for endobronchial disease when additional external radiation cannot be tolerated. Rarely, surgical resection of a solitary metastasis or for palliative purposes is considered.
The treatment of a locally recurrent NSCLC follows the same guidelines as for primary tumor stages I to III. If surgery was used initially, radiation therapy is the main modality. If the recurrence manifests as distant metastases, patients are treated as if they have stage IV disease with a focus on palliation.
Treatment for recurrent or metastatic stage IV NSCLC includes chemotherapy or targeted drugs. The choice depends on tumor histology, mutational profile, patient functional status, and patient preference. For example, an EGFR TKI, such as gefitinib or erlotinib, can be used as second- or third-line therapy even among patients who do not have sensitive TKI, such as gefitinib or erlotinib, can be used as second- or third-line therapy even among patients who do not have sensitiveEGFR mutations. When NSCLC progresses, repeat biopsies are commonly done to repeat the molecular and PD-L1 analysis, which can guide future treatment.
Complications of lung cancer
Asymptomatic malignant pleural effusions require no treatment. Initial treatment of a symptomatic effusion is with thoracentesis. Symptomatic effusions that recur despite multiple thoracenteses are drained through a chest tube. Infusion of talc (or occasionally, tetracycline or bleomycin) into the pleural space (a procedure called pleurodesis) scars the pleura, eliminates the pleural space, and is effective in . Symptomatic effusions that recur despite multiple thoracenteses are drained through a chest tube. Infusion of talc (or occasionally, tetracycline or bleomycin) into the pleural space (a procedure called pleurodesis) scars the pleura, eliminates the pleural space, and is effective in> 90% of cases. Pleurodesis can also be done surgically, often with a video-assisted thoracoscopic surgery (VATS) procedure.
Treatment of superior vena cava syndrome is the same as treatment of lung cancer, with chemotherapy (SCLC), radiation therapy (NSCLC), or both (NSCLC). Corticosteroids are commonly used but are of unproven benefit.
Treatment of Horner syndrome caused by apical tumors is with surgery with or without preoperative radiation therapy or with radiation therapy with or without adjuvant chemotherapy.
Treatment of paraneoplastic syndromes varies by syndrome.
End-of-life care
Based on poor overall survival, the need for end-of-life care should be anticipated. Studies have reported that early palliative care intervention leads to less end-of-life chemotherapy use and may even extend life (ie, by avoiding adverse effects of aggressive treatments).
Symptoms of breathlessness can be treated with supplemental oxygen and bronchodilators. Pre-terminal breathlessness can be treated with opioids.
Pain, anxiety, nausea, and anorexia are especially common and can be treated with parenteral morphine; oral, transdermal, or parenteral opioids; and antiemetics. Pain, anxiety, nausea, and anorexia are especially common and can be treated with parenteral morphine; oral, transdermal, or parenteral opioids; and antiemetics.
The care provided by hospice programs is extremely well-accepted by patients and families, yet this intervention is markedly underused.
Treatment references
1. Farjah F, Flum DR, Varghese TK Jr, et al: Surgeon specialty and long-term survival after pulmonary resection for lung cancer. Ann Thorac Surg 87 (4):995–1004, 2009. doi: 10.1016/j.athoracsur.2008.12.030
2. Schipper PH, Diggs BS, Ungerleider RM, Welke KF: The influence of surgeon specialty on outcomes in general thoracic surgery: A national sample 1996 to 2005. Ann Thorac Surg 88 (5):1566–1572, 2009. doi: 10.1016/j.athoracsur.2009.08.055
Prognosis for Lung Carcinoma
For SCLC, the overall prognosis is poor. The median survival time for limited-stage SCLC is 20 months, with a 5-year survival rate of 20%. Patients with extensive-stage SCLC do especially poorly, with a 5-year survival rate of < 1%.
For NSCLC, the 5-year survival rate varies by stage, from 68 to 92% for patients with stage I disease to 0 to 10 % for patients with stage IV disease (1). On average, untreated patients with metastatic NSCLC survive 6 months, whereas the median survival for treated patients is about 9 months. Patient survival has improved in both early and later stage NSCLC. Evidence shows improved survival in early-stage disease (stages IB to IIIB) when platinum-based chemotherapy regimens are used after surgical resection. In addition, targeted therapies have improved survival in patients with stage IV disease, in particular patients with an EGFR mutation, or EML-4-ALK or ROS1 translocations. Targeted therapies and improved sequential treatments are incrementally prolonging survival, particularly in later stage disease.
Prognosis reference
1. Goldstraw P, Chansky K, Crowley J, et al: The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 11(1):39-51, 2016. doi:10.1016/j.jtho.2015.09.009
Prevention of Lung Carcinoma
No active interventions to prevent lung cancer are proven to be effective except for smoking cessation.
Remediation of high radon levels in private residences removes known cancer-promoting radiation, but a reduction in lung cancer incidence is unproven.
Increasing dietary intake of fruits and vegetables high in retinoids and beta-carotene appears to have no effect on lung cancer incidence. Vitamin supplementation is either unproven (vitamin E) or harmful (beta-carotene) in people who smoke. Evidence suggesting that nonsteroidal anti-inflammatory drugs (NSAIDs) and vitamin E supplementation may protect people who formerly smoked from lung cancer has not been confirmed. Chemopreventive interventions, aside from smoking cessation, should be done only as part of a clinical trial. Increasing dietary intake of fruits and vegetables high in retinoids and beta-carotene appears to have no effect on lung cancer incidence. Vitamin supplementation is either unproven (vitamin E) or harmful (beta-carotene) in people who smoke. Evidence suggesting that nonsteroidal anti-inflammatory drugs (NSAIDs) and vitamin E supplementation may protect people who formerly smoked from lung cancer has not been confirmed. Chemopreventive interventions, aside from smoking cessation, should be done only as part of a clinical trial.
Molecular approaches targeting cell signaling and cell cycle pathways and tumor-associated antigens (precision chemoprevention) are under investigation.
Key Points
The main factor contributing to lung cancer is smoking.
About 15% of all lung cancer patients have never smoked cigarettes and have suspected driver mutations.
Lung cancer can be small cell lung carcinoma (SCLC) or non–small cell lung carcinoma (NSCLC).
Several genetic driver mutations that are amenable to targeted drugs have been identified in NSCLC; newly diagnosed adenocarcinoma should be tested for EGFR, ALK, BRAF, and ROS1 mutations. Tumors should also have PD-L1 immunostaining.
Manifestations can include cough, fever, hoarseness, pleural effusion, pneumonia, Pancoast tumor, paraneoplastic syndromes, superior vena cava syndrome, Horner syndrome, and metastases to the brain, liver, and bone.
Suspect the diagnosis based on clinical information and imaging studies (eg, CT, PET-CT), and confirm it histologically (eg, by cytology of sputum or pleural fluid or core biopsy).
Consider yearly screening with low-dose helical CT for people who currently smoke and those who formerly smoked who are ≥ 50 years and at high risk (> 20 pack-years of smoking, people who formerly smoked must have quit < 15 years ago); shared decision making should occur before imaging is pursued.
Do testing, beginning with whole-body imaging, to stage cancer.
Treat early-stage NSCLC with resection when pulmonary reserve is adequate, often followed by chemotherapy.
Treat advanced stage SCLC and NSCLC with chemotherapy and/or immunotherapy.
Genetic testing should be completed on adenocarcinoma to help define treatment regimens.
More Information
The following English language resources provide information for clinicians. THE MANUAL is not responsible for the content of this resource.
Lung Cancer Mutation Consortium: group of cancer centers that conduct clinical trials
US Preventive Services Task Force Recommendations for Lung Cancer Screening
Eastern Cooperative Oncology Group: A multidisciplinary organization that designs and conducts cancer research







