



Nasopharyngeal airways are flexible tubes with one end flared (hence their synonym: nasal trumpets) and the other end beveled that are inserted, beveled end first, through the nares into the pharynx.


(See also Airway Establishment and Control, How To Do Head Tilt–Chin Lift and Jaw-Thrust Maneuvers, and How to Insert an Oropharyngeal Airway.)
Pharyngeal airways (both nasopharyngeal and oropharyngeal) are a component of preliminary upper airway management for patients with apnea or severe ventilatory failure, which also includes
Proper patient positioning
Manual jaw maneuvers
The goal of all of these methods is to relieve upper airway obstruction caused by a relaxed tongue lying on the posterior pharyngeal wall.
Indications for Nasopharyngeal Airway
Spontaneously breathing patients with soft tissue obstruction of the upper airway
Sometimes for dilation and anesthesia of the nasal passage to prepare for nasotracheal intubation
Nasopharyngeal airways are better tolerated and are preferred rather than oropharyngeal airways for patients who are obtunded with intact gag reflexes.
Nasopharyngeal airways can be used in some settings where oropharyngeal airways cannot, eg, oral trauma or trismus (restriction of mouth opening including spasm of muscles of mastication).
Nasopharyngeal airways may also help facilitate bag-valve-mask ventilation.
Contraindications to Nasopharyngeal Airway
Absolute contraindications:
Suspected cribriform plate (basilar skull) fracture
Passage of the nasopharyngeal airway into the cranial vault through a disrupted cribriform plate has been reported but is rare.
Relative contraindications:
Significant nasal trauma
Complications of Nasopharyngeal Airway
Complications include
Epistaxis
Gagging and the potential for vomiting and aspiration in conscious patients
Sinusitis
Equipment for Nasopharyngeal Airway
Gloves, mask, and gown
Towels, sheets, or commercial devices as needed for placing neck and head into sniffing position
Various sizes of nasopharyngeal airways
Water-soluble lubricant or anesthetic jelly
Suctioning apparatus and Yankauer catheter; Magill forceps (if needed to remove easily accessible foreign bodies and patient has no gag reflex), to clear the pharynx as needed
Nasogastric tube, to relieve gastric insufflation as needed
Additional Considerations for Nasopharyngeal Airway
Two airways, one in each nostril, may be used to improve oxygenation and ventilation.
An oropharyngeal airway may be used concurrently with nasopharyngeal airways.
Nasopharyngeal airways can usually be used even with major facial injuries.
Although topical vasoconstrictors and/or anesthetics are sometimes used, no evidence indicates that they decrease complications or pain.
Relevant Anatomy for Nasopharyngeal Airway
Aligning the external auditory canal with the sternal notch may help open the upper airway and establishes the best position to view the airway if endotracheal intubation becomes necessary.
The degree of head elevation that best aligns the ear and sternal notch varies (eg, none in children with a large occiput, a large degree in obese patients).
Positioning for Nasopharyngeal Airway
The sniffing position—only in the absence of cervical spine injury:
Position the patient supine on the stretcher.
Align the upper airway for optimal air passage by placing the patient into a proper sniffing position. Proper sniffing position aligns the external auditory canal with the sternal notch. To achieve the sniffing position, folded towels or other materials may need to be placed under the head, neck, or shoulders, so that the neck is flexed on the body and the head is extended on the neck. In obese patients, many folded towels or a commercial ramp device may be needed to sufficiently elevate the shoulders and neck. In children, padding is usually needed behind the shoulders to accommodate the enlarged occiput.
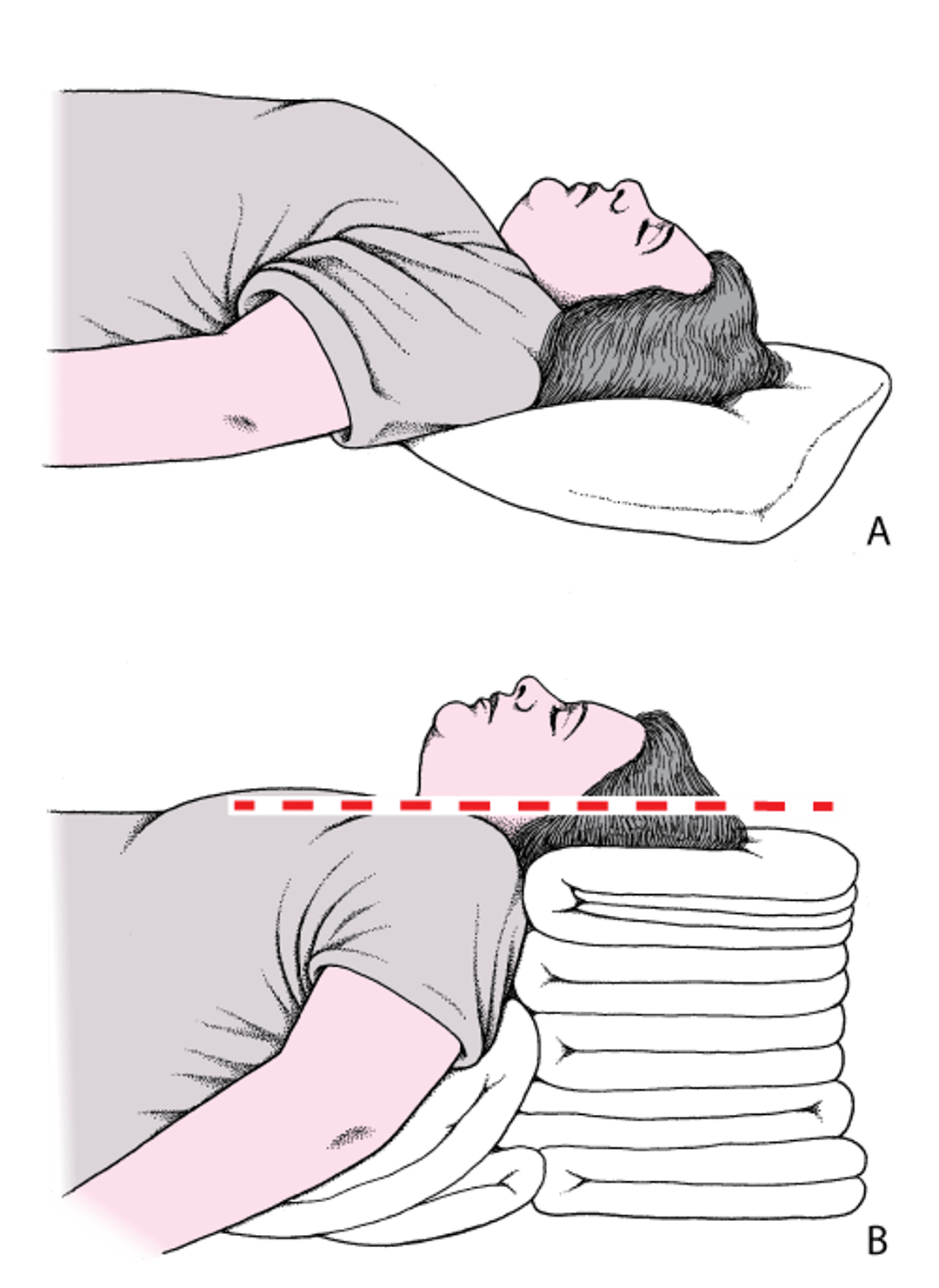
Head and neck positioning to open the airway: Sniffing position
A: The head is flat on the stretcher; the airway is constricted. B: The ear and sternal notch are aligned, with the face parallel to the ceiling (in the sniffing position), opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

If cervical spine injury is a possibility:
Position the patient supine or at a slight incline on the stretcher.
Avoid moving the neck and use only the jaw-thrust maneuver or chin lift without head tilt to manually facilitate opening of the upper airway.
Step-by-Step Description of Nasopharyngeal Airway Procedure
As necessary, clear the oropharynx of obstructing secretions, vomitus, or foreign material.
Determine the appropriate size of the airway. When held against the side of the face, a correctly sized airway will extend from the tip of the nose to the tragus of the ear. Measure the length of the airway to ensure it does not cause obstruction.
Open the nares to reveal the nasal passage. Inspect both nares to determine which side is wider.
Lubricate the nasopharyngeal airway with water-soluble lubricant or anesthetic jelly such as lidocaine gel. Lubricate the nasopharyngeal airway with water-soluble lubricant or anesthetic jelly such as lidocaine gel.
Insert the airway posteriorly (not cephalad) parallel to the floor of the nasal cavity, with the bevel of the tip facing toward the nasal septum (ie, with the pointed end lateral and the open end of the airway facing the septum). Use gentle yet firm pressure to pass the airway through the nasal cavity under the inferior turbinate.
If you encounter resistance, try rotating the airway slightly and re-advance. If the tube still will not pass, try inserting it into the other nostril.
Advance the airway straight back until the flange is resting at the nostril opening.


Aftercare for Nasopharyngeal Airway
Ventilate the patient as appropriate. Use a head tilt–chin lift or jaw-thrust maneuver as necessary to lift the tongue and prevent it from obstructing the nasopharyngeal airway.
Monitor the patient and identify and remediate any impediments to proper ventilation and oxygenation.
Warnings and Common Errors for Nasopharyngeal Airway
Minimize the risk of nasal bleeding by making sure the pointed end of the bevel is not scraping along the nasal septum; the opening should be toward the septum and the pointed end should be lateral.
More Information
The following are some English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Roberts K, Whalley H, Bleetman A: The nasopharyngeal airway: Dispelling myths and establishing the facts. Emerg Med J 22:394-396, 2005.
Roberts K, Porter K: How do you size a nasopharyngeal airway? Resuscitation 56, 2003.







