



Colonic diverticulosis is the presence of 1 or more diverticula in the colon. Most diverticula are asymptomatic, but some become inflamed or bleed. Diagnosis is by colonoscopy, capsule endoscopy, barium enema, CT, or MRI. Asymptomatic diverticulosis requires no treatment. When symptoms develop, treatment varies depending on clinical manifestations.


")

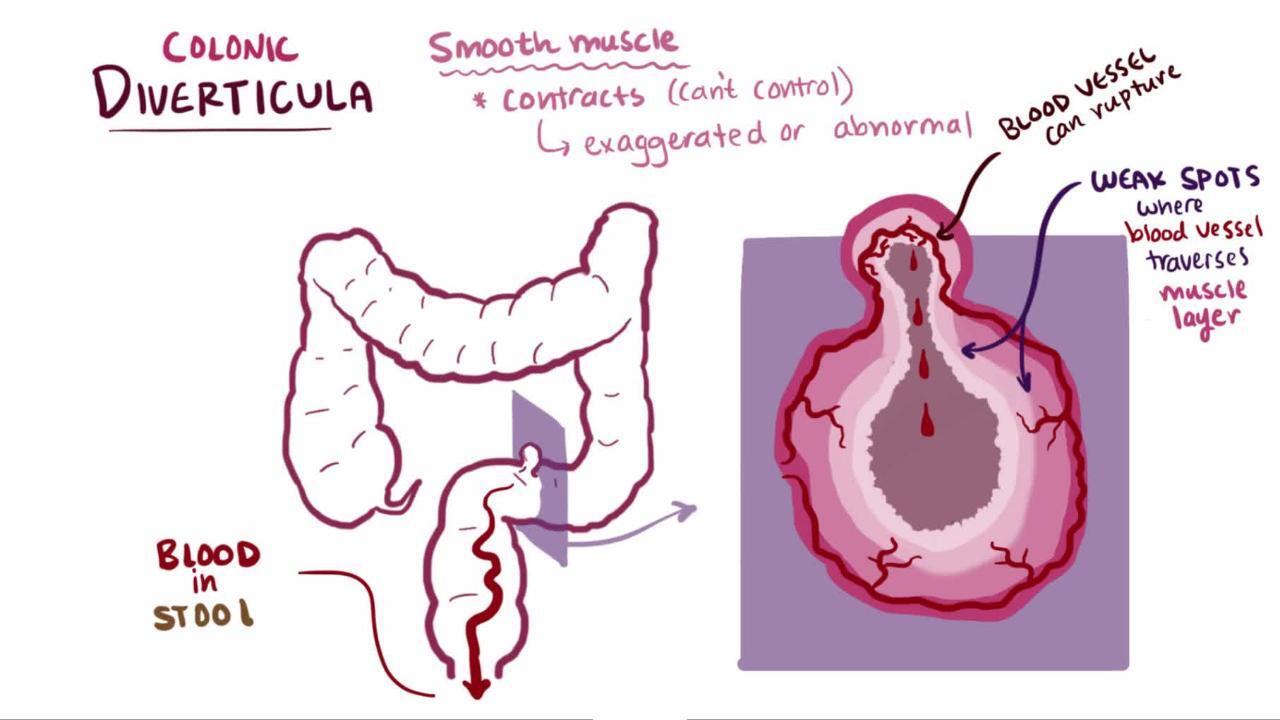
A colonic diverticulum is a saclike pouch of colonic mucosa and submucosa that protrudes through the muscular layer of the colon; because it does not contain all layers of the bowel, it is considered a pseudodiverticulum (see also Definition of Diverticular Disease).

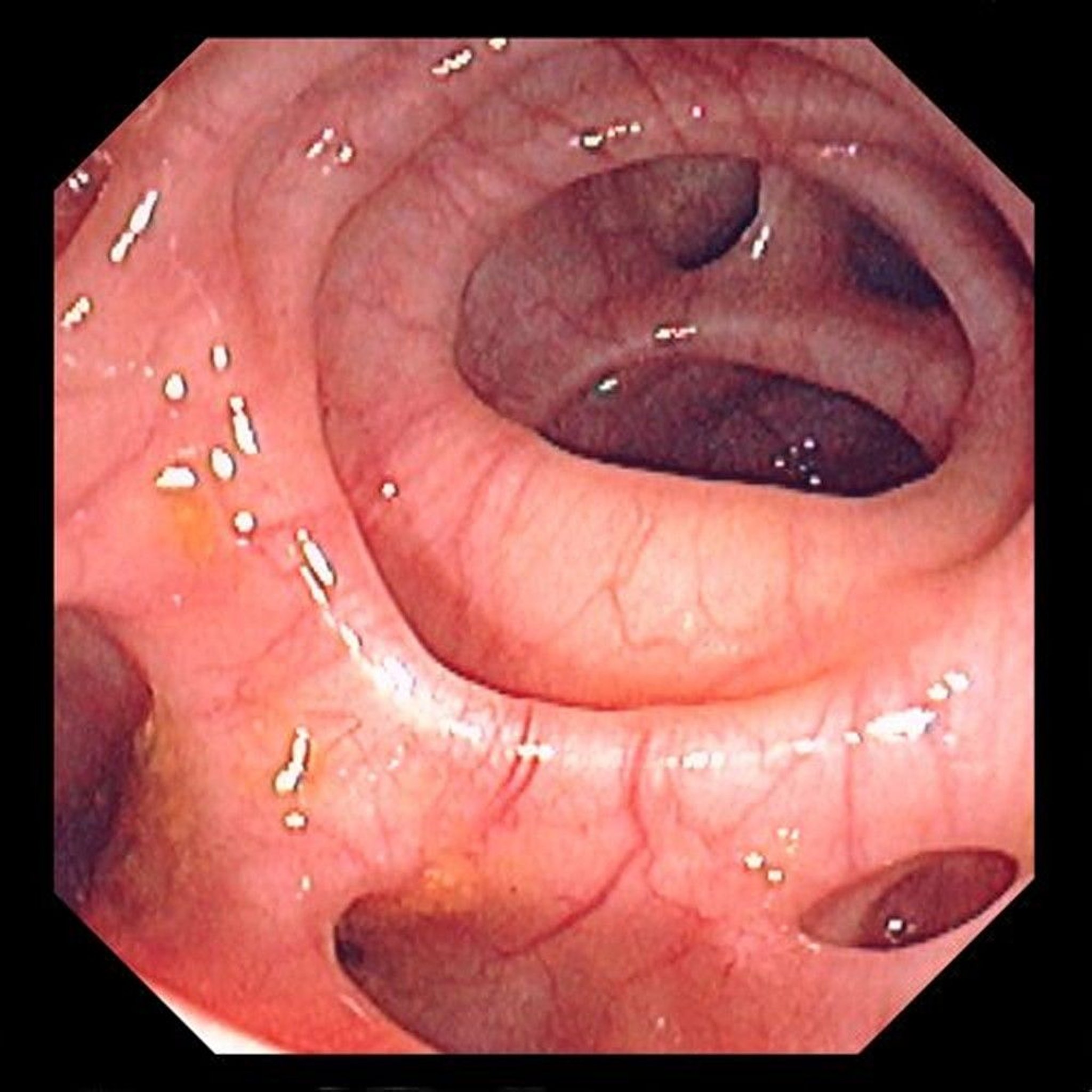
Image provided by David M. Martin, MD.
Although diverticula can occur anywhere in the large bowel, they usually occur in the sigmoid portion of the colon. They rarely occur below the peritoneal reflection and involve the rectum. Diverticula vary in diameter but typically are 3 to 10 mm in size. Giant diverticula, which are extremely rare, are defined as diverticula > 4 cm in diameter; sizes up to 25 cm have been reported. People who have colonic diverticulosis usually have several diverticula.

Diverticulosis becomes more common with increasing age (1).
General reference
1. Tursi A, Scarpignato C, Strate LL, et al. Colonic diverticular disease [published correction appears in Nat Rev Dis Primers. 2020 Apr 29;6(1):35. doi: 10.1038/s41572-020-0176-y] [published correction appears in Nat Rev Dis Primers. 2020 Jun 17;6(1):50. doi: 10.1038/s41572-020-0192-y]. Nat Rev Dis Primers. 2020;6(1):20. Published 2020 Mar 26. doi:10.1038/s41572-020-0153-5
Etiology of Colonic Diverticulosis
The etiology of colonic diverticulosis is multifactorial and not entirely known.
There may be a correlation between symptomatic diverticular disease and environmental factors such as a diet low in fiber or high in red meat, sedentary lifestyle, obesity, smoking, and use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, corticosteroids, and opioids.
Other possible risk factors include heritable factors and alterations in the colonic wall structure and motility.
Diverticula are possibly caused by an increase in intraluminal pressure, which leads to mucosal extrusion through the weakest points of the muscular layer of the bowel—areas adjacent to intramural blood vessels.
The etiology of giant diverticula is unclear. One theory is that a narrow neck-opening leads to a ball-valve effect with intermittent obstruction of the opening, causing the diverticulum to enlarge. A very large giant diverticulum is often a true perforation of a smaller diverticulum that was contained and walled off and became lined mostly by granulation tissue.
Symptoms and Signs of Colonic Diverticulosis
Approximately 80% of patients with diverticulosis are asymptomatic or have only intermittent constipation. Approximately 20% become symptomatic with pain or bleeding when inflammatory or hemorrhagic complications develop (1).
Patients with diverticulosis sometimes develop nonspecific gastrointestinal (GI) symptoms, including abdominal pain, bloating, constipation, diarrhea, and passage of mucus from the rectum. This constellation is sometimes referred to as symptomatic uncomplicated diverticular disease (SUDD). However, some specialists believe these symptoms are due to another disorder (eg, irritable bowel syndrome), and the presence of diverticula is coincidental rather than causal.
Complications of diverticulosis
Complications of colonic diverticular disease are more common among people who smoke, have obesity, have HIV infection, use NSAIDs, or are undergoing cancer chemotherapy. Complications occur in 15 to 20% of patients and include
Diverticular bleeding
Segmental colitis associated with diverticular disease (SCAD)
Diverticulitis is painful inflammation of a diverticulum. It may be uncomplicated or complicated.
Diverticular bleeding occurs in 10 to 15% of patients with diverticulosis.
Segmental colitis associated with diverticular disease (SCAD) refers to manifestations of colitis (eg, hematochezia, abdominal pain, diarrhea) that develop in a few patients with diverticulosis. The degree to which the diverticulosis is causal is unclear.
Diverticular bleeding
Diverticular bleeding is the most common cause (up to 50%) of brisk lower GI bleeding in adults. A study showed that the cumulative incidence of lower GI bleeding from diverticulosis was about 2% at 5 years and 10% at 10 years (2).
The pathophysiology of diverticular bleeding is unknown, but several mechanisms are hypothesized, including
Local trauma from impacted feces in a diverticulum that can erode the adjacent vessel
Enlargement of the diverticulum that can stretch (and ultimately tear) the vessel
NSAIDs have been reported to increase the risk of hemorrhage.
Although most diverticula are in the distal (left) colon, two-thirds of diverticular bleeding occurs from diverticula in the proximal (right) colon (3). Patients with pancolonic diverticulosis have a higher incidence of bleeding.
Diverticular bleeding manifests as painless hematochezia. Because the bleeding vessel is an arteriole, the amount of blood loss is usually moderate to severe. Fresh blood or maroon-colored stool is the typical manifestation; rarely, right-sided diverticular bleeding can manifest as melena. Diverticular bleeding usually occurs without concomitant diverticulitis.

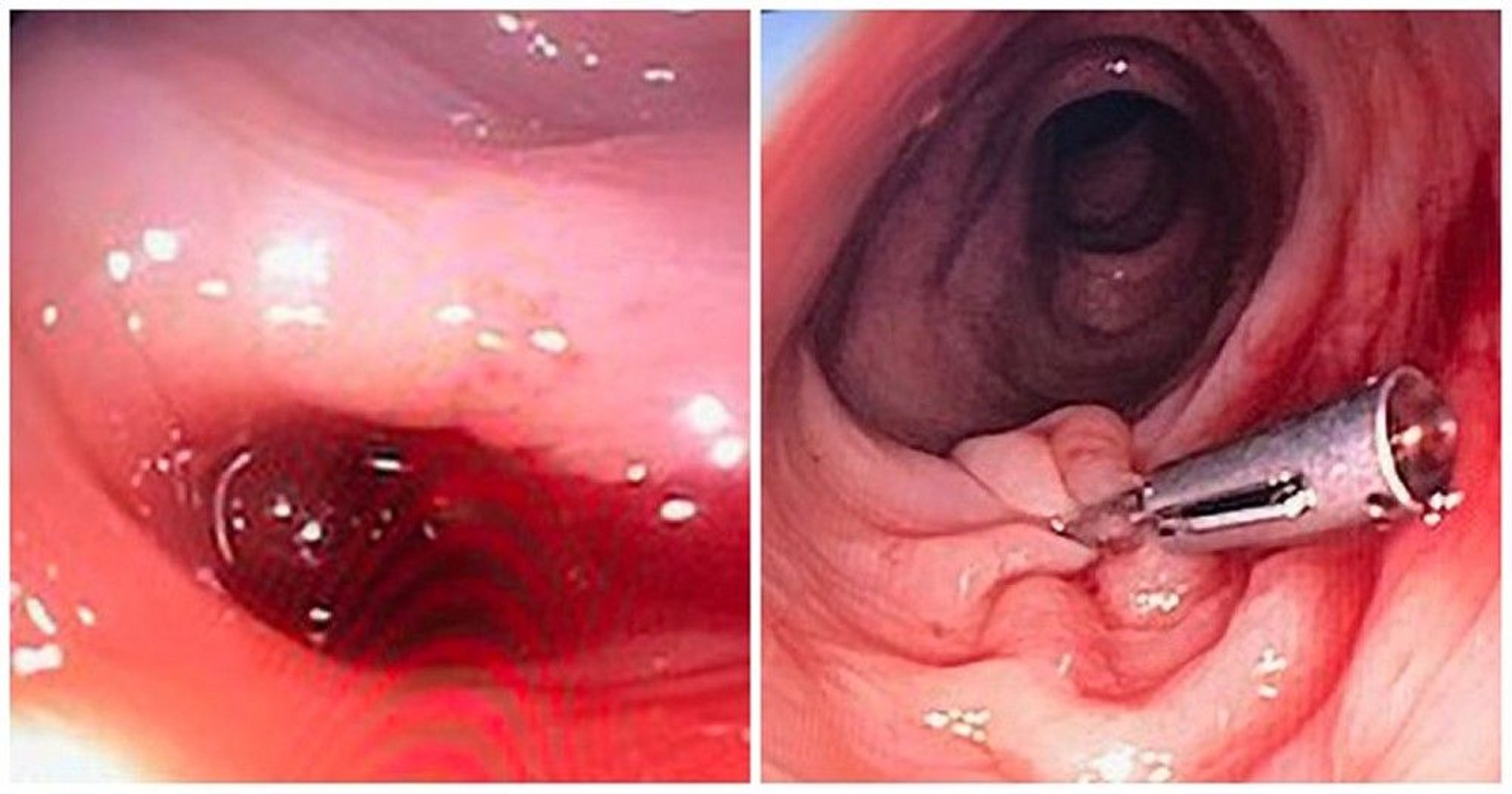
Photos courtesy of Drs. Joel A. Baum and Rafael A. Ching Companioni.
The majority of episodes of bleeding cease spontaneously. The remainder require intervention, typically endoscopic (see also the American College of Gastroenterology's 2023 updated practice guidelines on management of patients with acute lower gastrointestinal bleeding).
Patients who have had a diverticular bleeding episode have an increased risk of rebleeding. After an episode of diverticular bleeding, the risk of rebleeding is as high as 47% within 8 months.
Symptoms and signs references
1. Comparato G, Pilotto A, Franzè A, Franceschi M, Di Mario F. Diverticular disease in the elderly. Dig Dis. 2007;25(2):151-159. doi:10.1159/000099480
2. Niikura R, Nagata N, Shimbo T, et al. Natural history of bleeding risk in colonic diverticulosis patients: A long-term colonoscopy-based cohort study. Aliment Pharmacol Ther 41(9):888–894, 2015. doi: 10.1111/apt.13148
3. Mohammed Ilyas MI, Szilagy EJ. Management of Diverticular Bleeding: Evaluation, Stabilization, Intervention, and Recurrence of Bleeding and Indications for Resection after Control of Bleeding. Clin Colon Rectal Surg. 2018;31(4):243-250. doi:10.1055/s-0037-1607963
Diagnosis of Colonic Diverticulosis
Usually colonoscopy or CT
Asymptomatic diverticula are usually found incidentally during colonoscopy, capsule endoscopy, barium enema, CT, or MRI.

Lower GI bleeding due to diverticulosis is suspected when painless rectal bleeding develops, particularly in an older adult patient or in a patient who has a history of diverticular disease. Evaluation of lower GI bleeding typically includes colonoscopy, which can be done after rapid colonic preparation: 4 to 6 L of polyethylene glycol solution delivered orally, ideally via a nasogastric tube, and given over 3 to 4 hours until the rectal effluent is clear of blood and stool. Endoscopic findings in diverticular bleeding range from active bleeding to a nonbleeding visible vessel (NBVV), an adherent clot that is resistant to washing off, and dark, flat spots. The rate of diagnosing definitive diverticular bleeding is 25% (typically includes colonoscopy, which can be done after rapid colonic preparation: 4 to 6 L of polyethylene glycol solution delivered orally, ideally via a nasogastric tube, and given over 3 to 4 hours until the rectal effluent is clear of blood and stool. Endoscopic findings in diverticular bleeding range from active bleeding to a nonbleeding visible vessel (NBVV), an adherent clot that is resistant to washing off, and dark, flat spots. The rate of diagnosing definitive diverticular bleeding is 25% (1, 2).
If the source cannot be seen with colonoscopy and ongoing bleeding is sufficiently rapid (> 0.5 to 1 mL/minute), CT angiography or radionuclide imaging may localize the source.
Diagnosis references
1. Jensen DM. Endoscopic Diagnosis and Treatment of Colonic Diverticular Bleeding. Gastrointest Endosc Clin N Am. 2024;34(2):345-361. doi:10.1016/j.giec.2023.10.002
2. Sengupta N, Feuerstein JD, Jairath V, et al. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. Am J Gastroenterol. 2023;118(2):208-231. doi:10.14309/ajg.0000000000002130
Treatment of Colonic Diverticulosis
No treatment for asymptomatic diverticulosis
Management of specific symptoms
Diverticular bleeding treated as a lower GI bleed
Asymptomatic diverticulosis requires no treatment or dietary changes. There is no association between consumption of nuts, seeds, corn, or popcorn and diverticulitis, diverticular hemorrhage, or uncomplicated diverticulosis, and avoidance of these foods is no longer recommended. NSAIDs and opioid analgesics may increase the risk of diverticular perforation and bleeding, therefore these medications should be used only with appropriate caution and after extensive discussion with the patient about the risks.
For diverticulosis with nonspecific GI symptoms, treatment is aimed at reducing spasm of a segment of colon. A high-fiber diet is often recommended and may be supplemented by psyllium seed preparations or bran together with adequate fluid intake. However, the role of fiber in the treatment of diverticulosis is limited. In general, data are inadequate to confirm beneficial effects of fiber. Bulk-forming laxatives should be considered for people with constipation (see also the treatment is aimed at reducing spasm of a segment of colon. A high-fiber diet is often recommended and may be supplemented by psyllium seed preparations or bran together with adequate fluid intake. However, the role of fiber in the treatment of diverticulosis is limited. In general, data are inadequate to confirm beneficial effects of fiber. Bulk-forming laxatives should be considered for people with constipation (see also the2019 guidelines for diagnosis and management of diverticular disease from the National Institute for Health and Care Excellence). Antispasmodics (eg, belladonna) are not of benefit and may cause adverse effects. Low-fiber diets are not helpful. Surgery is unwarranted for uncomplicated disease except for giant diverticula.
Pearls & Pitfalls
|
Treatment of diverticular bleeding
Diverticular bleeding stops spontaneously in 75% of patients. Initial management is as for lower GI bleeding. Treatment of diverticular bleeding is often given during the diagnostic procedure.
A colonoscopy should be the first test performed after adequate colon preparation in patients with minor lower GI bleeding and in patients in whom bleeding has clinically ceased. In these patients, observation without colonoscopy should be considered when lower GI bleeding has subsided and when the patient has had, within the year, a well-prepared colonoscopy that showed diverticulosis but no colorectal cancer or other possible etiologies of GI bleeding (eg, angioectasias, postpolypectomy bleeding).
Colonoscopic identification of stigmata of recent hemorrhage (active bleeding, adherent clot, dark spot, and a visible vessel) allows for endoscopic options to control bleeding, including epinephrine injection, application of endoclips or fibrin sealant, heater probe or bipolar coagulation, and band ligation. Both early and late recurring bleeding rates are lower in patients with definitive colonic diverticular bleeding that is treated endoscopically than in those with presumptive colonic diverticular bleeding that is treated conservatively (Colonoscopic identification of stigmata of recent hemorrhage (active bleeding, adherent clot, dark spot, and a visible vessel) allows for endoscopic options to control bleeding, including epinephrine injection, application of endoclips or fibrin sealant, heater probe or bipolar coagulation, and band ligation. Both early and late recurring bleeding rates are lower in patients with definitive colonic diverticular bleeding that is treated endoscopically than in those with presumptive colonic diverticular bleeding that is treated conservatively (1).
CT angiography should be performed initially in patients with ongoing hemodynamically significant lower GI bleeding; however, this test has low diagnostic yield in those with minor bleeding or no clinical evidence of continuing bleeding. During angiography, a number of techniques can be used to control the bleeding, particularly embolization. Embolization is successful approximately 80% of the time. Angiographic complications of bowel ischemia or infarction are less common (< 5%) with current super-selective catheterization techniques (2).
Surgery is rarely needed but is recommended for patients who have had multiple or persistent episodes of diverticular bleeding refractory to therapy or who have hemodynamic instability despite aggressive resuscitation.
If angiography or surgery is being considered, identifying the specific bleeding diverticulum endoscopically or using a nuclear medicine study during active bleeding gives direction to the interventional radiologist and may limit the size of a potential surgical resection. When the bleeding site is known, the need for subtotal colectomy (with its associated higher morbidity and mortality) is markedly reduced because a hemicolectomy or segmental colectomy may be done instead. However, patients who have continued to have a life-threatening hemorrhage and no identifiable bleeding diverticulum may require a subtotal colectomy. Patients with diverticular bleeding who have an unclear localization of the bleeding site have a mortality rate of 43% after colonic surgery, whereas patients who have a defined localization of the bleeding site have a mortality rate of 7% after surgery (3).
Treatment references
1. Gobinet-Suguro M, Nagata N, Kobayashi K, et al. Treatment strategies for reducing early and late recurrence of colonic diverticular bleeding based on stigmata of recent hemorrhage: A large multicenter study. Gastrointest Endosc. 2022;95(6):1210–1222.e12. doi:10.1016/j.gie.2021.12.023
2. Sengupta N, Feuerstein JD, Jairath V, et al. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. Am J Gastroenterol. 2023;118(2):208-231. doi:10.14309/ajg.0000000000002130
3. Schultz JK, Azhar N, Binda GA, et al. European Society of Coloproctology: Guidelines for the management of diverticular disease of the colon. Colorectal Dis. 2020;22(supplement 2):S5–S28. doi:10.1111/codi.15140
Key Points
Colonic diverticula are saclike mucosal pouches that protrude from the colon.
Diverticulosis is increasingly common with age; it is present in over 60% of people older than 70 years.
Diverticulosis is usually asymptomatic, but approximately 20% of patients develop symptoms and/or complications, including inflammation (diverticulitis) and lower gastrointestinal bleeding.
Asymptomatic diverticulosis requires no treatment.
Diverticular bleeding stops spontaneously in most patients; control the remainder during colonoscopy or angiography, or rarely with surgery.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American College of Gastroenterology (ACG): Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline (2023)
National Institute for Health and Care Excellence (NICE): Diverticular disease: Diagnosis and management (2019)
Symptomatic Uncomplicated Diverticular Disease (SUDD)
Symptomatic uncomplicated diverticular disease refers to the presence of persistent and recurrent nonspecific abdominal symptoms in patients with diverticulosis in the absence of overt colitis or diverticulitis.
Some medical authorities consider symptomatic uncomplicated diverticular disease (SUDD) to be a form of irritable bowel syndrome that occurs coincidentally in patients with diverticulosis.
Patients with SUDD have left lower quadrant abdominal pain with bloating, constipation, diarrhea, or passage of mucus from the rectum. In general, patients have a very low incidence of complications.
Diagnosis of SUDD is difficult because the difference between irritable bowel syndrome and SUDD is not well-defined.
There are no strong, evidence-based data regarding treatment of patients with SUDD (1, 2). Some suggestions for symptom control include the use of probiotics, high-fiber diet, gut-directed antibiotics, and mesalazine (3).
References
1. Elisei W, Tursi A. Recent advances in the treatment of colonic diverticular disease and prevention of acute diverticulitis. Ann Gastroenterol. 2016;29(1):24–32. PMID: 26752946
2. Boynton W, Floch M. New strategies for the management of diverticular disease: Insights for the clinician. Therap Adv Gastroenterol. 2013;6(3):205–213. doi:10.1177/1756283X13478679
3. Calini G, Abd El Aziz MA, Paolini L, et al. Symptomatic Uncomplicated Diverticular Disease (SUDD): Practical Guidance and Challenges for Clinical Management. Clin Exp Gastroenterol. 2023;16:29-43. Published 2023 Mar 28. doi:10.2147/CEG.S340929







