

Incompetence of the lower esophageal sphincter allows reflux of gastric contents into the esophagus, causing burning pain. Prolonged reflux may lead to esophagitis, stricture, and rarely metaplasia or cancer. Diagnosis is clinical, sometimes with endoscopy, with or without acid testing. Treatment involves lifestyle modification, acid suppression using proton pump inhibitors, and sometimes surgical repair.
(See also Overview of Esophageal and Swallowing Disorders.)
Gastroesophageal reflux disease (GERD) is common. The prevalence varies widely depending on the population being studied; some estimates range from 10 to 20% of adults (1). It also occurs frequently in infants, typically beginning at birth.
Reference
1. El-Serag HB, Sweet S, Winchester CC, Dent J: Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 63(6):871-880, 2014. doi: 10.1136/gutjnl-2012-304269
Etiology of GERD
The presence of reflux implies lower esophageal sphincter (LES) incompetence, which may result from a generalized loss of intrinsic sphincter tone or from recurrent inappropriate transient relaxations (ie, unrelated to swallowing). Transient LES relaxations are triggered by gastric distention or subthreshold pharyngeal stimulation.
Factors that contribute to the competence of the gastroesophageal junction include the angle of the cardioesophageal junction, the action of the diaphragm, gravity (ie, an upright position), and the patient's age. Factors that may contribute to reflux include weight gain, fatty foods, caffeinated or carbonated beverages, alcohol, tobacco smoking, and medications. Medications that lower LES pressure include anticholinergics, antihistamines, tricyclic antidepressants, calcium channel blockers, progesterone, and nitrates.Factors that contribute to the competence of the gastroesophageal junction include the angle of the cardioesophageal junction, the action of the diaphragm, gravity (ie, an upright position), and the patient's age. Factors that may contribute to reflux include weight gain, fatty foods, caffeinated or carbonated beverages, alcohol, tobacco smoking, and medications. Medications that lower LES pressure include anticholinergics, antihistamines, tricyclic antidepressants, calcium channel blockers, progesterone, and nitrates.
Complications of GERD
GERD may lead to esophagitis, esophageal ulcer, esophageal stricture, Barrett esophagus (replacement of normal squamous epithelium of the distal esophagus with metaplastic columnar epithelium during the healing phase of acute esophagitis), and esophageal adenocarcinoma.
Factors that contribute to the development of esophagitis include the caustic nature of the refluxate, the inability to clear the refluxate from the esophagus, the volume of gastric contents, and local mucosal protective functions. Some patients, particularly infants, may aspirate the reflux material; however, the cause of pulmonary aspiration is rarely GERD.


This image shows grade B esophagitis.
This image shows grade B esophagitis.
Image provided by Kristle Lynch, MD.

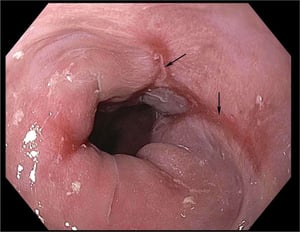
Gastroesophageal reflux may cause esophagitis to manifest as distal esophageal erosions and ulcerations (arrows). Scarring may eventually lead to stricture.
Gastroesophageal reflux may cause esophagitis to manifest as distal esophageal erosions and ulcerations (arrows). Scarr
Image provided by Kristle Lynch, MD.

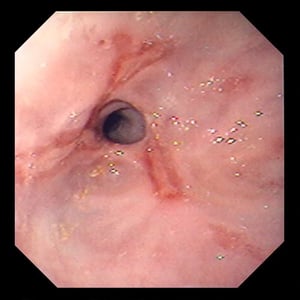
This image shows esophageal stricture caused by longstanding reflux disease and also shows superficial ulcerations.
This image shows esophageal stricture caused by longstanding reflux disease and also shows superficial ulcerations.
Image provided by David M. Martin, MD.


In this image of Barrett esophagus, red-appearing bands of metaplastic epithelium can be seen extending proximally.
In this image of Barrett esophagus, red-appearing bands of metaplastic epithelium can be seen extending proximally.
Image provided by Kristle Lynch, MD.
This image shows grade B esophagitis.
This image shows grade B esophagitis.
Image provided by Kristle Lynch, MD.
Gastroesophageal reflux may cause esophagitis to manifest as distal esophageal erosions and ulcerations (arrows). Scarring may eventually lead to stricture.
Gastroesophageal reflux may cause esophagitis to manifest as distal esophageal erosions and ulcerations (arrows). Scarr
Image provided by Kristle Lynch, MD.
This image shows esophageal stricture caused by longstanding reflux disease and also shows superficial ulcerations.
This image shows esophageal stricture caused by longstanding reflux disease and also shows superficial ulcerations.
Image provided by David M. Martin, MD.
In this image of Barrett esophagus, red-appearing bands of metaplastic epithelium can be seen extending proximally.
In this image of Barrett esophagus, red-appearing bands of metaplastic epithelium can be seen extending proximally.
Image provided by Kristle Lynch, MD.
Symptoms and Signs of GERD
The most prominent symptom of GERD is heartburn, with or without regurgitation of gastric contents into the mouth. Infants present with vomiting, irritability, anorexia, and sometimes symptoms of chronic aspiration. Both adults and infants with chronic aspiration may have cough, hoarseness, or wheezing.
Esophagitis may cause odynophagia and even esophageal hemorrhage, which is usually occult but can be massive. Peptic strictures cause a gradually progressive dysphagia for solid foods. Peptic esophageal ulcers cause the same type of pain as gastric or duodenal ulcers, but the pain is usually localized to the xiphoid or high substernal region. Peptic esophageal ulcers heal slowly, tend to recur, and usually leave a stricture on healing.
Diagnosis of GERD
Clinical diagnosis
Endoscopy for patients not responding to empiric treatment
Advanced pH testing for patients with typical symptoms but normal endoscopy
(See also the American College of Gastroenterology’s 2022 guidelines for the diagnosis and management of gastroesophageal reflux disease.)
A detailed history points to the diagnosis. Patients with typical symptoms of GERD may be given a trial of acid-suppressing therapy. Patients who do not improve, or have long-standing symptoms or symptoms of complications, should undergo further testing.
Endoscopy, with cytologic washings and/or biopsy of abnormal areas, is the test of choice. Endoscopic biopsy is the only test that consistently detects the columnar mucosal changes of Barrett esophagus. Patients with unremarkable endoscopy findings who have typical symptoms despite treatment with proton pump inhibitors should undergo advanced pH testing. Although barium swallow readily shows esophageal ulcers and peptic strictures, it is less useful for mild to moderate reflux; in addition, most patients with abnormalities require subsequent endoscopy. Endoscopic findings can be used to grade the severity of reflux esophagitis (1):
Grade A: One or more mucosal breaks ≤ 5 mm that do not cross the tops of 2 mucosal folds
Grade B: One or more mucosal breaks > 5 mm that do not cross the tops of 2 mucosal folds
Grade C: One or more mucosal breaks that cross ≥ 2 mucosal folds and involve < 75% of the esophageal circumference
Grade D: One or more mucosal breaks involving ≥ 75% of esophageal circumference
Per the Lyon Consensus, grades C and D esophagitis are objective evidence of GERD (2). Esophageal manometry is used to evaluate esophageal peristalsis before surgical treatment.
Diagnosis references
1. Sami SS, Ragunath K: The Los Angeles classification of gastroesophageal reflux disease. Video Journal and Encyclopedia of GI Endoscopy 1(1):103–104, 2013. doi: 10.1016/S2212- 0971(13)70046-3103
2. Gyawali CP, Kahrilas PJ, Savarino E, et al: Modern diagnosis of GERD: The Lyon Consensus. Gut 67(7):1351–1362, 2018. doi: 10.1136/gutjnl-2017-314722
Treatment of GERD
Head of bed elevated
Coffee, alcohol, fats, and smoking avoided
Proton pump inhibitors, H2 blockers
Management of uncomplicated GERD consists of elevating the head of the bed about 15 cm (6 inches) by placing about 15- to 20-cm (6- to 8-inch) blocks under the legs at the head of the bed, by using a wedge pillow, or by placing a wedge under the mattress. Also, the following should be avoided:
Eating within 3 hours of bedtime
Strong stimulants of acid secretion (eg, caffeine, alcohol)Strong stimulants of acid secretion (eg, caffeine, alcohol)
Certain medications (eg, anticholinergics)
Specific foods (eg, fats, chocolate)
Smoking
Weight loss is recommended for patients who are overweight and those who have gained weight recently.
Medical therapy is often with a proton pump inhibitor; some are more potent than others, but all have been shown to be effective. For example, adults can be given oral omeprazole 20 mg, lansoprazole 30 mg, pantoprazole 40 mg, or esomeprazole 40 mg 30 minutes before a meal (eg, before breakfast, or for twice daily dosing, before breakfast and dinner). In some cases (eg, only partial response to once-a-day dosing), proton pump inhibitors may be given twice daily before meals. Infants and children may be given these medications at an appropriate lower single daily dose (ie, omeprazole 20 mg in children Medical therapy is often with a proton pump inhibitor; some are more potent than others, but all have been shown to be effective. For example, adults can be given oral omeprazole 20 mg, lansoprazole 30 mg, pantoprazole 40 mg, or esomeprazole 40 mg 30 minutes before a meal (eg, before breakfast, or for twice daily dosing, before breakfast and dinner). In some cases (eg, only partial response to once-a-day dosing), proton pump inhibitors may be given twice daily before meals. Infants and children may be given these medications at an appropriate lower single daily dose (ie, omeprazole 20 mg in children> 3 years, 10 mg in children < 3 years; lansoprazole 15 mg in children 3 years; lansoprazole 15 mg in children≤ 30 kg, 30 mg in children > 30 kg). These medications may be continued long-term, but the dose should be adjusted to the minimum required to prevent symptoms, including intermittent or as-needed dosing.
H2 blockers are also an effective treatment option for mildly symptomatic GERD. Potassium-competitive acid blockers (eg, vonoprazan) are an emerging therapy available in certain countries but not in the United States. Promotility agents (eg, metoclopramide 10 mg orally 30 minutes before meals and at bedtime) are less effective but may be added to a proton pump inhibitor regimen.H2 blockers are also an effective treatment option for mildly symptomatic GERD. Potassium-competitive acid blockers (eg, vonoprazan) are an emerging therapy available in certain countries but not in the United States. Promotility agents (eg, metoclopramide 10 mg orally 30 minutes before meals and at bedtime) are less effective but may be added to a proton pump inhibitor regimen.
Antireflux surgery (usually fundoplication via laparoscopy) is done in patients with grades C and D esophagitis, large hiatal hernias, hemorrhage, stricture, ulcers, large amounts of symptomatic nonacid reflux, or who cannot tolerate medical therapy. Esophageal strictures are most often managed by repeated endoscopic dilation.
Barrett esophagus may or may not regress with medical or surgical therapy. (See also the American College of Gastroenterology’s updated 2022 guidelines for the diagnosis and management of Barrett’s esophagus.) Because Barrett esophagus is a precursor to adenocarcinoma, endoscopic surveillance for malignant transformation is recommended every 3 to 5 years in nondysplastic disease. The American College of Gastroenterology's 2022 guidelines recommend consideration of endoscopic ablative therapy for patients with confirmed low-grade dysplasia and without life-limiting comorbidity; however, endoscopic surveillance every 12 months is an acceptable alternative. Patients with Barrett esophagus and confirmed high-grade dysplasia should be managed with endoscopic ablative therapy unless they have life-limiting comorbidity. Endoscopic ablative techniques for Barrett esophagus include mucosal resection, photodynamic therapy, cryotherapy, and laser ablation.

Key Points
Lower esophageal sphincter incompetence and transient relaxations allow gastric contents to reflux into the esophagus and rarely into the larynx or lungs.
Complications include esophagitis, esophageal stricture, Barrett esophagus, and esophageal adenocarcinoma.
The main symptom in adults is heartburn, and infants present with vomiting, irritability, anorexia, and sometimes symptoms of chronic aspiration; at any age, chronic aspiration may cause cough, hoarseness, or wheezing.
Diagnose clinically; do endoscopy in patients not responding to empiric treatment and consider advanced pH monitoring if endoscopy is normal in patients with typical symptoms.
Treat with lifestyle changes (eg, head of bed elevation, weight loss, dietary trigger avoidance) and acid-suppressing therapy.
Antireflux surgery can help patients with severe esophagitis, complications of esophagitis, intolerance to medical therapy, or a large amount of symptomatic nonacid reflux.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American College of Gastroenterology: Guidelines for the diagnosis and management of gastroesophageal reflux disease (2022)
American College of Gastroenterology: Updated guidelines for the diagnosis and management of Barrett’s esophagus (2022)
Drugs Mentioned In This Article





