



- Liver Structure and Function
- Evaluation of the Patient With a Liver Disorder
- The Asymptomatic Patient With Abnormal Liver Test Results
- Acute Liver Failure
- Ascites
- Inborn Metabolic Disorders Causing Hyperbilirubinemia
- Jaundice
- Metabolic Dysfunction–Associated Liver Disease (MASLD)
- Portal Hypertension
- Portosystemic Encephalopathy
- Postoperative Liver Dysfunction
- Spontaneous Bacterial Peritonitis (SBP)
- Systemic Abnormalities in Liver Disease
Jaundice is a yellowish discoloration of the skin and mucous membranes caused by hyperbilirubinemia. Jaundice becomes visible when the bilirubin level is about 2 to 3 mg/dL (34 to 51 micromol/L).




(See also Liver Structure and Function and Evaluation of the Patient With a Liver Disorder.)
Pathophysiology of Jaundice
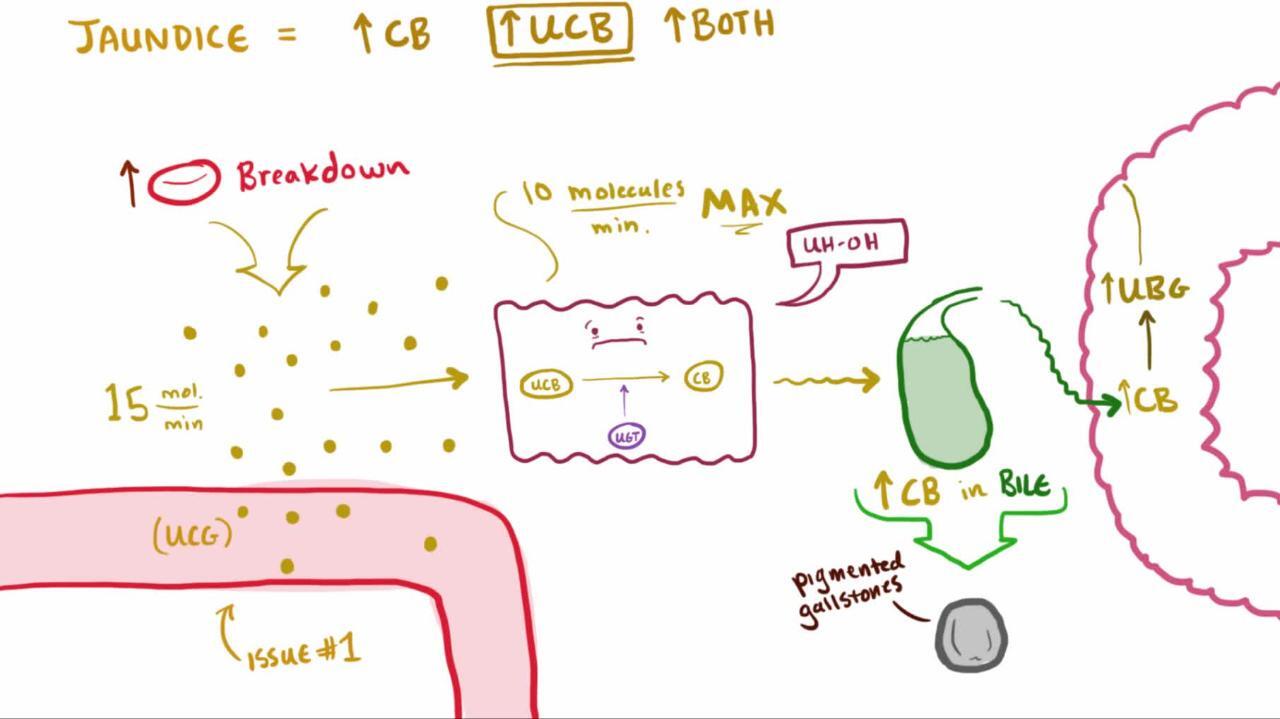
Most bilirubin is produced when hemoglobin (Hb) is broken down into unconjugated bilirubin (and other substances). Unconjugated bilirubin binds to albumin in the blood for transport to the liver, where it is taken up by hepatocytes and conjugated with glucuronic acid to make it water soluble. Conjugated bilirubin is excreted in bile into the duodenum. In the intestine, bacteria metabolize bilirubin to form urobilinogen. Some urobilinogen is eliminated in the feces, and some is reabsorbed, extracted by hepatocytes, reprocessed, and re-excreted in bile (enterohepatic circulation—see Overview of Bilirubin Metabolism ).

Mechanisms of hyperbilirubinemia
Hyperbilirubinemia may involve predominantly unconjugated or conjugated bilirubin.
Unconjugated hyperbilirubinemia is most often caused by ≥ 1 of the following:
Increased production
Decreased hepatic uptake
Decreased conjugation
Conjugated hyperbilirubinemia is most often caused by ≥ 1 of the following:
Dysfunction of hepatocytes (hepatocellular dysfunction)
Slowing of bile egress from the liver (intrahepatic cholestasis)
Obstruction of extrahepatic bile flow (extrahepatic cholestasis)
Consequences
Outcome is determined primarily by the cause of jaundice and the presence and severity of hepatic dysfunction. Hepatic dysfunction can result in coagulopathy, encephalopathy, and portal hypertension (which can lead to gastrointestinal bleeding).
Etiology of Jaundice
Although hyperbilirubinemia can be classified as predominantly unconjugated or conjugated, many hepatobiliary disorders cause both forms.
Many conditions (see table Mechanisms and Some Causes of Jaundice in Adults), including use of certain drugs (see table Some Drugs and Toxins That Can Cause Jaundice), can cause jaundice, but the most common causes overall are
Inflammatory hepatitis (viral hepatitis, autoimmune hepatitis, toxic hepatic injury)
Biliary obstruction
Mechanisms and Some Causes of Jaundice in Adults
Mechanism | Examples | Suggestive Findings* |
|---|---|---|
Unconjugated hyperbilirubinemia | ||
Increased bilirubin production | Common: Hemolysis Less common: Resorption of large hematomas, ineffective erythropoiesis | Few or no clinical manifestations of hepatobiliary disease; sometimes anemia, ecchymoses Serum bilirubin level usually < 3.5 mg/dL (< 59 micromol/L), no bilirubin in urine, normal aminotransferase levels |
Decreased hepatic bilirubin uptake | Common: Heart failure Less common: Drugs, fasting, portosystemic shunts | — |
Decreased hepatic conjugation | Common: Gilbert syndrome Less common: Ethinyl estradiol, Less common: Ethinyl estradiol,Crigler-Najjar syndrome, hyperthyroidism | — |
Conjugated hyperbilirubinemia† | ||
Hepatocellular dysfunction | Common: Drugs, toxins, viral hepatitis Less common: Alcohol-related liver disease, hemochromatosis, primary biliary cholangitis, primary sclerosing cholangitis, steatohepatitis, Wilson disease | Aminotransferase levels usually > 500 U/L (8.35 microkat/L) |
Intrahepatic cholestasis | Common: Alcohol-related liver disease, drugs, toxins, viral hepatitis Less common: Infiltrative disorders (eg, amyloidosis, lymphoma, sarcoidosis, tuberculosis), pregnancy, primary biliary cholangitis, steatohepatitis | Gradual onset of jaundice, sometimes pruritus If severe, clay-colored stools, steatorrhea If long-standing, weight loss Alkaline phosphatase and GGT usually > 3 times normal Aminotransferase levels < 200 U/L (3.34 microkat/L) |
Extrahepatic cholestasis | Common: Common bile duct stone, pancreatic cancer Less common: Acute cholangitis, pancreatic pseudocyst, primary sclerosing cholangitis, common duct strictures caused by previous surgery, other tumors | Depending on cause, manifestations possibly similar to those of intrahepatic cholestasis or a more acute disorder (eg, abdominal pain or vomiting due to a common bile duct stone or acute pancreatitis) Alkaline phosphatase and GGT usually > 3 times normal Aminotransferase levels < 200 U/L (3.34 microkat/L) |
Other, less common mechanisms | Hereditary disorders (mainly Dubin-Johnson syndrome and Rotor syndrome) | Normal liver enzymes |
* Symptoms and signs of the causative disorder may be present. | ||
† Bilirubin is present in urine. | ||
GGT = gamma-glutamyltransferase. | ||
Some Drugs and Toxins That Can Cause Jaundice
Mechanism | Drugs or Toxins |
|---|---|
Increased bilirubin production | Drugs that cause hemolysis (common among patients with glucose-6-phosphate dehydrogenase [G6PD] deficiency), such as sulfa drugs and nitrofurantoin), such as sulfa drugs and nitrofurantoin |
Decreased hepatic uptake | Chloramphenicol, probenecid, rifampinChloramphenicol, probenecid, rifampin |
Decreased conjugation | Ethinyl estradiolEthinyl estradiol |
Hepatocellular dysfunction | Acetaminophen (high dose or overdose)Acetaminophen (high dose or overdose), amiodarone, isoniazid, , amiodarone, isoniazid,nonsteroidal anti-inflammatory drugs, statins, many others, many drug combinations Amanita phalloides mushrooms, carbon tetrachloride, phosphorus (see Hydrocarbon Poisoning and Volatile Solvents) |
Intrahepatic cholestasis | Amoxicillin/clavulanate, Amoxicillin/clavulanate,anabolic steroids, chlorpromazine, pyrrolizidine alkaloids (eg, in , chlorpromazine, pyrrolizidine alkaloids (eg, inherbal preparations), oral contraceptives, phenothiazines |
Evaluation of Jaundice
History
History of present illness should include onset and duration of jaundice. Hyperbilirubinemia can cause urine to darken before jaundice is visible. Therefore, the onset of dark urine indicates onset of hyperbilirubinemia more accurately than onset of jaundice. Important associated symptoms include fever, prodromal symptoms (eg, fever, malaise, myalgias) before jaundice, changes in stool color, pruritus, steatorrhea, and abdominal pain (including location, severity, duration, and radiation). Important symptoms suggesting severe disease include nausea and vomiting, weight loss, and possible symptoms of coagulopathy (eg, easy bruising or bleeding, tarry or bloody stools).
Review of systems should seek symptoms of possible causes, including weight loss and abdominal pain (cancer); joint pain and swelling (autoimmune or viral hepatitis, hemochromatosis, primary sclerosing cholangitis, sarcoidosis); and missed menses (pregnancy).
Past medical history should identify known causative disorders, such as hepatobiliary disease (eg, gallstones, hepatitis, cirrhosis); disorders that can cause hemolysis (eg, hemoglobinopathy, glucose-6-phosphate dehydrogenase [G6PD] deficiency); and disorders associated with liver or biliary disease, including inflammatory bowel disease, infiltrative disorders (eg, amyloidosis, lymphoma, sarcoidosis, tuberculosis), and HIV infection or AIDS.
Drug history should include questions about use of drugs or exposure to toxins known to affect the liver (see table Some Drugs and Toxins That Can Cause Jaundice) and about vaccination against hepatitis.
Surgical history should include questions about previous surgery on the biliary tract (a potential cause of strictures).
Social history should include questions about risk factors for hepatitis (see table Some Risk Factors for Hepatitis), amount and duration of alcohol use, injection drug use, and sexual history.
Family history should include questions about recurrent, mild jaundice in family members and diagnosed hereditary liver disorders. The patient’s history of recreational drug and alcohol use should be corroborated by friends or family members when possible.
Some Risk Factors for Hepatitis
Type of Hepatitis | Risk Factors |
|---|---|
Day care attendance or employment Residence or employment in a closed institution Travel to an endemic area Oral-anal sex Ingestion of raw shellfish | |
Injection drug use Sharing of razor blades or toothbrushes Tattooing Body piercing Absence of vaccination in health care workers High-risk sexual activity Birth in areas of high endemicity | |
Blood transfusion before 1992 Injection drug use Exposure during health care work or sexual activity Date of birth between 1945 and 1965 |
Physical examination
Vital signs are reviewed for fever and signs of systemic toxicity (eg, hypotension, tachycardia).
General appearance is noted, particularly for cachexia and lethargy.
Head and neck examination includes inspection of the sclerae and tongue for icterus and the eyes for Kayser-Fleischer rings (best seen with slit lamp). Mild jaundice is best seen by examining the sclerae in natural light; it is usually detectable when serum bilirubin reaches 2 to 2.5 mg/dL (34 to 43 micromol/L). Breath odor should be noted (eg, for fetor hepaticus).


DR P. MARAZZI/SCIENCE PHOTO LIBRARY
The abdomen is inspected for collateral vasculature, ascites, and surgical scars. The liver is palpated for hepatomegaly, masses, nodularity, and tenderness. The spleen is palpated for splenomegaly. The abdomen is examined for umbilical hernia, shifting dullness, fluid wave, masses, and tenderness. The rectum is examined for gross or occult blood.
Men are checked for testicular atrophy and gynecomastia.
The upper extremities are examined for Dupuytren contractures.
Neurologic examination includes mental status assessment and evaluation for asterixis (a characteristic flapping tremor of the hands).
The skin is examined for jaundice, palmar erythema, needle tracks, vascular spiders, excoriations, xanthomas (consistent with primary biliary cholangitis), paucity of axillary and pubic hair, hyperpigmentation, ecchymoses, petechiae, and purpura.
Red flags
The following findings are of particular concern:
Marked abdominal pain and tenderness
Altered mental status
Gastrointestinal (GI) bleeding (occult or gross)
Ecchymoses, petechiae, or purpura
Interpretation of findings
Severity of illness is indicated mainly by the degree (if any) of hepatic dysfunction. Ascending cholangitis is a concern because it requires emergency treatment.
Severe hepatic dysfunction is indicated by encephalopathy (eg, mental status change, asterixis) or coagulopathy (eg, easy bleeding, purpura, tarry or heme-positive stool), particularly in patients with signs of portal hypertension (eg, abdominal collateral vasculature, ascites, splenomegaly). Massive upper GI bleeding suggests variceal bleeding due to portal hypertension (and possibly coagulopathy).
Ascending cholangitis is suggested by fever and marked, continuous right upper quadrant abdominal pain; acute pancreatitis with biliary obstruction (eg, due to a common duct stone or pancreatic pseudocyst) may manifest similarly.
Cause of jaundice may be suggested by the following:
Acute jaundice in the young and healthy suggests acute viral hepatitis, particularly when a viral prodrome, risk factors, or both are present; however, acetaminophen overdoseacetaminophen overdose is also common.
Acute jaundice after acute drug or toxin exposure in healthy patients is likely to be due to that substance.
A long history of heavy alcohol use suggests alcohol-related liver disease, particularly when typical stigmata are present.
A personal or family history of recurrent, mild jaundice without findings of hepatobiliary dysfunction suggests a hereditary disorder, usually Gilbert syndrome.
Gradual onset of jaundice with pruritus, weight loss, and clay-colored stools suggests intrahepatic or extrahepatic cholestasis.
Painless jaundice in older patients with weight loss and a mass but with minimal pruritus suggests biliary obstruction caused by cancer.
Other examination findings can also be helpful (see table Findings Suggesting a Cause of Jaundice).
Findings Suggesting a Cause of Jaundice
Finding | Possible Causes |
|---|---|
Risk factors | |
Alcohol use (heavy) | Alcohol-related liver disease, including alcoholic hepatitis and cirrhosis |
Gastrointestinal cancer | Extrahepatic biliary obstruction |
Hypercoagulable state | Hepatic vein thrombosis (Budd-Chiari syndrome) |
Inflammatory bowel disease | |
Pregnancy | Intrahepatic cholestasis, steatohepatitis (acute fatty liver due to pregnancy) |
Previous cholecystectomy | Biliary stricture Retained or recurrent common duct stone |
Recent surgery | Benign postoperative intrahepatic cholestasis Lengthy cardiac bypass surgery |
Symptoms | |
Colicky right upper quadrant, right shoulder, or subscapular pain (current or previous) | |
Constant right upper quadrant pain | Acute alcoholic or viral hepatitis, acute cholangitis |
Dark urine | Conjugated hyperbilirubinemia |
Joint pain, swelling, or both | Hepatitis (autoimmune or viral) |
Nausea or vomiting before jaundice | Common bile duct obstruction by a stone (particularly if accompanied by abdominal pain or rigors) |
Pruritus and clay-colored stools | Intrahepatic or extrahepatic cholestasis, possibly severe if stools are clay-colored |
Viral prodrome (eg, fever, malaise, myalgias) | |
Physical examination | |
Abdominal collateral vasculature, ascites, and splenomegaly | Portal hypertension (eg, due to cirrhosis) |
Cachexia in a patient with a hard, lumpy liver | Metastases (common) |
Diffuse lymphadenopathy in a patient with acute jaundice | |
Diffuse lymphadenopathy in a patient with chronic jaundice | |
Dupuytren contractures, palmar erythema, paucity of axillary and pubic hair, and vascular spiders | |
Gynecomastia and testicular atrophy | |
Hyperpigmentation | |
Needle marks | |
Resolving hematoma | Extravasation of blood into tissues |
Xanthomas | |
Testing
The following are done:
Blood tests (bilirubin, aminotransferase, alkaline phosphatase)
Usually imaging
Sometimes biopsy (percutaneous or transjugular approaches)
Blood tests include measurement of total and direct bilirubin, aminotransferase, and alkaline phosphatase levels in all patients. Results help differentiate cholestasis from hepatocellular dysfunction (important because patients with cholestasis usually require imaging tests):
Hepatocellular dysfunction: Marked aminotransferase elevation (> 500 U/L [8.35 microkat/L]) and moderate alkaline phosphatase elevation (< 3 times normal)
Cholestasis: Moderate aminotransferase elevation (< 200 U/L [3.34 microkat/L]) and marked alkaline phosphatase elevation (> 3 times normal)
Also, patients with hepatocellular dysfunction or cholestasis have dark urine due to bilirubinuria because conjugated bilirubin is excreted in urine; unconjugated bilirubin is not. Bilirubin fractionation also differentiates conjugated from unconjugated forms. When aminotransferase and alkaline phosphatase levels are normal, fractionation of bilirubin can help suggest causes, such as Gilbert syndrome or hemolysis (unconjugated) vs Dubin-Johnson syndrome or Rotor syndrome (conjugated).
Other blood tests are done based on clinical suspicion and initial test findings, as for the following:
Signs of hepatic insufficiency (eg, encephalopathy, ascites, ecchymoses) or gastrointestinal (GI) bleeding: Coagulation profile (prothrombin time [PT]/partial thromboplastin time [PTT])
Hepatitis risk factors (see table Some Risk Factors for Hepatitis) or a hepatocellular mechanism suggested by blood test results: Hepatitis viral and autoimmune serologic tests
Fever, abdominal pain, and tenderness: Complete blood count and, if patients appear ill, blood cultures
Suspicion of hemolysis can be confirmed by a peripheral blood smear.
Imaging is done if pain suggests extrahepatic obstruction or cholangitis or if blood test results suggest cholestasis.
Abdominal ultrasonography is usually done first; usually, it is highly accurate in detecting extrahepatic obstruction. CT and MRI are alternatives. Ultrasonography is usually more accurate for gallstones, and CT is more accurate for pancreatic lesions. All these tests can detect abnormalities in the biliary tree and focal liver lesions but are less accurate in detecting diffuse hepatocellular disorders (eg, hepatitis, cirrhosis).
If ultrasonography shows extrahepatic cholestasis, other tests may be necessary to determine the cause; usually, magnetic resonance cholangiopancreatography (MRCP), endoscopic ultrasonography (EUS), or endoscopic retrograde cholangiopancreatography (ERCP) is used. ERCP is more invasive but allows treatment of some obstructive lesions (eg, stone removal, stenting of strictures).
Liver biopsy is not commonly required but can help diagnose certain disorders (eg, disorders causing intrahepatic cholestasis, some kinds of hepatitis, some infiltrative disorders, Dubin-Johnson syndrome, hemochromatosis, Wilson disease). Biopsy can also help when liver enzyme abnormalities are unexplained by other tests.
Laparoscopy (peritoneoscopy) allows direct inspection of the liver and gallbladder without the trauma of a full laparotomy. Unexplained cholestatic jaundice warrants laparoscopy occasionally and diagnostic laparotomy rarely.
Treatment of Jaundice
Treatment of causes and complications
The cause and any complications are treated. Jaundice itself requires no treatment in adults (unlike in neonates—see Neonatal Hyperbilirubinemia). Itching, if bothersome, may be relieved with cholestyramine 2 to 8 g orally twice a day. However, cholestyramine is ineffective in patients with complete biliary obstruction.). Itching, if bothersome, may be relieved with cholestyramine 2 to 8 g orally twice a day. However, cholestyramine is ineffective in patients with complete biliary obstruction.
Geriatrics Essentials: Jaundice
Symptoms may be attenuated or missed in the older patient; eg, abdominal pain may be mild or absent in acute viral hepatitis. A sleep disturbance or mild confusion resulting from portosystemic encephalopathy may be misattributed to dementia.
Key Points
Suspect acute viral hepatitis in patients, particularly young and healthy patients, who have acute jaundice, particularly with a viral prodrome.
Suspect biliary obstruction due to cancer in older patients with painless jaundice, weight loss, an abdominal mass, and minimal pruritus.
Suspect hepatocellular dysfunction if aminotransferase levels are > 500 U/L and alkaline phosphatase elevation is < 3 times normal.
Suspect cholestasis if aminotransferase levels are < 200 U/L and alkaline phosphatase elevation is > 3 times normal.
Hepatic dysfunction is significant if mental status is altered and coagulopathy is present.







