



Cor pulmonale is right ventricular (RV) enlargement secondary to a lung disorder that causes pulmonary artery hypertension. Right ventricular failure follows. Findings include peripheral edema, neck vein distention, hepatomegaly, and a parasternal lift. Diagnosis is clinical and by echocardiography. Treatment is directed at the cause.
Topic Resources
")


Cor pulmonale results from a disorder of the lung or its vasculature; it does not refer to right ventricular (RV) enlargement secondary to left ventricular (LV) failure, a congenital heart disorder (eg, ventricular septal defect), or an acquired valvular disorder. Cor pulmonale is usually chronic but may be acute and reversible. Primary pulmonary hypertension (ie, not caused by a pulmonary or cardiac disorder) is discussed elsewhere.
Pathophysiology of Cor Pulmonale
Lung disorders cause pulmonary hypertension that can lead to cor pulmonale by several mechanisms:
Loss of capillary beds (eg, due to bullous changes in COPD [chronic obstructive pulmonary disease] or thrombosis in pulmonary embolism)
Vasoconstriction caused by hypoxia, hypercapnia, or both
Increased alveolar pressure (eg, in COPD, during mechanical ventilation)
Medial hypertrophy in arterioles (often a response to pulmonary hypertension due to other mechanisms)
Pulmonary hypertension increases afterload on the RV, resulting in a cascade of events that is similar to what occurs in LV failure, including elevated end-diastolic and central venous pressure and ventricular hypertrophy and dilation. Demands on the RV may be intensified by increased blood viscosity due to hypoxia-induced polycythemia. Rarely, RV failure affects the LV if a dysfunctional septum bulges into the LV, interfering with filling and thus causing diastolic dysfunction.
Etiology of Cor Pulmonale
Acute cor pulmonale has few causes. Chronic cor pulmonale is usually caused by COPD, but there are several less common causes (see table Causes of Cor Pulmonale). In patients with COPD, an acute exacerbation or pulmonary infection may trigger RV overload. In chronic cor pulmonale, risk of venous thromboembolism is increased.
Causes of Cor Pulmonale
Acuity | Condition |
|---|---|
Acute | Massive pulmonary embolization Injury due to mechanical ventilation (most commonly in patients with ARDS) |
Chronic | COPD* Extensive loss of lung tissue due to surgery or trauma Chronic, unresolved pulmonary emboli Pulmonary veno-occlusive disorders Pulmonary interstitial fibrosis Kyphoscoliosis Obesity with alveolar hypoventilation Neuromuscular disorders involving respiratory muscles Idiopathic alveolar hypotension |
* COPD is the most common cause of chronic cor pulmonale. | |
ARDS = acute respiratory distress syndrome; COPD = chronic obstructive pulmonary disease. | |
Symptoms and Signs of Cor Pulmonale
Initially, cor pulmonale is asymptomatic, although patients usually have significant symptoms (eg, dyspnea, exertional fatigue) due to the underlying lung disorder. Later, as RV pressures increase, physical signs commonly include a left parasternal systolic lift, a loud pulmonic component of the 2nd heart sound (S2), and murmurs of functional tricuspid and pulmonic insufficiency (regurgitation). Later, an RV gallop rhythm (3rd [S3] and 4th [S4] heart sounds) augmented during inspiration, distended jugular veins (with a dominant a wave unless tricuspid regurgitation is present), hepatomegaly, and lower-extremity edema may occur.
Diagnosis of Cor Pulmonale
Clinical suspicion
Echocardiography
Cor pulmonale should be suspected in all patients with one of its causes. Chest x-ray shows RV and proximal pulmonary artery enlargement with distal arterial attenuation. ECG evidence of RV hypertrophy (eg, right axis deviation, QR wave in lead V1, and dominant R wave in leads V1 to V3) correlates well with degree of pulmonary hypertension. However, because pulmonary hyperinflation and bullae in COPD cause realignment of the heart, physical examination, x-rays, and ECG may be relatively insensitive.
Echocardiography or radionuclide imaging is done to evaluate LV and RV function; echocardiography can assess RV systolic pressure but is often technically limited by the lung disorder; cardiac MRI may be helpful in some patients to assess cardiac chambers and function. Right heart catheterization may be required for confirmation.

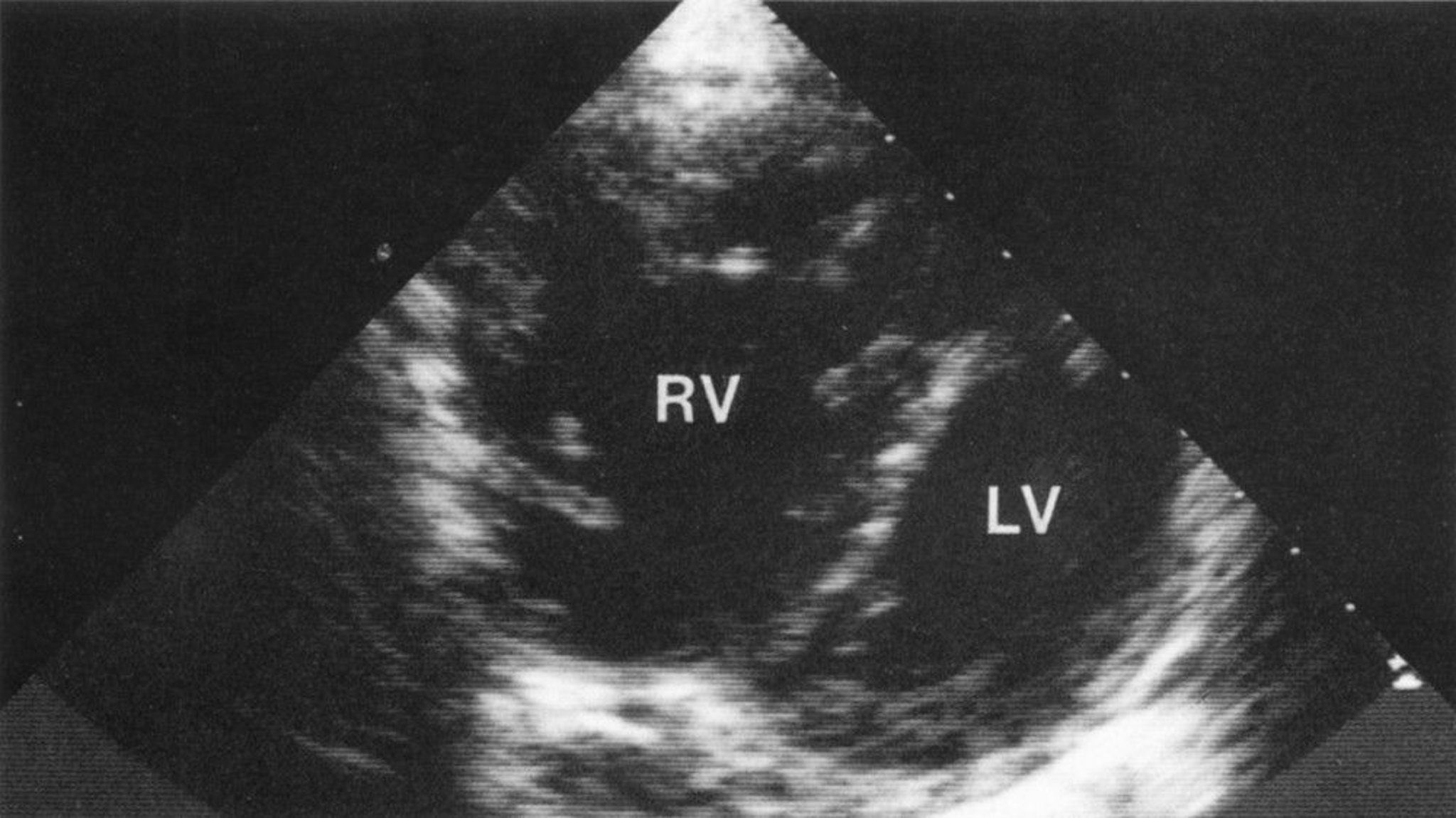
© Springer Science+Business Media
Treatment of Cor Pulmonale
Treatment of cause
Treatment of cor pulmonale is difficult; it focuses on the cause (see table Causes of Heart Failure), particularly alleviation or moderation of hypoxia. Early identification and treatment are important before structural changes become irreversible.
If peripheral edema is present, diuretics may seem appropriate, but they are helpful only if LV failure and pulmonary fluid overload are also present. Diuretics should be used cautiously because small decreases in preload often worsen cor pulmonale. Pulmonary vasodilators (eg, hydralazine, calcium channel blockers, nitrous oxide, prostacyclin, phosphodiesterase inhibitors), although beneficial in primary pulmonary hypertension, are not effective. Bosentan, an endothelin receptor blocker, also may benefit patients with primary pulmonary hypertension, but its use is not well studied in cor pulmonale. Digoxin is effective only if patients have concomitant LV dysfunction; caution is required because patients with COPD are sensitive to digoxin’s effects. If peripheral edema is present, diuretics may seem appropriate, but they are helpful only if LV failure and pulmonary fluid overload are also present. Diuretics should be used cautiously because small decreases in preload often worsen cor pulmonale. Pulmonary vasodilators (eg, hydralazine, calcium channel blockers, nitrous oxide, prostacyclin, phosphodiesterase inhibitors), although beneficial in primary pulmonary hypertension, are not effective. Bosentan, an endothelin receptor blocker, also may benefit patients with primary pulmonary hypertension, but its use is not well studied in cor pulmonale. Digoxin is effective only if patients have concomitant LV dysfunction; caution is required because patients with COPD are sensitive to digoxin’s effects.
Phlebotomy during hypoxic cor pulmonale has been suggested, but the benefits of decreasing blood viscosity are not likely to offset the harm of reducing oxygen-carrying capacity unless significant polycythemia is present. For patients with chronic cor pulmonale, long-term anticoagulants reduce risk of venous thromboembolism.
Key Points
Cor pulmonale is RV enlargement and eventually failure secondary to a lung disorder that causes pulmonary artery hypertension.
Cor pulmonale itself is usually asymptomatic but common physical findings include a left parasternal systolic lift, a loud pulmonic component of S2, functional tricuspid and pulmonic regurgitation murmurs, and later, distended jugular veins, hepatomegaly, and lower-extremity edema.
Diagnosis usually requires echocardiography or radionuclide imaging, and sometimes right heart catheterization.
Early identification and treatment of the cause are important before cardiac structural changes become irreversible.
Although patients may have significant peripheral edema, diuretics are not helpful and may be harmful; small decreases in preload often worsen cor pulmonale.







