


Heart failure (HF) is a syndrome of ventricular dysfunction. Left ventricular (LV) failure causes shortness of breath and fatigue, and right ventricular (RV) failure causes peripheral and abdominal fluid accumulation; the ventricles can be involved together or separately. Diagnosis is initially clinical, supported by chest x-ray, echocardiography, and levels of plasma natriuretic peptides. Treatment includes patient education, diuretics, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers, beta-blockers, aldosterone antagonists, sodium-glucose cotransporter-2 inhibitors, neprilysin inhibitors, sinus node inhibitors, specialized implantable pacemakers/defibrillators and other devices, and correction of the cause(s) of the HF syndrome.Heart failure (HF) is a syndrome of ventricular dysfunction. Left ventricular (LV) failure causes shortness of breath and fatigue, and right ventricular (RV) failure causes peripheral and abdominal fluid accumulation; the ventricles can be involved together or separately. Diagnosis is initially clinical, supported by chest x-ray, echocardiography, and levels of plasma natriuretic peptides. Treatment includes patient education, diuretics, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers, beta-blockers, aldosterone antagonists, sodium-glucose cotransporter-2 inhibitors, neprilysin inhibitors, sinus node inhibitors, specialized implantable pacemakers/defibrillators and other devices, and correction of the cause(s) of the HF syndrome.
Heart failure affects about 6.5 million people in the US; > 960,000 new cases occur each year. About 26 million people are affected worldwide.
(See also Heart Failure in Children.)
Physiology of Heart Failure
Cardiac contractility (force and velocity of contraction), ventricular performance, and myocardial oxygen requirements are determined by
Preload
Afterload
Substrate availability (eg, oxygen, fatty acids, glucose)
Heart rate and rhythm
Amount of viable myocardium
Cardiac output (CO) is the product of stroke volume and heart rate; it is also affected by venous return, peripheral vascular tone, and neurohumoral factors.
Preload is the loading condition of the heart at the end of its relaxation and filling phase (diastole) just before contraction (systole). Preload represents the degree of end-diastolic fiber stretch and end-diastolic volume, which is influenced by ventricular diastolic pressure and the composition of the myocardial wall. Typically, left ventricular (LV) end-diastolic pressure, especially if higher than normal, is a reasonable measure of preload. LV dilation, hypertrophy, and changes in myocardial distensibility (compliance) modify preload.
Afterload is the force resisting myocardial fiber contraction at the start of systole. It is determined by LV chamber pressure, radius, and wall thickness at the time the aortic valve opens. Clinically, systemic systolic blood pressure at or shortly after the aortic valve opens correlates with peak systolic wall stress and approximates afterload.
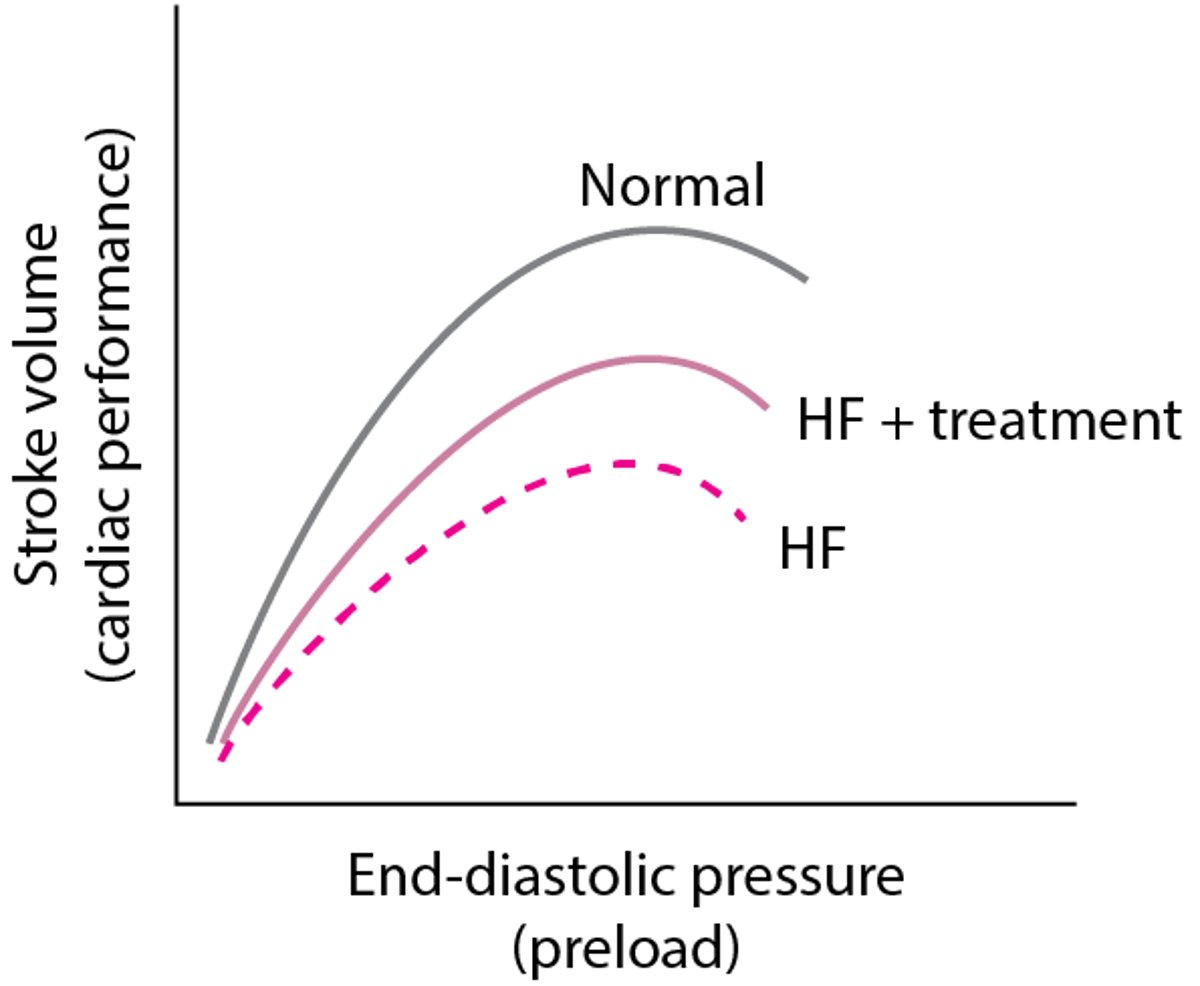
The Frank-Starling principle describes the relationship between preload and cardiac performance. It states that, normally, systolic contractile performance (represented by stroke volume or CO) is proportional to preload within the normal physiologic range (see figure Frank-Starling principle). Contractility is difficult to measure clinically (because it requires cardiac catheterization with pressure-volume analysis) but is reasonably reflected by the ejection fraction (EF), which is the percentage of end-diastolic volume ejected with each contraction (stroke volume/end-diastolic volume). EF can generally be adequately assessed noninvasively with echocardiography, nuclear imaging, or MRI.
The force-frequency relationship refers to the phenomenon in which repetitive stimulation of a muscle within a certain frequency range results in increased force of contraction. Normal cardiac muscle at typical heart rates exhibits a positive force-frequency relationship, so a faster rate causes stronger contraction (and corresponding greater substrate requirements). During some types of heart failure, the force-frequency relationship may become negative, so that myocardial contractility decreases as heart rate increases above a certain rate.
Cardiac reserve is the ability of the heart to increase its performance above resting levels in response to emotional or physical stress; body oxygen consumption may increase from 250 to ≥ 1500 mL/minute during maximal exertion. Mechanisms include
Increasing heart rate
Increasing systolic and diastolic volumes
Increasing stroke volume
Increasing tissue extraction of oxygen (the difference between oxygen content in arterial blood and in mixed venous or pulmonary artery blood)
In well-trained young adults during maximal exercise, heart rate may increase from 55 to 70 beats/minute at rest to 180 beats/minute, and CO may increase from 6 to ≥ 25 L/minute. At rest, arterial blood contains about 18 mL oxygen/dL of blood, and mixed venous or pulmonary artery blood contains about 14 mL/dL. Oxygen extraction is thus about 4 mL/dL. When demand is increased, oxygen extraction may increase to 12 to 14 mL/dL. This mechanism also helps compensate for reduced tissue blood flow in heart failure.
Frank-Starling principle
Normally (top curve), as preload increases, cardiac performance also increases. However at a certain point, performance plateaus, then declines. In heart failure (HF) due to systolic dysfunction (bottom curve), the overall curve shifts downward, reflecting reduced cardiac performance at a given preload, and as preload increases, cardiac performance increases less. With treatment (middle curve), performance is improved, although not normalized. |

Pathophysiology of Heart Failure
In heart failure, the heart may not provide tissues with adequate blood for metabolic needs, and cardiac-related elevation of pulmonary or systemic venous pressures may result in organ congestion. This condition can result from abnormalities of systolic or diastolic function or, commonly, both. Although a primary abnormality can be a change in cardiomyocyte function, there are also changes in collagen turnover of the extracellular matrix. Cardiac structural defects (eg, congenital defects, valvular disorders), rhythm abnormalities (including persistently high heart rate), and high metabolic demands (eg, due to thyrotoxicosis) also can cause HF.
Heart failure with reduced ejection fraction (HFrEF)
In HFrEF (also called systolic HF), global LV systolic dysfunction predominates. The LV contracts poorly and empties inadequately, leading to
Increased diastolic volume and pressure
Decreased ejection fraction (≤ 40%)
Many defects in energy utilization, energy supply, electrophysiologic functions, and contractile element interaction occur, with abnormalities in intracellular calcium modulation and cAMP production.
Predominant systolic dysfunction is common in heat failure due to myocardial infarction, myocarditis, and dilated cardiomyopathy. Systolic dysfunction may affect primarily the LV or the right ventricle (RV); LV failure often leads to RV failure.
Heart failure with preserved ejection fraction (HFpEF)
In HFpEF (also called diastolic heart failure), LV filling is impaired, resulting in
Increased LV end-diastolic pressure at rest or during exertion
Usually, normal LV end-diastolic volume
Global contractility and hence ejection fraction remain normal (≥ 50%).
However, in some patients, marked restriction to LV filling can cause inappropriately low LV end-diastolic volume and thus cause low CO (cardiac output) and systemic symptoms. Elevated left atrial pressures can cause pulmonary hypertension and pulmonary congestion.
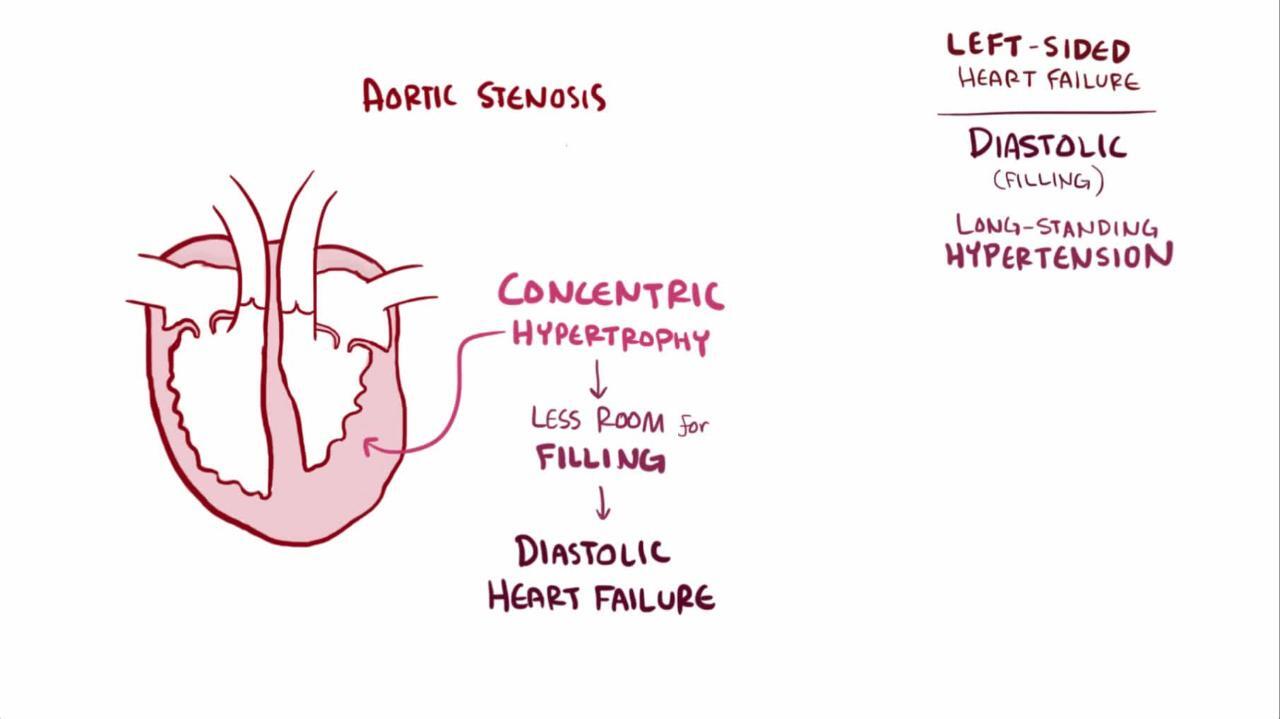
Diastolic dysfunction usually results from impaired ventricular relaxation (an active process), increased ventricular stiffness, valvular disease, or constrictive pericarditis. Acute myocardial ischemia is also a cause of diastolic dysfunction. Resistance to filling increases with age, reflecting both cardiomyocyte dysfunction and cardiomyocyte loss, and increased interstitial collagen deposition; thus, diastolic dysfunction is particularly common among older adults. Diastolic dysfunction predominates in hypertrophic cardiomyopathy, other disorders with ventricular hypertrophy (eg, hypertension, significant aortic stenosis), and amyloid infiltration of the myocardium. LV filling and function may also be impaired if marked increases in RV pressure shift the interventricular septum to the left.
Diastolic dysfunction has increasingly been recognized as a cause of HF. Estimates vary, but about 50% of patients with heart failure have HFpEF; the prevalence increases with age and in patients with diabetes. It is now known that HFpEF is a complex, heterogenous, multiorgan, systemic syndrome, often with multiple concomitant pathophysiologies. Current data suggest that multiple comorbidities (eg, obesity, hypertension, diabetes, chronic kidney disease) lead to systemic inflammation, widespread endothelial dysfunction, cardiac microvascular dysfunction, and, ultimately, molecular changes in the heart that cause increased myocardial fibrosis and ventricular stiffening. Thus, although HFrEF is typically associated with primary myocardial injury, HFpEF may be associated with secondary myocardial injury due to abnormalities in the periphery.
Heart failure with mildly reduced ejection fraction (HFmrEF)
International societies have put forth the concept of HF with mildly reduced ejection fraction (HFmrEF), in which patients have an LV ejection fraction of 41 to 49%. It is unclear whether this group is a distinct population or consists of a mixture of patients with either HFpEF or HFrEF.
LV failure
In heart failure that involves left ventricular dysfunction, CO decreases and pulmonary venous pressure increases. When pulmonary capillary pressure exceeds the oncotic pressure of plasma proteins (about 24 mm Hg), fluid extravasates from the capillaries into the interstitial space and alveoli, reducing pulmonary compliance and increasing the work of breathing. Lymphatic drainage increases but cannot compensate for the increase in pulmonary fluid. Marked fluid accumulation in alveoli (pulmonary edema) significantly alters ventilation-perfusion (V/Q) relationships: Deoxygenated pulmonary arterial blood passes through poorly ventilated alveoli, decreasing systemic arterial oxygenation (PaO2) and causing dyspnea. However, dyspnea may occur before V/Q abnormalities, probably because of elevated pulmonary venous pressure and increased work of breathing; the precise mechanism is unclear.
In severe or chronic LV failure, pleural effusions characteristically develop, further aggravating dyspnea. Minute ventilation increases; thus, PaCO2 decreases and blood pH increases (respiratory alkalosis). Marked interstitial edema of the small airways may interfere with ventilation, elevating PaCO2—a sign of impending respiratory failure.
RV failure
In heart failure that involves right ventricular dysfunction, systemic venous pressure increases, causing fluid extravasation and consequent edema, primarily in dependent tissues (feet and ankles of ambulatory patients) and abdominal viscera. The liver is most severely affected, but the stomach and intestine also become congested; fluid accumulation in the peritoneal cavity (ascites) can occur. RV failure commonly causes moderate hepatic dysfunction, with usually modest increases in conjugated and unconjugated bilirubin, PT (prothrombin time), and hepatic enzymes (particularly alkaline phosphatase and gamma-glutamyl transpeptidase [GGT]). The impaired liver breaks down less aldosterone, further contributing to fluid accumulation. Chronic venous congestion in the viscera can cause anorexia, malabsorption of nutrients and drugs, protein-losing enteropathy (characterized by diarrhea and marked hypoalbuminemia), chronic gastrointestinal blood loss, and rarely ischemic bowel infarction.
Cardiac response
In HFrEF, left ventricular systolic function is grossly impaired; therefore, a higher preload is required to maintain CO. As a result, the ventricles are remodeled over time: During remodelling, the LV becomes less ovoid and more spherical, dilates, and hypertrophies; the RV dilates and may hypertrophy. Initially compensatory, remodelling ultimately is associated with adverse outcomes because the changes eventually increase diastolic stiffness and wall tension (ie, diastolic dysfunction develops), compromising cardiac performance, especially during physical stress. Increased wall stress raises oxygen demand and accelerates apoptosis (programmed cell death) of myocardial cells. Dilation of the ventricles can also cause mitral or tricuspid valve regurgitation (due to annular dilation) with further increases in end-diastolic volumes.
Hemodynamic responses
With reduced CO, oxygen delivery to the tissues is maintained by increasing oxygen extraction from the blood and sometimes shifting the oxyhemoglobin dissociation curve (see figure Oxyhemoglobin dissociation curve) to the right to favor oxygen release.
Reduced CO with lower systemic blood pressure activates arterial baroreflexes, increasing sympathetic tone and decreasing parasympathetic tone. As a result, heart rate and myocardial contractility increase, arterioles in selected vascular beds constrict, venoconstriction occurs, and sodium and water are retained. These changes compensate for reduced ventricular performance and help maintain hemodynamic homeostasis in the early stages of heart failure. However, these compensatory changes increase cardiac work, preload, and afterload; reduce coronary and renal perfusion; cause fluid accumulation resulting in congestion; increase potassium excretion; and may cause cardiomyocyte necrosis and arrhythmias.
Renal responses
As cardiac function deteriorates, renal blood flow decreases (due to low cardiac output). In addition, renal venous pressures increase, leading to renal venous congestion. These changes both result in a decrease in GFR (glomerular filtration rate), and blood flow within the kidneys is redistributed. The filtration fraction and filtered sodium decrease, but tubular resorption increases, leading to sodium and water retention. Blood flow is further redistributed away from the kidneys during exercise, but renal blood flow improves during rest.
Decreased perfusion of the kidneys (and possibly decreased arterial systolic stretch secondary to declining ventricular function) activates the renin-angiotensin-aldosterone system (RAAS), increasing sodium and water retention and renal and peripheral vascular tone. These effects are amplified by the intense sympathetic activation accompanying heart failure.
The renin-angiotensin-aldosterone-vasopressin (antidiuretic hormone [ADH]) system causes a cascade of potentially deleterious long-term effects. Angiotensin II worsens heart failure by causing vasoconstriction, including efferent renal vasoconstriction, and by increasing aldosterone production, which enhances sodium reabsorption in the distal nephron and also causes myocardial and vascular collagen deposition and fibrosis. Angiotensin II increases (antidiuretic hormone [ADH]) system causes a cascade of potentially deleterious long-term effects. Angiotensin II worsens heart failure by causing vasoconstriction, including efferent renal vasoconstriction, and by increasing aldosterone production, which enhances sodium reabsorption in the distal nephron and also causes myocardial and vascular collagen deposition and fibrosis. Angiotensin II increasesnorepinephrine release, stimulates release of vasopressin, and triggers apoptosis. Angiotensin II may be involved in vascular and myocardial hypertrophy, thus contributing to the remodeling of the heart and peripheral vasculature, potentially worsening HF. Aldosterone can be synthesized in the heart and vasculature independently of angiotensin II (perhaps mediated by , and triggers apoptosis. Angiotensin II may be involved in vascular and myocardial hypertrophy, thus contributing to the remodeling of the heart and peripheral vasculature, potentially worsening HF. Aldosterone can be synthesized in the heart and vasculature independently of angiotensin II (perhaps mediated bycorticotropin, nitric oxide, free radicals, and other stimuli) and may have deleterious effects in these organs.
Heart failure that causes progressive renal dysfunction (including renal dysfunction caused by drugs used to treat HF) contributes to worsening HF and has been termed the cardiorenal syndrome.
Neurohumoral responses
In conditions of stress, neurohumoral responses help increase heart function and maintain blood pressure and organ perfusion, but chronic activation of these responses is detrimental to the normal balance between myocardial-stimulating and vasoconstricting hormones and between myocardial-relaxing and vasodilating hormones.
The heart contains many neurohumoral receptors (alpha-1, beta-1, beta-2, beta-3, angiotensin II type 1 [AT1] and type 2 [AT2], muscarinic, endothelin, serotonin, The heart contains many neurohumoral receptors (alpha-1, beta-1, beta-2, beta-3, angiotensin II type 1 [AT1] and type 2 [AT2], muscarinic, endothelin, serotonin,adenosine, cytokine, natriuretic peptides); the roles of all of these receptors are not yet fully defined. In patients with heart failure, beta-1 receptors (which constitute 70% of cardiac beta receptors) are downregulated, probably in response to intense sympathetic activation. The result of downregulation is impaired myocyte contractility and increased heart rate.
Plasma norepinephrine levels are increased, largely reflecting sympathetic nerve stimulation as plasma epinephrine levels are not increased. Detrimental effects include vasoconstriction with increased preload and afterload, direct myocardial damage including apoptosis, reduced renal blood flow, and activation of other neurohumoral systems, including the renin-angiotensin-aldosterone-vasopressin system.
Vasopressin is released in response to a fall in blood pressure via various neurohormonal stimuli. Increased vasopressin decreases renal excretion of free water, possibly contributing to hyponatremia in heart failure. Vasopressin levels in patients with HF and normal blood pressure vary.
Atrial natriuretic peptide is released in response to increased atrial volume and pressure; brain (B-type) natriuretic peptide (BNP) is released from the ventricle in response to ventricular stretching. These peptides enhance renal excretion of sodium, but in patients with HF, the effect is blunted by decreased renal perfusion pressure, receptor downregulation, and perhaps enhanced enzymatic degradation. In addition, elevated levels of natriuretic peptides exert a counter-regulatory effect on the renin-angiotensin-aldosterone system and catecholamine stimulation.
Because endothelial dysfunction occurs in HF, fewer endogenous vasodilators (eg, nitric oxide, prostaglandins) are produced, and more endogenous vasoconstrictors (eg, endothelin) are produced, thus increasing afterload.
The failing heart and other organs produce tumor necrosis factor (TNF) alpha. This cytokine increases catabolism and is possibly responsible for cardiac cachexia (loss of lean tissue ≥ 10%), which may accompany severely symptomatic HF, and for other detrimental changes. The failing heart also undergoes metabolic changes with increased free fatty acid utilization and decreased glucose utilization; these changes may become therapeutic targets.
Changes with aging
Age-related changes in the heart and cardiovascular system lower the threshold for expression of heart failure. Interstitial collagen within the myocardium increases, the myocardium stiffens, and myocardial relaxation is prolonged. These changes lead to a significant reduction in diastolic left ventricular function, even in healthy older people. Modest decline in systolic function also occurs with aging. An age-related decrease in myocardial and vascular responsiveness to beta-adrenergic stimulation further impairs the ability of the cardiovascular system to respond to increased work demands.
As a result of these changes, peak exercise capacity decreases significantly (about 8%/decade after age 30), and CO at peak exercise decreases more modestly. This decline can be slowed by regular physical exercise. Thus, older patients are more prone than are younger ones to develop HF symptoms in response to the stress of systemic disorders or relatively modest cardiovascular insults. Stressors include infections (particularly pneumonia), hyperthyroidism, anemia, hypertension, myocardial ischemia, hypoxia, hyperthermia, renal failure, perioperative IV fluid loads, nonadherence to drug regimens or to low-salt diets, and use of certain drugs (particularly NSAIDs [nonsteroidal anti-inflammatory drugs]).
Etiology of Heart Failure
Both cardiac and systemic factors can impair cardiac performance and cause or aggravate heart failure.
Causes of Heart Failure
Type | Examples |
|---|---|
Cardiac | |
Myocardial damage | Some chemotherapy drugs |
Valvular disorders | |
Arrhythmias | Bradyarrhythmias Tachyarrhythmias |
Conduction defects | |
Reduced substrate availability (eg, of free fatty acids or glucose) | Ischemia |
Infiltrative or matrix disorders | Chronic fibrosis (eg, systemic sclerosis) |
Systemic | |
Disorders that increase demand for CO | |
Disorders that increase resistance to output (afterload) | |
AV = atrioventricular; CO = cardiac output. | |
Classification of Heart Failure
The most common classification of heart failure currently in use stratifies patients into
Heart failure with reduced ejection fraction ("systolic HF")
Heart failure with preserved ejection fraction ("diastolic HF")
Heart failure with reduced ejection fraction (HFrEF) is defined as heart failure with left ventricular ejection fraction (LVEF) ≤ 40%.
Heart failure with preserved ejection fraction (HFpEF) is defined as heart failure with LVEF ≥ 50%.
Patients with LVEF between 41% and 49% are in an intermediate zone, and have recently been categorized as HF with mildly reduced ejection fraction (HFmrEF—1).
The traditional distinction between left and right ventricular failure is somewhat misleading because the heart is an integrated pump, and changes in one chamber ultimately affect the whole heart. However, these terms indicate the major site of pathology leading to heart failure and can be useful for initial evaluation and treatment. Other common descriptive terms for heart failure include acute or chronic; high output or low output; dilated or nondilated; and ischemic, hypertensive, or idiopathic dilated cardiomyopathy. Treatment differs based on whether the presentation is acute or chronic HF.
LV failure characteristically develops in ischemic heart disease, hypertension, mitral regurgitation, aortic regurgitation, aortic stenosis, most forms of cardiomyopathy, and congenital heart disorders (eg, ventricular septal defect, patent ductus arteriosus with large shunts).
RV failure is most commonly caused by previous LV failure (which increases pulmonary venous pressure and leads to pulmonary hypertension, thus overloading the RV) or by a severe lung disorder (in which case it is called cor pulmonale). Other causes are multiple pulmonary emboli, RV infarction, pulmonary arterial hypertension, tricuspid regurgitation, tricuspid stenosis, mitral stenosis, pulmonary artery stenosis, pulmonic valve stenosis, pulmonary venous occlusive disease, arrhythmogenic RV cardiomyopathy, or congenital disorders such as Ebstein anomaly or Eisenmenger syndrome. Some conditions mimic RV failure, except cardiac function may be normal; they include volume overload and increased systemic venous pressure in polycythemia or overtransfusion, acute kidney injury with retention of sodium and water, obstruction of either vena cava, and hypoproteinemia due to any cause resulting in low plasma oncotic pressure and peripheral edema.
Biventricular failure results from disorders that affect the whole myocardium (eg, viral myocarditis, amyloidosis, Chagas disease) or long-standing LV failure causing RV failure.
High-output HF results from a persistently high cardiac output, which may eventually result in an inability of a normal heart to maintain adequate output. Conditions that may increase CO (cardiac output) include severe anemia, end-stage liver disease, beriberi, thyrotoxicosis, advanced Paget disease, arteriovenous fistula, and persistent tachycardia.
Cardiomyopathy is a general term indicating disease of the myocardium. Most commonly, the term refers to a primary disorder of the ventricular myocardium that is not caused by congenital anatomic defects; valvular, systemic, or pulmonary vascular disorders; isolated pericardial, nodal, or conduction system disorders; or epicardial coronary artery disease (CAD). The term is sometimes used to reflect etiology (eg, ischemic vs hypertensive cardiomyopathy). Cardiomyopathy does not always lead to symptomatic HF. It is often idiopathic and is classified as dilated, congestive, hypertrophic, infiltrative-restrictive, or apical-ballooning cardiomyopathy (also known as takotsubo or stress cardiomyopathy).
Classification reference
1. Heidenreich PA, Bozkurt B, Aguilar D, et al: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145:e876–e894, 2022, doi: 10.1161/CIR.0000000000001062
Symptoms and Signs of Heart Failure
Manifestations of heart failure differ depending on the extent to which the LV and RV are initially affected. Clinical severity varies significantly and is usually classified according to the New York Heart Association (NYHA) system (see table NYHA Classification of Heart Failure); the examples of ordinary activity may be modified for older, debilitated patients. Because HF has such a broad range of severity, some experts suggest subdividing NYHA class III into IIIA or IIIB. Class IIIB is typically reserved for those patients who recently had a heart failure exacerbation. The American College of Cardiology/American Heart Association has advocated a staging system for HF (A, B, C, or D) to highlight the need for HF prevention.
A: High risk of HF but no structural or functional cardiac abnormalities or symptoms
B: Structural or functional cardiac abnormalities but no symptoms of HF
C: Structural heart disease with symptoms of HF
D: Refractory HF requiring advanced therapies (eg, mechanical circulatory support, cardiac transplantation) or palliative care
Severe LV failure may cause pulmonary edema or cardiogenic shock.
New York Heart Association (NYHA) Classification of Heart Failure
NYHA Class | Definition | Limitation | Example |
|---|---|---|---|
I | Ordinary physical activity does not cause undue fatigue, dyspnea, or palpitations. | None | Can complete any activity requiring ≤ 7 MET:
|
II | Ordinary physical activity causes fatigue, dyspnea, palpitations, or angina. | Mild | Can complete any activity requiring ≤ 5 MET:
|
III | Comfortable at rest; less than ordinary physical activity causes fatigue, dyspnea, palpitations, or angina. | Moderate | Can complete any activity requiring ≤ 2 MET:
|
IV | Symptoms occur at rest; any physical activity increases discomfort. | Severe | Cannot do or cannot complete any activity requiring ≥ 2 MET; cannot do any of the above activities |
MET = metabolic equivalent of task, a measure of how much energy is expended compared to remaining at rest. | |||
History
In LV failure, the most common symptoms are dyspnea and fatigue due to increased pulmonary venous pressures, and low cardiac output (CO, at rest or inability to augment CO during exertion). Dyspnea usually occurs during exertion and is relieved by rest. As HF worsens, dyspnea can occur during rest and at night, sometimes causing nocturnal cough. Dyspnea occurring immediately or soon after lying flat and relieved promptly by sitting up (orthopnea) is common as heart failure advances. In paroxysmal nocturnal dyspnea (PND), dyspnea awakens patients several hours after they lie down and is relieved only after they sit up for 15 to 20 minutes. In severe HF, periodic cycling of breathing (Cheyne-Stokes respiration—from a brief period of apnea, patients breathe progressively faster and deeper, then slower and shallower until they become apneic and repeat the cycle)—can occur during the day or night; the sudden hyperpneic phase may awaken the patient from sleep. Cheyne-Stokes breathing differs from PND in that the hyperpneic phase is short, lasting only 10 to 15 seconds, but the cycle recurs regularly, lasting 30 seconds to 2 minutes. PND is associated with pulmonary congestion, and Cheyne-Stokes respiration with low CO. Sleep-related breathing disorders, such as sleep apnea, are common in HF and may aggravate HF. Severely reduced cerebral blood flow and hypoxemia can cause chronic irritability and impair mental performance.
In RV failure, the most common symptoms are ankle swelling and fatigue. Sometimes patients feel a sensation of fullness in the abdomen or neck. Hepatic congestion can cause right upper quadrant abdominal discomfort, and stomach and intestinal congestion can cause early satiety, anorexia, and abdominal bloating.
Less specific heart failure symptoms include cool peripheries, postural light-headedness, nocturia, and decreased daytime micturition. Skeletal muscle wasting can occur in severe biventricular failure and may reflect some disuse but also increased catabolism associated with increased cytokine production. Significant weight loss (cardiac cachexia) is an ominous sign associated with high mortality.
In older people, presenting complaints may be atypical, such as confusion, delirium, falls, sudden functional decline, nocturnal urinary incontinence, or sleep disturbance. Coexisting cognitive impairment and depression may also influence assessment and therapeutic interventions and may be worsened by the HF.
Examination
General examination may detect signs of systemic or cardiac disorders that cause or aggravate heart failure (eg, anemia, hyperthyroidism, alcohol use disorder, hemochromatosis, atrial fibrillation with rapid rate, mitral regurgitation).
In LV failure, tachycardia and tachypnea may occur. Patients with severe LV failure may appear visibly dyspneic or cyanotic, hypotensive, and confused or agitated because of hypoxia and poor cerebral perfusion. Some of these less specific symptoms (eg, confusion) are more common in older patients.
Central cyanosis (affecting all of the body, including warm areas such as the tongue and mucous membranes) reflects severe hypoxemia. Peripheral cyanosis of the lips, fingers, and toes reflects low blood flow with increased oxygen extraction. If vigorous massage improves nail bed color, cyanosis may be peripheral; increasing local blood flow does not improve color if cyanosis is central.
Cardiac findings in HFrEF include
Diffuse, sustained, and laterally displaced apical impulse
Audible and occasionally palpable 3rd (S3) and 4th (S4) heart sounds
Accentuated pulmonic component (P2) of the 2nd heart sound (S2)
These abnormal heart sounds also can occur in HFpEF. A pansystolic murmur of mitral regurgitation at the apex may occur in either HFrEF or HFpEF.
Pulmonary findings include early inspiratory basilar crackles that do not clear with coughing and, if pleural effusion is present, dullness to percussion and diminished breath sounds at the lung base(s).
Signs of RV failure include
Nontender peripheral pitting edema (digital pressure leaves visible and palpable imprints, sometimes quite deep) in the feet and ankles
Enlarged and sometimes pulsatile liver palpable below the right costal margin
Abdominal swelling and ascites
Visible elevation of the jugular venous pressure, sometimes with large a or v waves that are visible even when the patient is seated or standing (see figure Normal jugular vein waves)
In severe cases of heart failure, peripheral edema can extend to the thighs or even the sacrum, scrotum, lower abdominal wall, and occasionally even higher. Severe edema in multiple areas is termed anasarca. Edema may be asymmetric if patients lie predominantly on one side.
Large V waves in the jugular veins are usually indicative of significant tricuspid regurgitation which is often present in RV failure. A paradoxical increase in the jugular venous pressure during inspiration (Kussmaul sign) is indicative of right-sided heart failure and can occur in RV failure, restrictive cardiomyopathy, constrictive pericarditis, and severe tricuspid regurgitation.
With hepatic congestion, the liver may be palpably enlarged or tender, and hepatojugular or abdominal-jugular reflux may be detected (see Approach to the Cardiac Patient). Precordial palpation may detect the left parasternal lift of RV enlargement, and auscultation may detect the murmur of tricuspid regurgitation or the RV S3 along the left sternal border; both findings are augmented upon inspiration.
Diagnosis of Heart Failure
Sometimes only clinical evaluation
Chest x-ray
Echocardiography, cardiac radionuclide scan, and/or MRI
BNP or N-terminal-pro-BNP (NT-pro-BNP) levels
ECG and other tests for etiology as needed
Clinical findings (eg, exertional dyspnea or fatigue, orthopnea, edema, tachycardia, pulmonary crackles, S3, jugular venous distention) suggest heart failure but are usually not apparent early. Some similar symptoms may result from COPD (chronic obstructive pulmonary disease) or recurrent pneumonia or may be erroneously attributed to obesity or old age. Suspicion for heart failure should be high in patients with a history of myocardial infarction, hypertension, or valvular disorders or murmurs and should be moderate in any patient who is older or has diabetes.
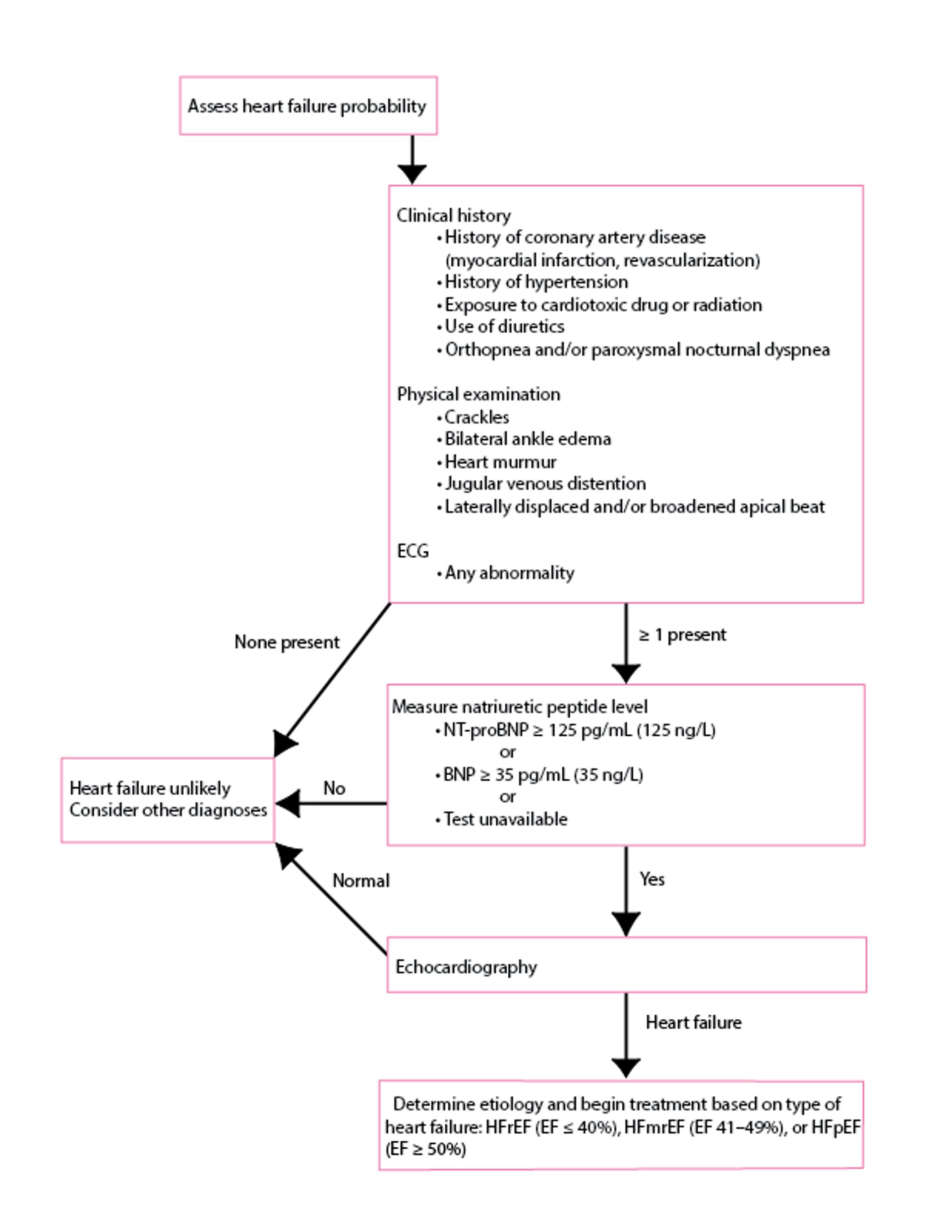
Chest x-ray, ECG, and an objective test of cardiac function, typically echocardiography, should be done (see figure Diagnosis of heart failure of acute onset). Blood tests, except for BNP levels, are not used for diagnosis but are useful for identifying cause and systemic effects (1, 2).
Diagnosis of heart failure of acute onset
Data from McDonagh TA, Metra M, Adamo M, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599-3726, 2021. doi: 10.1093/eurheartj/ehab368. |

Chest x-ray
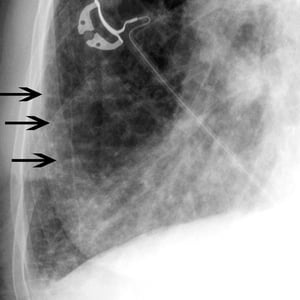
Chest x-ray findings suggesting heart failure include an enlarged cardiac silhouette, pleural effusion, fluid in the major fissure, and horizontal lines in the periphery of lower posterior lung fields (Kerley B lines). These findings reflect chronic elevation of left atrial pressure and chronic thickening of the intralobular septa due to edema. Upper lobe pulmonary venous congestion and interstitial or alveolar edema may also be present. Careful examination of the cardiac silhouette on a lateral projection can identify specific ventricular and atrial chamber enlargement. The x-ray may also suggest alternative diagnoses (eg, COPD, pneumonia, idiopathic pulmonary fibrosis, lung cancer).

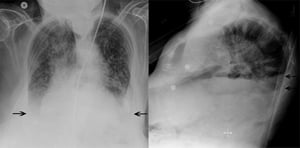
This patient has bilateral pleural effusions (arrows). The normally sharp costophrenic angles are obscured by fluid in this patient.
© 2017 Elliot K. Fishman, MD.

Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thickened, edematous interlobular septa often due to pulmonary edema.
© 2017 Elliot K. Fishman, MD.
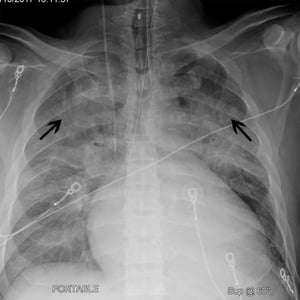
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest x-ray). The patient also has cephalization (black arrows) whereby upper lobe pulmonary vessels become more prominent. These findings are often seen in patients with heart failure.
© 2017 Elliot K. Fishman, MD.
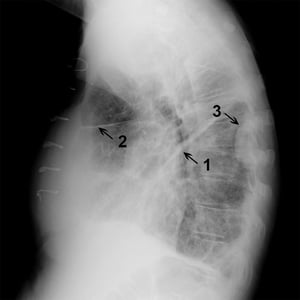
Lateral chest x-ray in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3) seen along right posterior chest wall.
© 2017 Elliot K. Fishman, MD.
This patient has bilateral pleural effusions (arrows). The normally sharp costophrenic angles are obscured by fluid in this patient.
© 2017 Elliot K. Fishman, MD.
Kerley B lines (arrows) are horizontal lines in the lung periphery that extend to the pleural surface. They denote thickened, edematous interlobular septa often due to pulmonary edema.
© 2017 Elliot K. Fishman, MD.
This patient has cardiomegaly (width of cardiac silhouette is > 50% of thoracic cage on a posterior-anterior chest x-ray). The patient also has cephalization (black arrows) whereby upper lobe pulmonary vessels become more prominent. These findings are often seen in patients with heart failure.
© 2017 Elliot K. Fishman, MD.
Lateral chest x-ray in a patient with fluid in major (1) and minor (2) fissures as well as a loculated effusion (3) seen along right posterior chest wall.
© 2017 Elliot K. Fishman, MD.
ECG
ECG findings are not diagnostic, but an abnormal ECG, especially showing previous myocardial infarction, left ventricular hypertrophy, left bundle branch block, or tachyarrhythmia (eg, rapid atrial fibrillation), increases suspicion for HF and may help identify the cause. An entirely normal ECG is uncommon in chronic HF.
Imaging
Echocardiography can help evaluate chamber dimensions, valve function, LVEF, wall motion abnormalities, LV hypertrophy, diastolic function, pulmonary artery pressure, LV and RV filling pressures, RV function, and pericardial effusion. Intracardiac thrombi, tumors, and calcifications within the heart valves, mitral annulus, and aortic wall abnormalities can be detected. Localized or segmental wall motion abnormalities strongly suggest underlying coronary artery disease but can also be present with patchy myocarditis. Doppler or color Doppler echocardiography accurately detects valvular disorders and shunts. The combination of Doppler evaluation of mitral inflow with tissue Doppler imaging of the mitral annulus can help identify and quantify LV diastolic dysfunction and LV filling pressures. Measuring LVEF can distinguish between predominant HFpEF (EF ≥ 50%) and HFrEF (EF ≤ 40%). It is important to re-emphasize that heart failure can occur with a normal LVEF. Speckle-tracking echocardiography (which is useful in detecting subclinical systolic dysfunction and specific patterns of myocardial dysfunction) may become important but currently is routinely reported only in specialized centers.
Radionuclide imaging also can help assess systolic and diastolic function, previous MI (myocardial infarction), and inducible ischemia or myocardial hibernation. It is used most commonly to assess the presence and/or severity of ischemic heart disease and can also be used to quantify left ventricular ejection fraction.
Cardiac MRI provides accurate images of cardiac structures and is becoming more widely available. Cardiac MRI using late gadolinium enhancement imaging (LGE, also called fibrosis or scar imaging) is useful to evaluate the cause of myocardial disease and to detect focal and diffuse myocardial fibrosis. Cardiac amyloidosis, sarcoidosis, hemachromatosis, and myocarditis are causes of HF that can be detected with or suspected by cardiac MRI findings.
Blood tests
Serum BNP levels are often high in heart failure; this finding may help when clinical findings are unclear or other diagnoses (eg, COPD) need to be excluded. It may be particularly useful for patients with a history of both pulmonary and cardiac disorders. NT-pro-BNP, an inactive moiety created when pro-BNP is cleaved, can be used similarly to BNP. However, a normal BNP level does not exclude the diagnosis of heart failure, particularly in patients with HFpEF and/or obesity. In HFpEF, BNP levels tend to be about 50% of those associated with HFrEF (at similar degree of symptoms), and up to 30% of patients with acute HFpEF have a BNP level below the commonly used threshold of 100 pg/mL (100 ng/L). Obesity, which is becoming an increasingly common comorbidity in HF, is associated with reduced BNP production and increased BNP clearance, resulting in lower levels.
Besides BNP, recommended blood tests include complete blood count, creatinine, BUN (blood urea nitrogen), electrolytes (including magnesium and calcium), glucose, albumin, ferritin, and liver tests. Thyroid function tests are recommended for patients with atrial fibrillation and for selected, especially older, patients.Besides BNP, recommended blood tests include complete blood count, creatinine, BUN (blood urea nitrogen), electrolytes (including magnesium and calcium), glucose, albumin, ferritin, and liver tests. Thyroid function tests are recommended for patients with atrial fibrillation and for selected, especially older, patients.
Other tests
Thoracic ultrasonography is a noninvasive method of detecting pulmonary congestion in patients with heart failure. Sonographic "comet tail artifact" on thoracic ultrasonography corresponds to the x-ray finding of Kerley B lines.

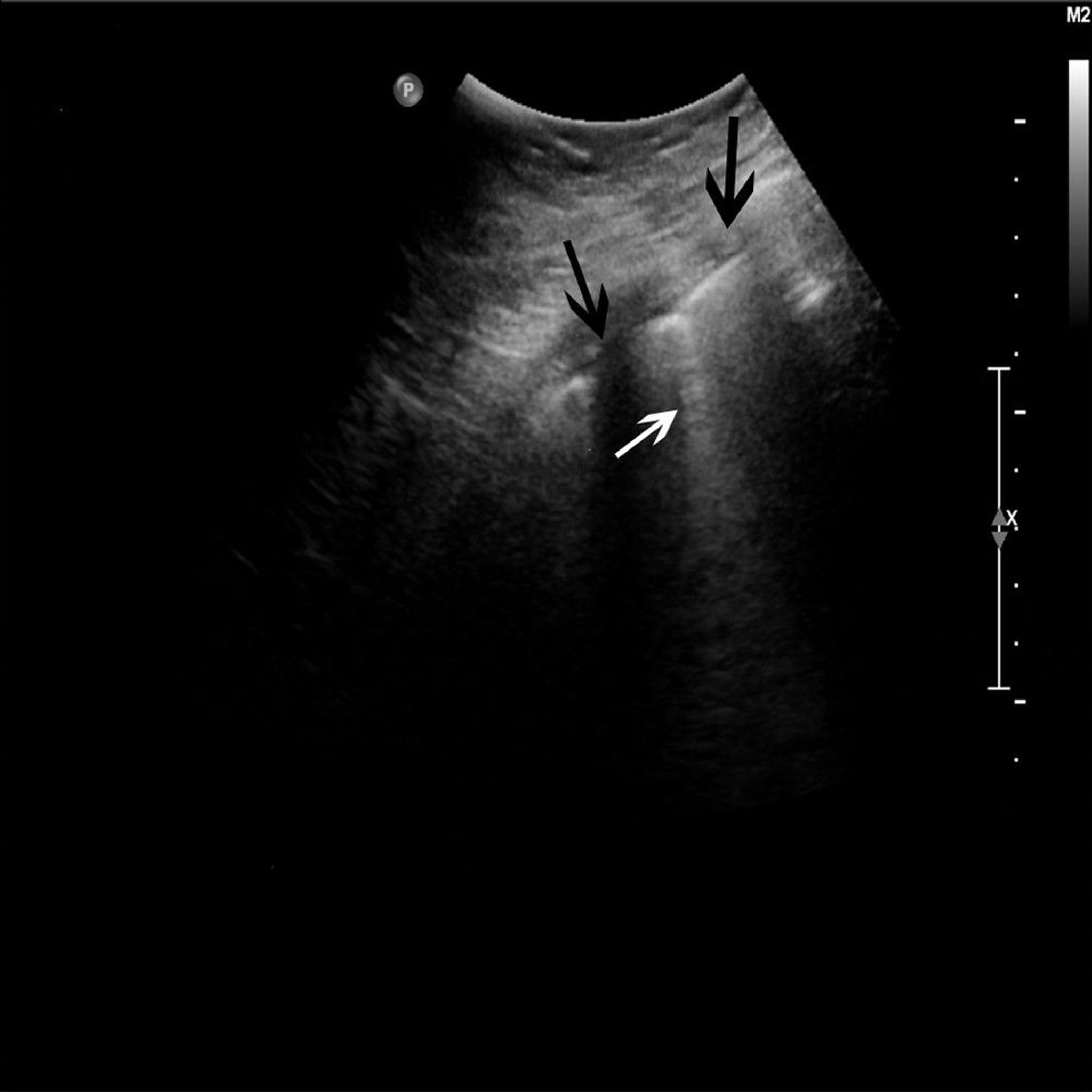
© 2017 Elliot K. Fishman, MD.
Coronary angiography or CT coronary angiography is indicated when coronary artery disease is suspected or the etiology of HF is uncertain.
Cardiac catheterization with intracardiac pressure measurements (invasive hemodynamics) may be helpful in the diagnosis of restrictive cardiomyopathies and constrictive pericarditis. Invasive hemodynamic measurements are also very helpful when the diagnosis of HF is equivocal, particularly in patients with HFpEF. In addition, perturbing the cardiovascular system (eg, exercise testing, volume challenge, drug challenges [eg, nitroglycerin, nitroprusside]) can be very helpful during invasive hemodynamic testing to help diagnose HF.Cardiac catheterization with intracardiac pressure measurements (invasive hemodynamics) may be helpful in the diagnosis of restrictive cardiomyopathies and constrictive pericarditis. Invasive hemodynamic measurements are also very helpful when the diagnosis of HF is equivocal, particularly in patients with HFpEF. In addition, perturbing the cardiovascular system (eg, exercise testing, volume challenge, drug challenges [eg, nitroglycerin, nitroprusside]) can be very helpful during invasive hemodynamic testing to help diagnose HF.
Endocardial biopsy is sometimes done when an infiltrative cardiomyopathy, or acute giant cell myocarditis is strongly suspected but cannot be confirmed with noninvasive imaging (eg, cardiac MRI).
Diagnosis references
1. McDonagh TA, Metra M, Adamo M, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599-3726, 2021. doi: 10.1093/eurheartj/ehab368
2. Heidenreich PA, Bozkurt B, Aguilar D, et al: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145:e876–e894, 2022, doi: 10.1161/CIR.0000000000001062
Prognosis for Heart Failure
Generally, patients with heart failure have a poor prognosis unless the cause is correctable. Overall combined 5 year survival is 35% for patients with HFpEF or HFrEF after an initial hospitalization for heart failure. In overt chronic HF, mortality depends on severity of symptoms and ventricular dysfunction and can range from 10 to 40%/year.
Specific factors that suggest a poor prognosis include hypotension, low ejection fraction, presence of coronary artery disease, troponin release, elevation of BUN, reduced GFR, hyponatremia, and poor functional capacity (eg, as tested by a 6-minute walk test).
BNP, NTproBNP, and risk scores such as the Meta-Analysis Global Group in Chronic Heart Failure (MAGGIC) Risk Score and the Seattle Heart Failure model, are helpful to predict prognosis in HF patients as an overall group, although there is significant variation in survival among individual patients.
HF usually involves gradual deterioration, interrupted by bouts of severe decompensation, and ultimately death, although the time course is being lengthened with modern therapies. However, death can also be sudden and unexpected, without prior worsening of symptoms.
End-of-life care
All patients and family members should be taught about disease progression and the risk of sudden cardiac death. For some patients, improving quality of life is as important as increasing quantity of life. Thus, it is important to determine patients’ wishes about resuscitation (eg, endotracheal intubation, CPR [cardiopulmonary respiration]) if their condition deteriorates, especially when HF is already severe.
All patients should be reassured that symptoms will be relieved, and they should be encouraged to seek medical attention early if their symptoms change significantly. Involvement of pharmacists, nurses, social workers, and clergy (when desired), who may be part of an interdisciplinary team or disease management program already in place, is particularly important in end-of-life care.
Treatment of Heart Failure
Diet and lifestyle changes
Treatment of cause
Drug therapy
Sometimes device therapy (eg, implantable cardioverter-defibrillator, cardiac resynchronization therapy, mechanical circulatory support)
Sometimes cardiac transplantation
Multidisciplinary care
Immediate inpatient treatment is required for patients with acute or worsening heart failure due to certain disorders (eg, acute myocardial infarction, atrial fibrillation with a very rapid ventricular rate, severe hypertension, acute valvular regurgitation), as well as for patients with pulmonary edema, severe symptoms, new-onset HF, or HF unresponsive to outpatient treatment. Patients with mild exacerbations of previously diagnosed HF can be treated at home.
The primary goal is to diagnose and to correct or treat the disorder that led to heart failure.
Short-term goals include relieving symptoms and improving hemodynamics; avoiding hypokalemia, renal dysfunction, and symptomatic hypotension; and correcting neurohumoral activation.
Long-term goals include correcting hypertension, preventing myocardial infarction and progression of atherosclerosis, improving cardiac function, reducing hospitalizations, and improving survival and quality of life.
Treatment involves dietary and lifestyle changes, drugs, devices, and sometimes percutaneous coronary interventions or surgery.
Treatment is tailored to the patient, considering causes, symptoms, and response to drugs, including adverse effects. There are currently several evidence-based therapies for chronic HFrEF (1, 2). There are fewer evidence-based treatments for chronic HFpEF, HFmrEF, acute HF syndromes, and RV failure (3).
See Drugs for Heart Failure for detailed information on drug treatment and the specific drugs and classes.
Disease management
General measures, especially patient and caregiver education and diet and lifestyle modifications, are important for all patients with heart failure.
Education
Sodium restriction
Appropriate weight and fitness levels
Correction of underlying conditions
Patient and caregiver education are critical to long-term success. The patient and family should be involved in treatment choices. They should be taught the importance of drug adherence, warning signs of an exacerbation, and how to link cause with effect (eg, increased salt in the diet with weight gain or symptoms).
Many centers (eg, specialized outpatient clinics) have integrated health care practitioners from different disciplines (eg, HF nurses, pharmacists, social workers, rehabilitation specialists) into multidisciplinary teams or outpatient heart failure management programs. These approaches can improve outcomes and reduce hospitalizations and are most effective in the sickest patients.
Dietary sodium restriction helps limit fluid retention. All patients should eliminate salt in cooking and at the table and avoid salted foods; the most severely ill should limit sodium to < 2 g/day by consuming only low-sodium foods.
Monitoring daily morning weight helps detect sodium and water accumulation early. If weight increases > 2 kg over a few days, patients may be able to adjust their diuretic dose themselves, but if weight gain continues or symptoms occur, patients should seek medical attention.
Intensive case management, particularly by monitoring drug adherence and frequency of unscheduled visits to the physician or emergency department and hospitalizations, can identify when intervention is needed. Specialized HF nurses are valuable in education, follow-up, and dosage adjustment according to predefined protocols.
Patients with atherosclerosis or diabetes should strictly follow a diet appropriate for their disorder. Obesity may cause and always aggravates the symptoms of HF; patients should attain a body mass index (BMI) ≤ 30 kg/m2 (ideally 21 to 25 kg/m2).
Regular light activity (eg, walking), tailored to symptoms, is generally encouraged. Activity prevents skeletal muscle deconditioning, which worsens functional status; however, activity does not appear to improve survival or decrease hospitalizations. Rest is appropriate during acute exacerbations. Formal exercise cardiac rehabilitation is useful for chronic HFrEF and is likely helpful for patients with HFpEF.
Patients should have annual influenza vaccination because influenza can precipitate HF exacerbations, particularly in institutionalized or older patients. Patients should be vaccinated against SARS-CoV-2.
If causes such as hypertension, persistent tachyarrhythmia, severe anemia, hemochromatosis, uncontrolled diabetes, thyrotoxicosis, beriberi, alcohol use disorder, or toxoplasmosis are successfully treated, patients may dramatically improve. Significant myocardial ischemia should be treated aggressively; treatment may include revascularization by percutaneous coronary intervention or bypass surgery. Management of extensive ventricular infiltration (eg, in amyloidosis) has improved considerably. Newer treatments for amyloidosis have markedly improved prognosis for many of these patients.
Arrhythmias
Because arrhythmias can worsen heart failure, it is important to identify and treat the cause of any arrhythmia.
Electrolytes are normalized.
Atrial and ventricular rates are controlled.
Sometimes antiarrhythmic drugs are given.
Sinus tachycardia, a common compensatory change in heart failure, usually subsides when HF treatment is effective. If it does not, associated causes (eg, hyperthyroidism, pulmonary emboli, fever, anemia, pain) should be sought. If sinus tachycardia persists despite correction of causes, a beta-blocker, given in gradually increasing doses, may help selected patients. However, lowering heart rate with a beta-blocker can be detrimental to patients with advanced HFpEF (eg, restrictive cardiomyopathy), in whom stroke volume is fixed because of severe diastolic dysfunction. In these patients, CO is heart rate–dependent, and lowering heart rate can thus lower CO at rest and/or with exertion.
Atrial fibrillation with an uncontrolled ventricular rate must be treated; the target resting ventricular rate is typically < 80 beats/minute. Beta-blockers are the treatment of choice, although rate-limiting calcium channel blockers may be used cautiously if systolic function is preserved. Adding digoxin, low-dose amiodarone, or other rhythm and/or rate controlling drugs may help some patients. Routine conversion to and maintenance of sinus rhythm has not been shown to be superior to rate control alone in large clinical trials. However, it is best to make this determination on a case-by-case basis because some patients improve significantly with restoration of normal sinus rhythm. If rapid atrial fibrillation does not respond to drugs, permanent pacemaker insertion with complete or partial ablation of the atrioventricular node, or other 80 beats/minute. Beta-blockers are the treatment of choice, although rate-limiting calcium channel blockers may be used cautiously if systolic function is preserved. Adding digoxin, low-dose amiodarone, or other rhythm and/or rate controlling drugs may help some patients. Routine conversion to and maintenance of sinus rhythm has not been shown to be superior to rate control alone in large clinical trials. However, it is best to make this determination on a case-by-case basis because some patients improve significantly with restoration of normal sinus rhythm. If rapid atrial fibrillation does not respond to drugs, permanent pacemaker insertion with complete or partial ablation of the atrioventricular node, or otheratrial fibrillation ablation procedures, may be considered in selected patients to restore a sinus or regular rhythm.
Isolated ventricular premature beats, which are common in HF, do not require specific treatment, although rarely very frequent ventricular premature beats (> 15,000/day) have been shown to precipitate heart failure (that reverses with suppression). However, optimization of HF treatments and correction of electrolyte abnormalities (especially potassium and magnesium) reduce the risk of ventricular arrhythmias.
Sustained ventricular tachycardia that persists despite correction of cause (eg, low potassium or magnesium, ischemia) and optimal medical treatment of HF may require an antiarrhythmic drug. Amiodarone, beta-blockers, and dofetilide are the drugs of choice because other antiarrhythmics have adverse proarrhythmic effects when LV systolic dysfunction is present. Because amiodarone increases digoxin and warfarin levels, digoxin and/or warfarin doses should be decreased by half or stopped. Serum digoxin level and INR (international normalized ratio) level should be routinely monitored. However, drug toxicity can occur even at therapeutic levels. Because long-term use of amiodarone can cause adverse effects, a low dose (200 mg orally once a day) is used when possible; blood tests for liver function and thyroid-stimulating hormone are done every 6 months. If chest x-ray is abnormal or dyspnea worsens significantly, chest x-ray and pulmonary function tests are done yearly to check for pulmonary fibrosis. For sustained ventricular arrhythmias, amiodarone may be required; to reduce risk of sudden death, a loading dose of 400 to 800 mg orally twice a day is given for 1 to 3 weeks until rhythm control is adequate, then dose is decreased over 1 month to a maintenance dose of 200 mg orally once a day. that persists despite correction of cause (eg, low potassium or magnesium, ischemia) and optimal medical treatment of HF may require an antiarrhythmic drug. Amiodarone, beta-blockers, and dofetilide are the drugs of choice because other antiarrhythmics have adverse proarrhythmic effects when LV systolic dysfunction is present. Because amiodarone increases digoxin and warfarin levels, digoxin and/or warfarin doses should be decreased by half or stopped. Serum digoxin level and INR (international normalized ratio) level should be routinely monitored. However, drug toxicity can occur even at therapeutic levels. Because long-term use of amiodarone can cause adverse effects, a low dose (200 mg orally once a day) is used when possible; blood tests for liver function and thyroid-stimulating hormone are done every 6 months. If chest x-ray is abnormal or dyspnea worsens significantly, chest x-ray and pulmonary function tests are done yearly to check for pulmonary fibrosis. For sustained ventricular arrhythmias, amiodarone may be required; to reduce risk of sudden death, a loading dose of 400 to 800 mg orally twice a day is given for 1 to 3 weeks until rhythm control is adequate, then dose is decreased over 1 month to a maintenance dose of 200 mg orally once a day.
Device therapy
Use of an implantable cardioverter-defibrillator (ICD) or cardiac resynchronization therapy (CRT) is appropriate for some patients.
An ICD is recommended for patients with an otherwise good life expectancy if they have symptomatic sustained ventricular tachycardia or ventricular fibrillation or if they remain symptomatic and have an LVEF persistently < 35% while receiving guideline-directed medical therapy. The data for ICD use in HFrEF are stronger for ischemic cardiomyopathy than in nonischemic cardiomyopathy. A clinical trial that included HFrEF patients with nonischemic cardiomyopathy demonstrated no mortality benefit from prophylactic (primary prevention) ICD placement (4).
CRT is a mode of pacing that synchronizes contraction of the left ventricle by simultaneously pacing its opposing wall, thereby improving stroke volume. CRT may relieve symptoms and reduce heart failure hospitalizations for patients who have HF, LVEF < 35%, and a widened QRS complex with a left bundle branch block pattern (> 0.15 second—the wider the QRS, the greater potential benefit). CRT devices are effective but expensive, and patients should be appropriately selected. Many CRT devices also incorporate an ICD in their mechanism.
An implantable device that remotely monitors invasive hemodynamics (eg, pulmonary artery pressure) may help guide heart failure management in highly selected patients. For example, drug (eg, diuretic) titration based on readings from one of these devices was associated with a marked reduction in HF hospitalization in one clinical trial that included patients with both HFrEF and HFpEF. The device uses the pulmonary artery diastolic pressure as a surrogate for pulmonary capillary wedge pressure (and hence left atrial pressure) in HF patients. However, it has been evaluated only in NYHA (New York Heart Association) class III patients who had recurrent HF exacerbations. Further evidence will help guide how this technology should be implemented.
Ultrafiltration (venovenous filtration) can be useful in selected hospitalized patients with severe cardiorenal syndrome and volume overload refractory to diuretics. However, ultrafiltration should not be used routinely because clinical trials do not show long-term clinical benefit.
An intra-aortic counterpulsation balloon pump (IABP) is helpful in selected patients with acute HF who have a good chance of recovery (eg, acute HF following myocardial infarction) or in those who need a bridge to a more permanent solution such as cardiac surgery (eg, to fix severe valvular disease or to revascularize multivessel coronary artery disease), an LV assist device, or heart transplantation. Other forms of temporary mechanical circulatory support for patients with acute HF and cardiogenic shock include surgically placed devices such as extracorporeal membrane oxygenation (ECMO, typically venoarterial cannulation) and centrifugal flow ventricular assist devices that can support either the LV, the RV, or both and can also be combined with an oxygenator to provide full cardiopulmonary support. Percutaneously placed devices such as intravascular microaxial ventricular assist devices are available for both LV and RV support. Selection of temporary mechanical circulatory support devices is based mainly on availability and local medical center experience.
Durable or ambulatory LV assist devices (LVADs) are longer-term implantable pumps that augment LV output. They are commonly used to maintain patients with severe HF who are awaiting transplantation and are also used as "destination therapy" (ie, as a long-term or permanent solution) in some patients who are not transplant candidates.
Surgery and percutaneous procedures
Surgery may be appropriate when certain underlying disorders are present. Surgery in patients with advanced HF should be done in a specialized center.
Surgical closure of congenital or acquired intracardiac shunts can be curative.
Coronary artery bypass grafting (CABG) for patients with LV systolic dysfunction secondary to coronary artery disease and evidence of myocardial viability may be beneficial; however, those patients with prior myocardial infarction and non-viable myocardium are less likely to benefit from CABG. Thus, the decision to revascularize a HF patient with multivessel coronary artery disease should be made on a case-by-case basis.
If HF is primarily due to a valvular disorder, valve repair or replacement should be considered. Patients with primary mitral regurgitation are more likely to benefit than patients with mitral regurgitation secondary to LV dilation, in whom poor myocardial function is likely to continue postoperatively. Surgery is preferably done before myocardial dilation and damage become irreversible. More recently, percutaneous mitral valve repair procedure (also called transcatheter end-to-end repair [TEER]), in which a clip is applied to approximate the anterior and posterior mitral leaflets, has been shown to reduce death and HF hospitalization in carefully selected patients with symptomatic HF despite optimal medical management and moderate to severe or severe mitral regurgitation with preserved LV size (end-systolic dimension ≤ 70 mm—5).
Heart transplantation is the treatment of choice for patients < 60 who have severe, refractory HF and no other life-threatening conditions and who are highly adherent to management recommendations. Some older patients (about 60 to 70 years) with otherwise good health are also typically considered if they meet other criteria for transplantation. Survival is 85 to 90% at 1 year, and annual mortality thereafter is about 4%/year; however, mortality rate while waiting for a donor is 12 to 15%. Human organ donation remains low.
Anemia and iron deficiency
Anemia is common among patients with chronic heart failure and is frequently multifactorial. Anemia is associated with worse symptoms and outcomes in HF and so reversible causes should be sought and treated. Iron deficiency is among the most common causes of anemia in HF, and iron replacement therapy should be considered once treatable causes such as blood loss (gastrointestinal or other) have been excluded. Oral iron replacement is often less effective due to poor absorption and other reasons, thus intravenous iron replacement is preferred.
Persistent heart failure
After treatment, symptoms often persist. Reasons include
Persistence of the underlying disorder (eg, hypertension, ischemia/infarction, valvular disease) despite treatment
Suboptimal treatment of heart failure
Drug nonadherence
Excess intake of dietary sodium or alcohol
Presence of an undiagnosed thyroid disorder, anemia, or supervening arrhythmia (eg, atrial fibrillation with rapid ventricular response, intermittent ventricular tachycardia)
Also, drugs used to treat other disorders may interfere with HF treatment. Nonsteroidal anti-inflammatory drugs (NSAIDs), thiazolidinediones (eg, pioglitazone) for diabetes, and short-acting dihydropyridine or nondihydropyridine calcium channel blockers can worsen heart failure and should be avoided unless no alternative exists; patients who must take such drugs should be followed closely.Also, drugs used to treat other disorders may interfere with HF treatment. Nonsteroidal anti-inflammatory drugs (NSAIDs), thiazolidinediones (eg, pioglitazone) for diabetes, and short-acting dihydropyridine or nondihydropyridine calcium channel blockers can worsen heart failure and should be avoided unless no alternative exists; patients who must take such drugs should be followed closely.
Treatment references
1. McDonagh TA, Metra M, Adamo M, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599-3726, 2021. doi: 10.1093/eurheartj/ehab368
2. Heidenreich PA, Bozkurt B, Aguilar D, et al: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145:e876–e894, 2022, doi: 10.1161/CIR.0000000000001062
3. Shah SJ, Kitzman D, Borlaug B, et al: Phenotype-specific treatment of heart failure with preserved ejection fraction: A multiorgan roadmap. Circulation 134(1):73–90, 2016. doi: 10.1161/CIRCULATIONAHA.116.021884
4. Kober L, Thune JJ, Nielsen JC, et al: Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med 375(13):1221–2130, 2016. doi: 10.1056/NEJMoa1608029
5. Stone GW, Lindenfield J, Abraham WT, et al: Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 379(24):2307–2318, 2018. doi: 10.1056/NEJMoa1806640
Key Points
Heart failure (HF) involves ventricular dysfunction that ultimately leads to the heart not providing tissues with adequate blood for metabolic needs.
In heart failure with reduced ejection fraction (HFrEF), the ventricle contracts poorly and empties inadequately; ejection fraction is low.
In heart failure with preserved ejection fraction (HFpEF), ventricular filling is impaired, resulting in increased end-diastolic pressure at rest and/or during exercise; ejection fraction is normal.
Consider HF in patients with exertional dyspnea or fatigue, orthopnea, and/or edema, particularly in those with a history of myocardial infarction, hypertension, or valvular disorders or murmurs.
Do chest x-ray, ECG, BNP levels, and an objective test of cardiac function, typically echocardiography.
Unless adequately treated, HF tends to progress and has a poor prognosis.
Treatment includes education and lifestyle changes, control of underlying disorders, a variety of drugs, and sometimes implantable devices (CRT, ICDs).
More Information
The following are some of the major English-language heart failure guidelines that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
McDonagh TA, Metra M, Adamo M, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36):3599-3726, 2021. doi: 10.1093/eurheartj/ehab368
Heidenreich PA, Bozkurt B, Aguilar D, et al: 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 145:e876–e894, 2022, doi: 10.1161/CIR.0000000000001062







