

Bag-valve-mask (BVM) ventilation is the standard method for rapidly providing rescue ventilation to patients with apnea or severe ventilatory failure.
(See also Airway Establishment and Control, How To Do Head Tilt–Chin Lift and Jaw-Thrust Maneuvers, How To Insert an Oropharyngeal Airway, and How To Insert a Nasopharyngeal Airway.)
Bag-valve-mask ventilation is used to ventilate a patient who is not able to spontaneously breathe on their own to maintain adequate oxygenation and/or ventilation. In BVM ventilation, a self-inflating bag (resuscitator bag) is attached to a nonrebreathing valve and then to a face mask that conforms to the soft tissues of the face. The opposite end of the bag is attached to an oxygen source (100% oxygen) and usually a reservoir bag. The mask is manually held tightly against the face, and squeezing the bag ventilates the patient through the nose and mouth. Unless contraindicated, airway adjuncts such as nasopharyngeal and/or oropharyngeal airways are used during BVM ventilation to assist in creating a patent airway. Positive end expiratory pressure (PEEP) valves should be used to optimize oxygenation if there are no contraindications to its use.
Establishing a patent airway is necessary for BVM ventilation and requires:
Keeping the oropharynx clear of physical obstructions (eg, tongue, soft palate, secretions, vomitus, foreign bodies)
Using proper patient positioning and manual maneuvers to relieve tongue and soft tissue obstruction of the upper airway
Using airway adjuncts such as a nasopharyngeal or oropharyngeal airway to facilitate effective air exchange (see also Airway Establishment and Control)
Successful BVM ventilation requires technical competence and depends on:
Preparing appropriate equipment (resuscitator bag with one-way valve, face mask, oxygen source, PEEP valve, and airway adjuncts)
Establishing and maintaining a patent airway
Establishing and maintaining an adequate mask seal
Using proper manual ventilation technique
Continuing reassessment for adequate ventilation and oxygenation
Rapid provision of successful ventilation and oxygenation is the goal.
Indications for BVM Ventilation
Emergency ventilation for apnea, respiratory failure, or impending respiratory arrest
Pre-ventilation and/or oxygenation or interim ventilation and/or oxygenation during efforts to achieve and maintain definitive artificial airways (eg, endotracheal intubation)
Contraindications for BVM Ventilation
Absolute contraindications:
There is no medical contraindication to providing ventilatory support to a patient; however, ventilatory support should not be initiated if there is a legal contraindication such as a do-not-resuscitate order or other specific advance directive declining ventilatory support.
Relative contraindications:
None
Complications of BVM Ventilation
If BVM ventilation is used for a prolonged period of time or if improperly performed, air may be introduced into the stomach. If air accumulates in the stomach and gastric distention is noted, a nasogastric tube should be inserted to evacuate the accumulated air.
Equipment for BVM Ventilation
Gloves, mask, gown, and eye protection (ie, universal precautions)
Oropharyngeal airways, nasopharyngeal airways, lubricating ointment
Bag-valve-mask device (resuscitator bag with one-way valve and face mask)
Additional sizes of face masks
PEEP valve
Oxygen source (100% oxygen, 15 L/minute)
Nasogastric tube
Suctioning apparatus and Yankauer catheter to suction oral secretion or any liquids in the oropharynx
Magill forceps (if needed to remove easily accessible foreign bodies in the oropharynx)
Pulse oximeter
Capnometer
Additional Considerations for BVM Ventilation
Two-person BVM ventilation should be used whenever possible. Bag-valve-mask ventilation can be done with one person or two, but two-person BVM ventilation is easier and more effective because a tight seal must be achieved and this usually requires 2 hands on the mask.
An airway adjunct is used when performing BVM ventilation unless contraindicated. An oropharyngeal airway is used unless the patient has an intact gag reflex; in such cases, a nasopharyngeal airway (nasal trumpet) is used. Bilateral nasopharyngeal airways and an oropharyngeal airway can be used together to optimize ventilation.
Characteristics that predict difficult BVM ventilation (and can thus help troubleshoot if ventilation is difficult) are described by the mnemonic (in English) MOANS:
M – Mask seal: Facial hair or facial trauma resulting in distorted anatomy can interfere with creating an adequate seal.
O – Obesity/Obstruction: Obesity can be a sign of increased soft tissue in the airway and thus may cause further occlusion when the patient is obtunded. Obstruction by other soft tissues or a foreign body can also prevent adequate ventilation.
A – Age: Extremes of age can predict who may be difficult to ventilate using a BVM due to anatomical changes.
N – No teeth. Performing BVM ventilation on a patient without teeth is usually ineffective; a supraglottic airway may be indicated.
S – Snoring: Snoring respirations can indicate that soft tissue, usually the tongue, is occluding the airway and that repositioning (eg, head tilt–chin lift, jaw thrust) is required.
A positive end expiratory pressure (PEEP) valve may be used during BVM ventilation to improve oxygenation. PEEP can increase alveolar recruitment and thus oxygenation if oxygenation is inadequate even with 100% oxygen due to atelectasis. However, PEEP should be used cautiously in patients who are hypotensive or pre-load dependent because it reduces venous return.
Relevant Anatomy for BVM Ventilation
Aligning the external auditory canal with the sternal notch may help open the upper airway to maximize air exchange and establishes the best position to view the airway if endotracheal intubation becomes necessary.
The degree of head elevation that best aligns the ear and sternal notch varies (eg, no elevation in children with a large occiput, a large degree in patients with obesity).
Positioning for BVM Ventilation
The sniffing position—only in the absence of cervical spine injury:
Position the patient supine on the stretcher.
Align the upper airway for optimal air passage by placing the patient into a proper sniffing position. Proper sniffing position aligns the external auditory canal with the sternal notch. To achieve the sniffing position, folded towels or other materials may need to be placed under the head, neck, or shoulders, so that the neck is flexed on the body and the head is extended on the neck. In patients with obesity, many folded towels or a commercial ramp device may be needed to sufficiently elevate the shoulders and neck. In children, padding is usually needed behind the shoulders to accommodate the enlarged occiput.
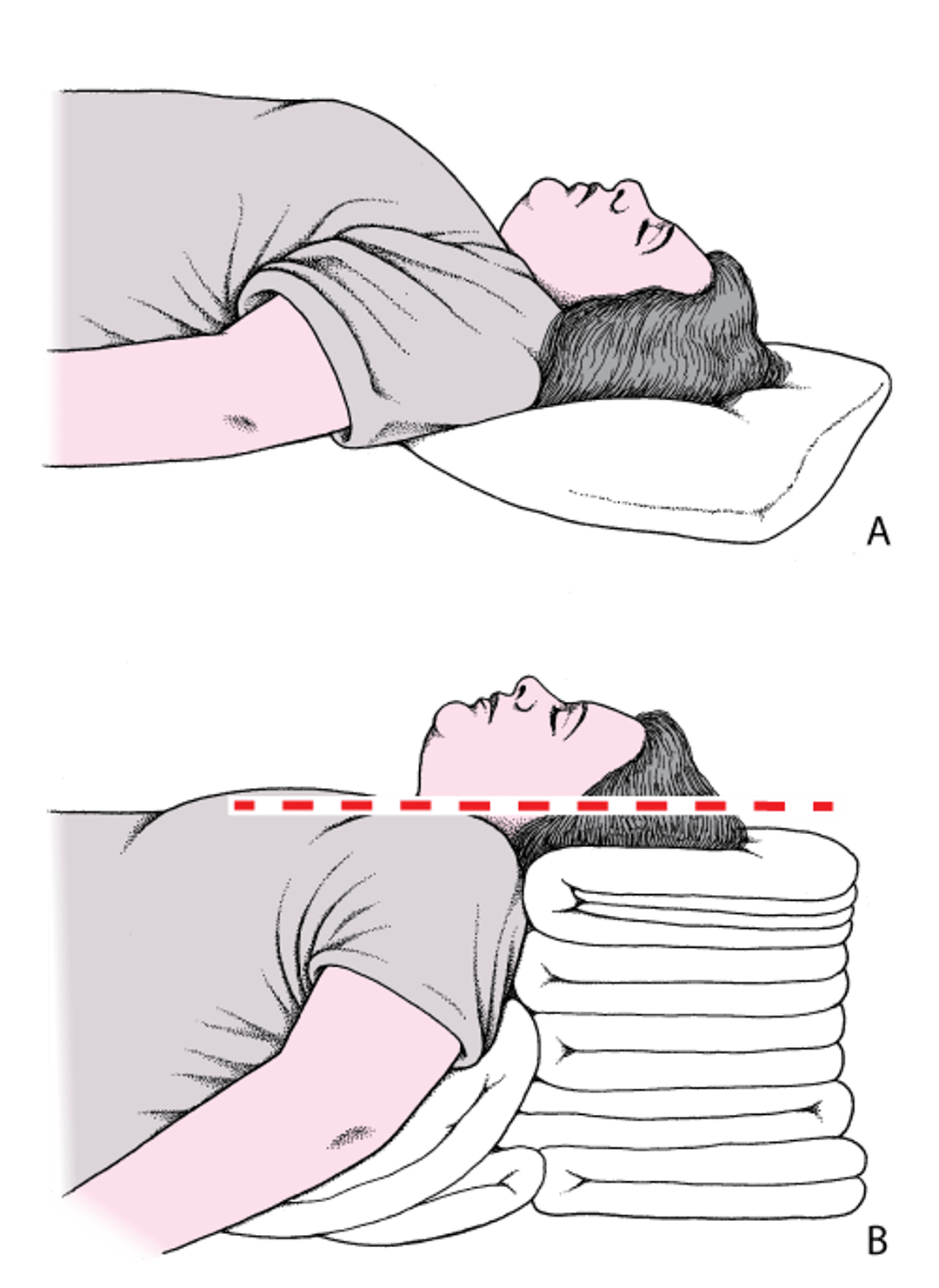
Head and Neck Positioning to Open the Airway: Sniffing Position
A: The head is flat on the stretcher; the airway is constricted. B: The ear and sternal notch are aligned, with the face parallel to the ceiling (in the sniffing position), opening the airway. Adapted from Levitan RM, Kinkle WC: The Airway Cam Pocket Guide to Intubation, ed. 2. Wayne (PA), Airway Cam Technologies, 2007. |

If there is concern for cervical spine injury because of a traumatic injury, evaluate and treat other life-threatening injuries first, and then:
Position the patient supine or at a slight incline on the stretcher.
Stand at the head of the stretcher.
Stabilize the cervical spine by securing the head with one hand on each side of the head.
If a rigid cervical collar is in place, the front of the collar can be removed to allow access to the mandible to perform a jaw thrust maneuver.
Avoid moving the neck and use only the jaw-thrust maneuver or chin lift without head tilt if needed to manually facilitate opening of the upper airway.
Step-by-Step Description of BVM Ventilation
Insert an oropharyngeal airway (if the patient does not have a gag reflex) or 1 to 2 nasopharyngeal airways (if the patient has a gag reflex) prior to bag-valve-mask (BVM) ventilation.
Select the appropriate size mask that fits over the mouth and nose but does not cover the eyes.
Perform two-person BVM ventilation if possible. (NOTE: The accompanying video presents the one-person technique first.)
Two-person mask technique:
In the two-person technique, the more experienced operator handles the mask, because maintaining a proper mask seal is the more difficult task. The second operator squeezes the bag.
Stand at the head of the stretcher and have the second operator stand to either side of the stretcher.
Using both hands, hold the mask between your thumbs and index fingers, which are placed on either side of the connector stem.
Making sure not to place your hands or the mask on the patient’s eyes, first place the nasal portion of the mask over the nose high enough to cover the bridge without air leaks. Next, lower the mask over the chin and allow it to seal along the 2 malar eminences. Cover the bridge of the nose, the 2 malar eminences, and the patient's lower lip with the mask to achieve a proper seal. Stretching the internal portion of the mask before placing it over the nose and mouth can help create a tighter seal.
Traditional hand placement is the "C-E" grip, placing the third, fourth, and fifth fingers (the "E") under the mandible and pulling the mandible upward, while the thumbs and second fingers create a "C" and then press down against the mask.
An alternative method, which may be preferred by clinicians who are less experienced with the two-person technique (1, 2), is to hold the mask to the face with the thenar eminences (muscles at the base of the thumb). Place the thenar eminences (the base of the thumbs in the palm) along each lateral edge of the mask. Then lower the mask onto the face and place the other 4 fingers under the mandible. Press the mask to the face with the thenar eminences while pulling the mandible upward with the fingers. Head tilt may be applied concurrently. This technique is easier to perform; allows the use of stronger hand muscles to maintain a proper seal, minimizing fatigue; and enables 4 fingers rather than 3 to lift the mandible (accomplishing chin lift and jaw thrust).
To assist in maintaining the sniffing position and a patent airway, provide a head tilt-chin lift maneuver by pulling up on the mask and patient’s face with your middle, ring, and little fingers while holding the mask onto the patient’s face, to further open the airway. If your hands are large enough, place your little fingers behind the mandibular rami to do a jaw-thrust maneuver. This re-positioning helps to direct air into the trachea rather than into the esophagus and prevents gastric distention.
Be sure to pull up only on the bony parts of the mandible, because pressure to the soft tissues of the neck or under the chin may obstruct the airway.
Once a proper seal is achieved, have the second operator attach the bag to the mask and begin ventilation.
One-person mask technique:
Using one hand, hold the mask, with your thumb and index finger wrapped around the connector stem of the mask. Most operators use their nondominant hand to grasp the mask, but either hand can be used as long as a good mask seal can be maintained.
Making sure not to place your hand or the mask on the patient’s eyes, first place the nasal portion of the mask over the nose, and then lower the body over the patient’s mouth. The bridge of the nose, the 2 malar eminences, and the mandibular alveolar ridge must be covered by the mask in order to achieve a proper seal.
The third, fourth, and fifth fingers should then be extended underneath the patient’s mandible, pulling it upward into the mask. This maneuver is similar to that of the head tilt–chin lift technique and further opens the airway.
While maintaining this upward traction on the mandible, press the mask downward onto the face to attain a tight mask seal. If your hand is large enough, place your little finger behind the mandibular ramus to do a jaw-thrust maneuver to further open the airway.
Be sure to pull up only on the bony parts of the mandible, because pressure to the soft tissues of the neck or under the chin may obstruct the airway.
Once a proper seal is achieved, use your other hand to begin ventilation.
Bag ventilation and oxygenation:
For each breath, steadily and smoothly squeeze the bag to deliver a tidal volume of 6 to 8 mL/kg (or about 500 mL for an average size adult) over 1 second, and then release the bag to allow it to reinflate. If using a 1000-mL volume bag, squeeze only halfway to deliver the correct tidal volume.
Observe for proper chest rise during ventilations; use a tidal volume just large enough to cause the chest to rise. Allow the chest to fall before delivering the next tidal volume.
With adequate mask seal, there should be minimal air leakage between the mask and the patient's face when the bag is squeezed.
Monitor the patient, checking breath sounds and using capnometry and pulse oximetry (pulse oximetry may not be accurate during cardiac arrest due to poor peripheral perfusion). Adequate ventilation can be confirmed by the presence of end tidal carbon dioxide waveform.
If oxygenation is inadequate despite proper form and use of 100% oxygen, attach a positive end expiratory pressure (PEEP) valve to recruit more alveoli to improve gas exchange. Set the PEEP valve initially at 5 and increase as needed to improve oxygen saturation. However, avoid PEEP in hypotensive patients.
For patients in cardiac arrest cases, do not exceed 8 to 10 breaths per minute (ie, one complete breath every 6 to 7.5 seconds).
For patients not in cardiac arrest, adjust breaths per minute to maintain end tidal carbon dioxide levels between 35 and 45 mm Hg via capnometry.
If gastric distention occurs, place a nasogastric tube to decompress the stomach.
If ventilation or oxygenation is still not adequate, prepare for other airway maneuvers such as a supraglottic airway or endotracheal intubation.


Aftercare for BVM Ventilation
Continue bag-valve-mask (BVM) ventilation until either a definitive artificial airway (eg, endotracheal tube) is achieved or spontaneous ventilation is adequate (eg, following naloxone administration for an opioid overdose).Continue bag-valve-mask (BVM) ventilation until either a definitive artificial airway (eg, endotracheal tube) is achieved or spontaneous ventilation is adequate (eg, following naloxone administration for an opioid overdose).
If a patient becomes more conscious or a gag reflex returns while doing BVM ventilation with an oropharyngeal airway in place, remove the oropharyngeal airway and provide continued treatment as appropriate. A nasopharyngeal airway may be better tolerated in patients with a gag reflex.
If endotracheal intubation is necessary, ventilate using maximum FiO2 through a non-rebreather mask for 3 to 5 minutes if the patient has spontaneous ventilations before intubation if feasible (3); if ventilation is not feasible because intubation must proceed immediately, pre-oxygenate the patient by giving 5 to 8 vital capacity breaths using a PEEP valve.
Warnings and Common Errors for BVM Ventilation
Do not place your hands or the mask on the patient’s eyes. Doing so may damage the eyes or cause a vagal reaction.
Tips and Tricks for BVM Ventilation
Neither excessive force nor rapid insufflation should be used to ventilate; doing so increases gastric distention, compromising ventilation.
A nasogastric tube is inserted to help decompress the stomach when possible.
References
1. Soleimanpour M, Rahmani F, Ala A, et al: Comparison of four techniques on facility of two-hand bag-valve-mask (BVM) ventilation: E-C, thenar eminence, thenar eminence (dominant hand)-E-C (non-dominant hand) and thenar eminence (non-dominant hand) - E-C (dominant hand). J Cardiovasc Thorac Res 8(4):147-151, 2016. doi:10.15171/jcvtr.2016.30
2. Otten D, Liao MM, Wolken R, et al: Comparison of bag-valve-mask hand-sealing techniques in a simulated model. Ann Emerg Med 63(1):6-12.e3, 2014. doi:10.1016/j.annemergmed.2013.07.014
3. Jarvis JL, Gonzales J, Johns D, Sager L: Implementation of a Clinical Bundle to Reduce Out-of-Hospital Peri-intubation Hypoxia. Ann Emerg Med 72(3):272-279.e1, 2018. doi:10.1016/j.annemergmed.2018.01.044
Drugs Mentioned In This Article





