

Parkinson disease is a slowly progressive degenerative disorder of specific areas of the brain. It is characterized by tremor when muscles are at rest (resting tremor), increased muscle tone (stiffness, or rigidity), slowness of voluntary movements, and difficulty maintaining balance (postural instability). In many people, thinking becomes impaired, or dementia develops.
Parkinson disease results from degeneration in the part of the brain that helps coordinate movements.
Often, the most obvious symptom is a tremor that occurs when muscles are relaxed.
Muscles become stiff, movements become slow and uncoordinated, and balance is easily lost.
Doctors base the diagnosis on symptoms.
General measures (such as simplifying daily tasks), medications (such as levodopa plus carbidopa), and sometimes surgery can help, but the disease is progressive, eventually causing severe disability and immobility.General measures (such as simplifying daily tasks), medications (such as levodopa plus carbidopa), and sometimes surgery can help, but the disease is progressive, eventually causing severe disability and immobility.
(See also Overview of Movement Disorders.)
Parkinson disease is the second most common degenerative disorder of the central nervous system after Alzheimer disease.
Parkinson disease commonly begins between the ages of 50 and 79 years. Less commonly, it begins between ages 21 and 40 years and is sometimes called young or early-onset Parkinson disease. Genetic causes are more likely in young and early-onset Parkinson disease; these forms may differ from later-onset Parkinson disease because they progress more slowly, are very sensitive to some medications, and progress more slowly. Rarely, it occurs in children or adolescents.
Parkinsonism has the same symptoms as Parkinson disease, but the symptoms are caused by various other conditions, such as multiple system atrophy, progressive supranuclear palsy, stroke, head injury, or certain medications and other substances. Parkinsonism caused by conditions other than Parkinson disease often involves additional symptoms of another disease (such as severe changes in blood pressure as occurs in multiple system atrophy).
Changes inside the brain
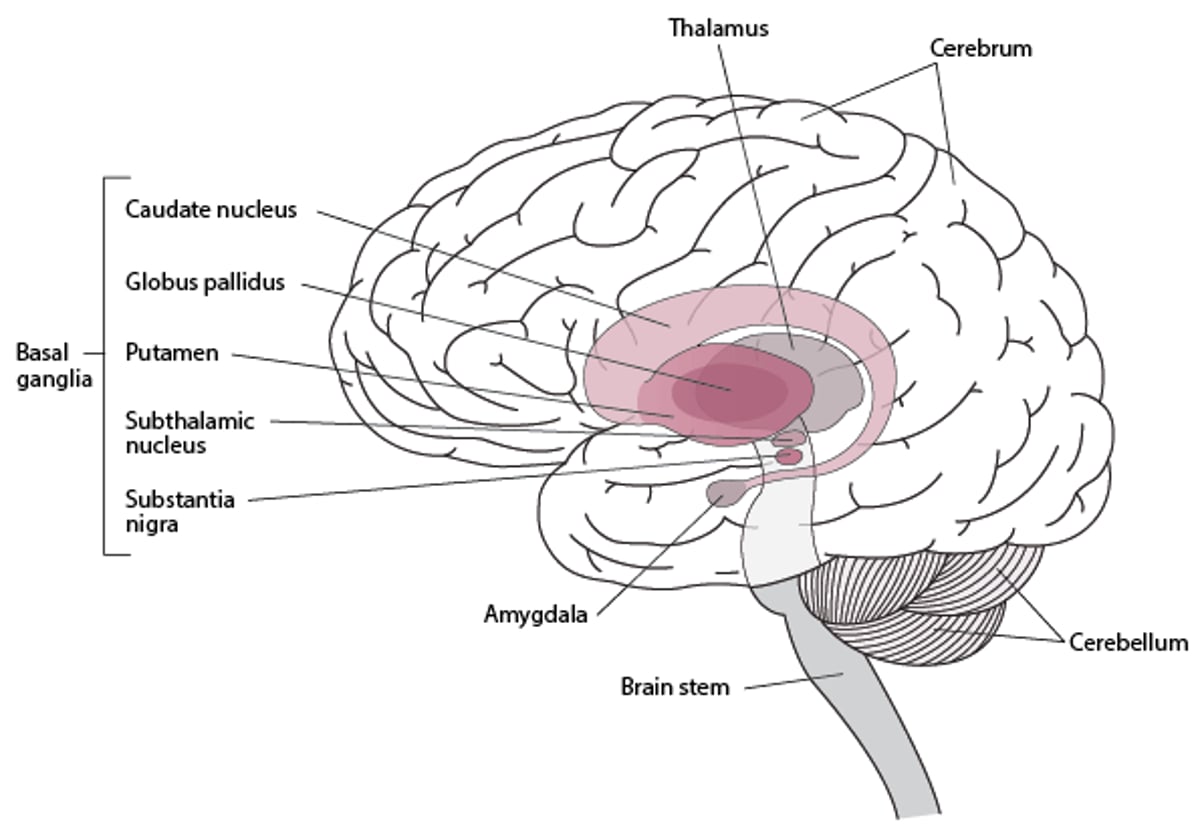
In Parkinson disease, nerve cells in part of the basal ganglia (called the substantia nigra) degenerate.
The basal ganglia are collections of nerve cells located deep within the brain. They help do the following:
Initiate and smooth out intended (voluntary) muscle movements
Suppress involuntary movements
Coordinate changes in posture
When the brain initiates an impulse to move a muscle (for example, to lift an arm), the impulse passes through the basal ganglia. Like all nerve cells, those in the basal ganglia release chemical messengers (neurotransmitters) that trigger the next nerve cell in the pathway to send an impulse. A key neurotransmitter in the basal ganglia is dopamine. Its overall effect is to increase nerve impulses to muscles.
When nerve cells in the basal ganglia degenerate, they produce less dopamine, and the number of connections between nerve cells in the basal ganglia decreases. As a result, the basal ganglia cannot properly control muscle movement, leading to tremor, slow movement (bradykinesia), a tendency to move less (hypokinesia), problems with posture and walking, and some loss of coordination.
Locating the Basal Ganglia
The basal ganglia are collections of nerve cells located deep within the brain. They include the following:
The basal ganglia help initiate and smooth out muscle movements, suppress involuntary movements, and coordinate changes in posture. |

Causes of Parkinson Disease
Usually, no specific cause can be identified.
In Parkinson disease, synuclein (a protein in the brain that helps nerve cells communicate) forms clumps called Lewy bodies in nerve cells. Lewy bodies consist of synuclein that has changed shape (misfolded) and become abnormal. Synuclein can accumulate in several regions of the brain, particularly in the substantia nigra (deep within the cerebrum) and interfere with brain function.
About 25 to 35% of people with Parkinson disease have relatives who have or have had the disease. Also, several gene mutations that can cause Parkinson disease have been identified.
Lewy bodies are also found in parts of the brain in people with neurologic disease whose symptoms are similar to those of patients with Parkinson disease. In dementia with Lewy bodies, Lewy bodies form throughout the outer layer of the brain (cerebral cortex). Lewy bodies may also be involved in Alzheimer disease, possibly explaining why about one-third of people with Parkinson disease have symptoms of Alzheimer disease and why some people with Alzheimer disease develop parkinsonian symptoms.
There is growing evidence that Parkinson disease is part of a more widespread disorder. In this disorder, synuclein accumulates not only in the brain but also in nerve cells in the heart, esophagus, intestines, and elsewhere. As a result, this disorder causes other symptoms such light-headedness when a person stands up, constipation, and difficulty swallowing, depending on where synuclein accumulates.
A head injury or exposure to pesticides may increase the risk of developing Parkinson disease. Consumption of caffeine, smoking, and physical activity may lower risk.
Did You Know...
|
Symptoms of Parkinson Disease
Usually, Parkinson disease begins subtly and progresses gradually.
The first symptoms are usually
Tremors
Problems with movement or a reduced sense of smell
Tremors typically have the following characteristics:
Are coarse and rhythmic
Usually occur in 1 hand while the hand is at rest (a resting tremor)
Often involve the wrist and fingers moving as if they are rolling small objects around (called pill-rolling)
Decrease when the hand is moving purposefully and disappear completely during sleep
May be worsened by emotional stress or fatigue
May eventually progress to the other hand, the arms, and the legs
May also affect the jaws, tongue, forehead, and eyelids and, to a lesser degree, the voice
In some people, a tremor never develops. Sometimes the tremor becomes less obvious as the disease progresses and muscles become stiffer.
Parkinson disease typically also causes the following symptoms:
Stiffness (rigidity): Muscles become stiff, making movement difficult. When a doctor tries to bend the person's forearm back or straighten it out, the arm resists being moved and, when it moves, it starts and stops, as it is being ratcheted (called cogwheel rigidity).
Slowed movements: Movements become slow and smaller and are difficult to initiate. Thus, people tend to move less. When they move less, moving becomes more difficult because joints become stiff and muscles weaken.
Difficulty maintaining balance and posture: Posture becomes stooped, and balance is difficult to maintain. Thus, people tend to topple forward or backward. Because movements are slow, people often cannot move their hands quickly enough to break a fall. These problems tend to develop later in the disease.
Walking becomes difficult, especially taking the first step. Once started, people often shuffle, taking short steps, keeping their arms bent at the waist, and swinging their arms little or not at all. While walking, some people have difficulty stopping or turning. When the disease is advanced, some people suddenly stop walking because they feel as if their feet are glued to the ground (called freezing). Other people unintentionally and gradually quicken their steps, breaking into a stumbling run to avoid falling. This symptom is called festination.
Stiffness and decreased mobility can contribute to muscle ache and fatigue. Having stiff muscles interferes with many movements: turning over in bed, getting in or out of a car, and standing up from a deep chair. Usual daily tasks (such as dressing, combing the hair, eating, and brushing the teeth) take longer.
Because people often have difficulty controlling the small muscles of the hands, daily tasks, such as buttoning a shirt and tying shoelaces, become increasingly difficult. Most people with Parkinson disease have shaky, tiny handwriting (micrographia) because initiating and sustaining each stroke of the pen is difficult. People may mistakenly think of these symptoms as weakness. However, strength and sensation are usually normal.
The face becomes less expressive (masklike) because the facial muscles that control expression do not move as much as they normally would. This lack of expression may be mistaken for depression, or it may cause depression to be overlooked. (Depression is common among people with Parkinson disease.) Eventually, the face can take on a blank stare with the mouth open, and the eyes may not blink often. Often, people drool or choke because the muscles in the face and throat are stiff, making swallowing difficult. People often speak softly in a monotone and may stutter because they have difficulty articulating words.
Parkinson disease also causes other symptoms:
Sleep problems, including insomnia, are common, often because people need to urinate frequently or because symptoms worsen during the night, making turning over in bed difficult. Rapid-eye-movement (REM) sleep behavior disorder commonly develops. In this disorder, the limbs, which normally do not move in REM sleep, may move suddenly and violently because people are acting out their dreams, sometimes injuring a bed partner. Lack of sleep may contribute to depression, impaired thinking, and drowsiness during the day.
Urination problems may occur. Urination may be difficult to start and to maintain (called urinary hesitancy). People may have a compelling need to urinate (urgency). Incontinence is common.
Difficulty swallowing can develop because the esophagus may move its contents more slowly. As a result, people may inhale (aspirate) mouth secretions and/or food they eat or liquids they drink. Aspiration can cause pneumonia.
Constipation can develop because the intestine may move its contents more slowly. Inactivity and levodopa, the main medication used to treat Parkinson disease, can worsen constipation.can develop because the intestine may move its contents more slowly. Inactivity and levodopa, the main medication used to treat Parkinson disease, can worsen constipation.
A sudden, excessive drop in blood pressure when a person stands (orthostatic hypotension) affects almost everyone with Parkinson disease.
Scales (seborrheic dermatitis) develop often on the scalp and face and occasionally in other areas.
Loss of smell (anosmia) is common, but people may not notice it.
Dementia develops in about 25 to 30% of people with Parkinson disease, usually late in the disease. In many others, thinking is impaired, but people may not recognize it.
Depression can develop, sometimes years before people have problems with movement. Depression tends to worsen as Parkinson disease becomes more severe. Depression can also make movement problems worse.
Hallucinations, delusions, and paranoia can occur, particularly if dementia develops. People may see or hear things that are not there (hallucinations) or firmly hold certain beliefs despite clear evidence that contradicts them (delusions). They may become mistrustful and think other people intend them harm (paranoia). These symptoms are considered psychotic symptoms because they represent loss of contact with reality. Psychotic symptoms are the most common reason people with Parkinson disease are put in an institution. Having these symptoms increases the risk of dying.
Mental symptoms, including psychotic symptoms, may be caused by Parkinson disease or by medications used to treat it.
The medications used to treat Parkinson disease (see table ) can also cause problems, such as obsessive-compulsive behavior or difficulty controlling urges, resulting, for example, in compulsive gambling or collecting.
Diagnosis of Parkinson Disease
A doctor's evaluation
Sometimes computed tomography or magnetic resonance imaging
Sometimes use of the medication levodopa to see whether it helpsSometimes use of the medication levodopa to see whether it helps
Parkinson disease is likely if people have the following:
Fewer, slow movements
The characteristic tremor
Muscle rigidity
Clear and long-lasting (sustained) improvement in response to levodopaClear and long-lasting (sustained) improvement in response to levodopa
Mild, early disease may be difficult for doctors to diagnose because it usually begins subtly. Diagnosis is especially difficult in older adults because aging can cause some of the same symptoms as Parkinson disease, such as loss of balance, slow movements, muscle stiffness, and stooped posture. Sometimes essential tremor is misdiagnosed as Parkinson disease.
To exclude other causes of the symptoms, doctors ask about previous disorders, exposure to toxins, and use of drugs that could cause parkinsonism.
Physical examination
During the physical examination, doctors ask people to do certain movements, which can help establish the diagnosis. For example, in people with Parkinson disease, the tremor disappears or lessens when doctors ask them to touch their nose with their finger. Also, people with the disease have difficulty performing rapidly alternating movements, such as placing their hands on their thighs, then rapidly turning their hands over back and forth several times.
Tests
No tests or imaging procedures can directly confirm the diagnosis. However, computed tomography (CT) and magnetic resonance imaging (MRI) may be done to look for a structural disorder that may be causing the symptoms. Single-photon emission computed tomography (SPECT) and positron emission tomography (PET) can detect brain abnormalities typical of the disease. However, SPECT and PET are currently used only in research facilities and do not distinguish Parkinson disease from other disorders that cause the same symptoms (parkinsonism).
If the diagnosis is unclear, doctors may give the person levodopa, a medication used to treat Parkinson disease. If If the diagnosis is unclear, doctors may give the person levodopa, a medication used to treat Parkinson disease. Iflevodopa results in clear improvement, Parkinson disease is likely.
Treatment of Parkinson Disease
General measures to manage symptoms
Physical and occupational therapy
Levodopa/carbidopa and other medicationsLevodopa/carbidopa and other medications
Sometimes surgery (including deep brain stimulation)
General measures used to treat Parkinson disease can help people function better.
Many medications can make movement easier and enable people to function effectively for many years. The mainstay of treatment for Parkinson disease is
Levodopa plus carbidopaLevodopa plus carbidopa
Other medications are generally less effective than levodopa, but they may benefit some people, particularly if levodopa is not tolerated or does not adequately control symptoms. However, no medication can cure the disease.Other medications are generally less effective than levodopa, but they may benefit some people, particularly if levodopa is not tolerated or does not adequately control symptoms. However, no medication can cure the disease.
Two or more medications may be needed. For older adults, starting doses are often reduced and gradually increased as tolerated. Medications that cause or worsen symptoms, particularly antipsychotic medications, are avoided.
The medications used to treat Parkinson disease can have troublesome side effects. If people notice any unusual effects (such as difficulty controlling urges or confusion), they should report them to their doctor. They should not stop taking a medication unless their doctor tells them to. If some medications used to treat Parkinson disease (such as levodopa/carbidopa) are stopped suddenly, they can cause The medications used to treat Parkinson disease can have troublesome side effects. If people notice any unusual effects (such as difficulty controlling urges or confusion), they should report them to their doctor. They should not stop taking a medication unless their doctor tells them to. If some medications used to treat Parkinson disease (such as levodopa/carbidopa) are stopped suddenly, they can causeneuroleptic malignant-like syndrome, with high fever, high blood pressure, muscle stiffness, muscle damage, and confusion. This syndrome can be life threatening.
Deep brain stimulation, a surgical procedure, is considered if people have advanced disease but no dementia or psychiatric symptoms and medications are ineffective or have severe side effects.
General measures
Various simple measures can help people with Parkinson disease maintain mobility and independence:
Continuing to do as many daily activities as possible
Following a program of regular exercise
Simplifying daily tasks—for example, having buttons on clothing replaced with Velcro fasteners or buying shoes with Velcro fasteners
Using assistive devices, such as zipper pulls and button hooks
Physical therapists and occupational therapists can help people learn how to incorporate these measures into their daily activities, as well as recommend exercises to improve muscle tone and maintain range of motion. Therapists may also recommend mechanical aids, such as wheeled walkers, to help people maintain independence.
Simple changes around the home can make it safer for people with Parkinson disease:
Removing throw rugs to prevent tripping
Installing grab bars in bathrooms and railings in hallways and other locations to reduce the risk of falling
For constipation, the following can help:
Consuming a high-fiber diet, including such foods as prunes and fruit juices
Exercising
Drinking plenty of fluids
Using osmotic laxatives (such as polyethylene glycol), stool softeners (such as senna concentrate), supplements (such as psyllium), or stimulant laxatives (such as bisacodyl taken by mouth) to keep bowel movements regularUsing osmotic laxatives (such as polyethylene glycol), stool softeners (such as senna concentrate), supplements (such as psyllium), or stimulant laxatives (such as bisacodyl taken by mouth) to keep bowel movements regular
Difficulty swallowing may limit food intake, so the diet must be nutritious. Making an effort to sniff more deeply may improve the ability to smell, enhancing the appetite.
Levodopa/carbidopa
Levodopa, which is given with carbidopa, is the first medication used to treat Parkinson disease. These medications, taken by mouth, are the mainstay of treatment for Parkinson disease.Levodopa, which is given with carbidopa, is the first medication used to treat Parkinson disease. These medications, taken by mouth, are the mainstay of treatment for Parkinson disease.
Levodopa may have side effects and become less effective over time as the Parkinson disease worsens. Other medications may be used and include amantadine and Levodopa may have side effects and become less effective over time as the Parkinson disease worsens. Other medications may be used and include amantadine anddopamine agonists (medications that act like dopamine, stimulating the same receptors on brain cells). Such medications are used because production of dopamine is decreased in Parkinson disease.
Levodopa reduces muscle stiffness, improves movement, and often substantially reduces tremor. Taking levodopa produces dramatic improvement in people with Parkinson disease. The medication enables many people with mild disease to return to a nearly normal level of activity and enables some people who are confined to bed to walk again.
Levodopa rarely helps people who have other disorders that can cause symptoms similar to those of Parkinson disease (parkinsonism), such as multiple system atrophy and progressive supranuclear palsy.
Levodopa is a dopamine precursor. That is, it is converted into dopamine in the body. Conversion occurs in the basal ganglia, where levodopa helps compensate for the decrease in dopamine due to Parkinson disease. However, before levodopa reaches the brain, some of it is converted to dopamine in the intestine and in the blood, which increases the risk of side effects such as vomiting, orthostatic hypotension, and flushing. Carbidopa is given with levodopa to prevent in the intestine and in the blood, which increases the risk of side effects such as vomiting, orthostatic hypotension, and flushing. Carbidopa is given with levodopa to preventlevodopa from being converted to dopamine before it reaches the basal ganglia. As a result, there are fewer side effects, and more dopamine is available to the brain.
Domperidone, like carbidopa, reduces the amount of levodopa that is converted into dopamine in the intestine and cardiovascular system (heart and blood vessels). Domperidone is not readily available in the United States.
To determine the best dose of levodopa for a particular person, doctors must balance control of the disease with the development of side effects, which may limit the amount of levodopa the person can tolerate. These side effects include
Nausea
Vomiting
Light-headedness
Involuntary movements (of the mouth, face, and limbs) called dyskinesias
Nightmares
Hallucinations and paranoia (psychotic symptoms)
Changes in blood pressure
Confusion
Obsessive or compulsive behavior or difficulty controlling urges, for example, resulting in compulsive gambling or uncontrollable spending
Occasionally, levodopa is needed to maintain movement even though it is causing hallucinations, paranoia, or confusion. In such cases, certain antipsychotic medications (such as quetiapine, clozapine, or pimavanserin) are used to lessen these side effects. (such as quetiapine, clozapine, or pimavanserin) are used to lessen these side effects.
After taking levodopa for 5 or more years, more than half the people begin to alternate rapidly between a good response to the medication and no response—called on-off effects. Within seconds, people may change from being fairly mobile to being severely impaired and immobile. The periods of mobility after each dose become shorter, and symptoms may occur before the next scheduled dose—the off effects. Also, symptoms may be accompanied by involuntary movements due to levodopa use, including writhing or hyperactivity. One of the following can be used to control the off effects for a while:for 5 or more years, more than half the people begin to alternate rapidly between a good response to the medication and no response—called on-off effects. Within seconds, people may change from being fairly mobile to being severely impaired and immobile. The periods of mobility after each dose become shorter, and symptoms may occur before the next scheduled dose—the off effects. Also, symptoms may be accompanied by involuntary movements due to levodopa use, including writhing or hyperactivity. One of the following can be used to control the off effects for a while:
Taking lower, more frequent doses
Switching to a form of levodopa that is released more gradually into the blood (a controlled-release formulation)
Adding a dopamine agonist or amantadineagonist or amantadine
However, after 15 to 20 years, the off effects become hard to suppress. Surgery is then considered.
A formulation of levodopa/carbidopa (available in Europe) can be given using a pump connected to a feeding tube inserted in the small intestine. The pump delivers A formulation of levodopa/carbidopa (available in Europe) can be given using a pump connected to a feeding tube inserted in the small intestine. The pump deliverslevodopa continuously, thus keeping the level of medication about the same and making side effects less likely. This formulation is being studied as treatment for people who have severe symptoms that cannot be relieved by medications and who cannot be treated with brain surgery. This formulation appears to greatly reduce the off times and increase quality of life.
Other medications
Other medications are generally less effective than levodopa, but they may benefit some people with Parkinson disease, particularly if Other medications are generally less effective than levodopa, but they may benefit some people with Parkinson disease, particularly iflevodopa is not tolerated or is insufficient.
Amantadine,Amantadine, a medication sometimes used to treat influenza, may be used alone to treat mild Parkinson disease or as a supplement to levodopa. a medication sometimes used to treat influenza, may be used alone to treat mild Parkinson disease or as a supplement to levodopa.Amantadine probably has many effects that make it work. For example, it stimulates nerve cells to release dopamine. It is used most often to help control the involuntary movements (dyskinesias) that are side effects of levodopa. It can also lessen tremors. If used alone, amantadine often loses its effectiveness after several months.
Dopamine agonists, which act like dopamine, may be useful at any stage of the disease. They include
Pramipexole and ropinirole (given by mouth)Pramipexole and ropinirole (given by mouth)
Rotigotine (given through a skin patch)Rotigotine (given through a skin patch)
Apomorphine (injected under the skin)Apomorphine (injected under the skin)
Side effects may limit the use of dopamine agonists taken by mouth. Patients who have Parkinson disease and take these medications have an increased risk of developing compulsive behavior, including compulsive gambling, excessive shopping, and overeating. In such cases, the dose is reduced, or the medication is stopped and another medication substituted.
PramipexolePramipexole and ropiniroleropinirole are given by mouth. They can be used first instead of or with levodopa in people who are under 60 and have early Parkinson disease. However, when used alone they are rarely effective for more than a few years. Or these medications can be used with are given by mouth. They can be used first instead of or with levodopa in people who are under 60 and have early Parkinson disease. However, when used alone they are rarely effective for more than a few years. Or these medications can be used withlevodopa in people with advanced Parkinson disease. These medications are usually taken 3 times a day. Daytime sleepiness is a common side effect.
A rotigotinerotigotine skin patch is applied once a day. The patch is worn continuously for 24 hours, then removed and replaced. The patch should be placed in different locations each day to reduce risk of skin irritation. Rotigotine is used alone, early in the disease.
Because apomorphineapomorphine is quick-acting, it is used to reverse the off effects of levodopa—when movement is difficult to initiate. Thus, this medication is called rescue therapy. It is usually used when people freeze in place, preventing them, for example, from walking. Affected people or another person (such as a family member) can inject apomorphine up to 5 times a day as needed. In some countries, apomorphine is available in a formulation that can be given using a pump to people who have severe symptoms when surgery is not an option. The pump is a small device that can be clipped to a belt or put in a pocket. A small tube from the pump is inserted under the skin. Apomorphine is pumped from the device through the tube under the skin. This system provides apomorphine automatically on a regular schedule.
RasagilineRasagiline and selegilineselegiline belong to a class of medications called monoamine oxidase inhibitors (MAO inhibitors). They slow the breakdown of levodopa into dopamine, thereby prolonging dopamine’s action in the body. These medications can be used alone but are often given to supplement levodopa. Theoretically, if taken with certain foods (such as certain cheeses), beverages (such as red wine), or drugs, MAO inhibitors can have a serious side effect called hypertensive crisis. However, this effect is unlikely when Parkinson disease is being treated because the doses used are low and the type of MAO inhibitor used (MAO type B inhibitors), particularly rasagiline, is less likely to have this effect.
Some anticholinergic medications are effective in reducing the severity of a tremor and can be used in the early stages of Parkinson disease or later to supplement levodopa. Commonly used anticholinergic medications include benztropine and trihexyphenidyl. Anticholinergic medications are particularly useful for very young people whose most troublesome symptom is a tremor. Doctors try to avoid using these medications in older adults because they also have troublesome side effects (such as confusion, drowsiness, dry mouth, blurred vision, dizziness, constipation, difficulty urinating, and loss of bladder control) and because these medications, when taken for a long time, increase the risk of mental decline. They may reduce tremor because they block the action of the neurotransmitter acetylcholine, and tremor is thought to be caused by an imbalance of acetylcholine (too much) and medications are effective in reducing the severity of a tremor and can be used in the early stages of Parkinson disease or later to supplement levodopa. Commonly used anticholinergic medications include benztropine and trihexyphenidyl. Anticholinergic medications are particularly useful for very young people whose most troublesome symptom is a tremor. Doctors try to avoid using these medications in older adults because they also have troublesome side effects (such as confusion, drowsiness, dry mouth, blurred vision, dizziness, constipation, difficulty urinating, and loss of bladder control) and because these medications, when taken for a long time, increase the risk of mental decline. They may reduce tremor because they block the action of the neurotransmitter acetylcholine, and tremor is thought to be caused by an imbalance of acetylcholine (too much) anddopamine (too little).
Occasionally, other medications with anticholinergic effects, including some antihistamines and tricyclic antidepressants, are used, sometimes to supplement levodopa. However, these medications are only mildly effective for treatment of Parkinson disease. Nonetheless, tricyclic antidepressants with anticholinergic effects may be useful in younger people who have depression and Parkinson disease.
Catechol O-methyltransferase (COMT) inhibitors (entacapone, opicapone, and tolcapone) slow the breakdown of (entacapone, opicapone, and tolcapone) slow the breakdown oflevodopa and dopamine, prolonging their effects, and therefore appear to be useful supplements to levodopa. These medications are used only with , prolonging their effects, and therefore appear to be useful supplements to levodopa. These medications are used only withlevodopa. Tolcapone is seldom used because, although rarely, it can damage the liver. However, tolcapone is stronger than other COMT inhibitors and may be useful if off effects are severe or long-lasting.is seldom used because, although rarely, it can damage the liver. However, tolcapone is stronger than other COMT inhibitors and may be useful if off effects are severe or long-lasting.
Medications Used to Treat Parkinson Disease
Medication | Some Side Effects | Comments |
|---|---|---|
Dopamine precursorDopamine precursor | ||
Levodopa (given with carbidopa)Levodopa (given with carbidopa) | For levodopa:For levodopa: Involuntary movements (of the mouth, face, and limbs), nightmares, low blood pressure when a person stands up (orthostatic hypotension), constipation, nausea, drowsiness, confusion, hallucinations, paranoia, palpitations, and flushing If levodopa/carbidopa is suddenly stopped, neuroleptic malignant syndrome (with high fever, high blood pressure, muscle stiffness, muscle damage, and coma), which can be life threateningIf levodopa/carbidopa is suddenly stopped, neuroleptic malignant syndrome (with high fever, high blood pressure, muscle stiffness, muscle damage, and coma), which can be life threatening | Levodopa/carbidopa is the mainstay of treatment. Carbidopa helps increase the effectiveness of levodopa and reduce its side effects. After several years, the effectiveness of the combination may lessen.helps increase the effectiveness of levodopa and reduce its side effects. After several years, the effectiveness of the combination may lessen. |
Antiviral medication | ||
AmantadineAmantadine | Nausea, dizziness, insomnia, anxiety, confusion, edema, difficulty urinating, worsening of glaucoma, and mottled discoloration of the skin due to dilated blood vessels (livedo reticularis) Rarely, when amantadine is stopped or the dose is reduced, neuroleptic malignant syndromeRarely, when amantadine is stopped or the dose is reduced, neuroleptic malignant syndrome | Amantadine can be used alone in the early stages for mild disease but may become ineffective after several months. Later, it is used to supplement levodopa and to lessen involuntary movements due to can be used alone in the early stages for mild disease but may become ineffective after several months. Later, it is used to supplement levodopa and to lessen involuntary movements due tolevodopa. |
Dopamine agonists | ||
ApomorphineApomorphine | Severe nausea, vomiting, and lumps (nodules) under the skin at the injection site | This quick-acting medication is injected under the skin. It is used as rescue therapy to reverse the off effects of levodopa. |
PramipexolePramipexole RopiniroleRopinirole | Drowsiness, nausea, light-headedness (due to orthostatic hypotension), confusion, obsessive-compulsive behavior, new or increased urges (such as gambling), and hallucinations When these medications are suddenly stopped, neuroleptic malignant syndrome | Early in the disease, these medications may be used alone or with small doses of levodopa to possibly delay Early in the disease, these medications may be used alone or with small doses of levodopa to possibly delaylevodopa’s side effects. Later in the disease, dopamine agonists are useful when the on-off effects of levodopa make it less effective. These medications are especially useful in people under 60. |
RotigotineRotigotine | Drowsiness, nausea, light-headedness (due to orthostatic hypotension), confusion, obsessive-compulsive behavior, new or increased urges (such as gambling), hallucinations, weight gain (possibly due to fluid retention), and sometimes skin irritation where the patch is applied | Rotigotine is available as a skin patch. It is used alone, early in the disease. The patch is worn continuously for 24 hours, then removed and replaced. The patch should be placed in different locations each day to reduce risk of irritating the skin, which may become red and itchy. |
MAO-B inhibitors | ||
RasagilineRasagiline | Nausea, insomnia, drowsiness, and swelling due to fluid accumulation (edema) | Rasagiline can be used alone but is often given as a supplement to levodopa. At best, rasagiline is modestly effective. |
SelegilineSelegiline | When given with levodopa, worsening of levodopa's side effects, including nausea, confusion, insomnia, and involuntary movements | Selegiline can be used alone but is often given as a supplement to levodopa. At best, selegiline is modestly effective. |
Anticholinergic medications* | ||
BenztropineBenztropine TrihexyphenidylTrihexyphenidyl Tricyclic antidepressants (such as amitriptyline), used if depression also needs to be treatedTricyclic antidepressants (such as amitriptyline), used if depression also needs to be treated Some antihistamines (such as diphenhydramine)Some antihistamines (such as diphenhydramine) | Drowsiness, confusion, dry mouth, blurred vision, dizziness, constipation, difficulty urinating, loss of bladder control, and impaired regulation of body temperature | Anticholinergic medications may be given alone in the early stages to young people whose most troublesome symptom is tremor. These medications can reduce tremor but do not affect slow movements or relieve muscle stiffness. Doctors try to avoid using these medications in older adults because the side effects are particularly troublesome for older adults. |
COMT inhibitors | ||
EntacaponeEntacapone OpicaponeOpicapone TolcaponeTolcapone | When given with levodopa, possibly worsening of levodopa's side effects, including nausea, confusion, and involuntary movements Diarrhea, back pain, and orange urine Rarely with tolcapone, risk of liver damageRarely with tolcapone, risk of liver damage | COMT inhibitors can be used to supplement levodopa late in the disease and to extend the interval between doses of levodopa. They are used only with levodopa. When tolcapone is used, doctors periodically do blood tests to evaluate how well the liver is functioning and whether it is damaged (liver tests). |
* Anticholinergic medications are seldom used to treat Parkinson disease because they are only mildly effective and have troublesome side effects. | ||
COMT = catechol O-methyltransferase; MAO-B = monoamine oxidase type B. | ||
Deep brain stimulation
People with involuntary movements or on-off effects due to long-term use of levodopa may benefit from deep brain stimulation. Tiny electrodes are surgically implanted in part of the basal ganglia. The electrodes send small amounts of electricity to the specific area of the basal ganglia responsible for the tremors. Magnetic resonance imaging (MRI) or computed tomography (CT) is used to locate the specific area to be stimulated. By stimulating this part, deep brain stimulation often greatly reduces involuntary movements and tremors and shortens the off part of the on-off effects. Deep brain stimulation is available only at special centers.People with involuntary movements or on-off effects due to long-term use of levodopa may benefit from deep brain stimulation. Tiny electrodes are surgically implanted in part of the basal ganglia. The electrodes send small amounts of electricity to the specific area of the basal ganglia responsible for the tremors. Magnetic resonance imaging (MRI) or computed tomography (CT) is used to locate the specific area to be stimulated. By stimulating this part, deep brain stimulation often greatly reduces involuntary movements and tremors and shortens the off part of the on-off effects. Deep brain stimulation is available only at special centers.
Other procedures
High-intensity focused ultrasound uses MRI to identify areas of the brain affected by Parkinson disease. Then concentrated ultrasound waves are applied to the targeted area to destroy it. This procedure does not involve invasive surgery. This procedure can help control tremors and may help treat slowed movements and rigidity.
In some countries, doctors surgically remove a small part of the brain that is severely affected or use a tiny electrical probe to destroy that part of the brain.
These procedures may lessen symptoms.
If these procedures are unsuccessful, deep brain stimulation of a different part of the brain may be done.
Stem cells
Transplantation of stem cells into the brain, once thought to be a possible treatment for Parkinson disease, has been shown to be ineffective and to have troublesome side effects.
Treatment of mental symptoms
Psychotic and other mental symptoms, whether caused by Parkinson disease itself, a medication, or something else, are treated.
Certain antipsychotic medications—quetiapine, clozapine, or pimavanserin—are sometimes used to treat psychotic symptoms in older adults with Parkinson disease and dementia. These medications, unlike other antipsychotics, do not worsen the symptoms of Parkinson disease. They are well-tolerated by younger people and help control the psychotic symptoms that occur in people with Certain antipsychotic medications—quetiapine, clozapine, or pimavanserin—are sometimes used to treat psychotic symptoms in older adults with Parkinson disease and dementia. These medications, unlike other antipsychotics, do not worsen the symptoms of Parkinson disease. They are well-tolerated by younger people and help control the psychotic symptoms that occur in people withParkinson disease dementia or that may be caused by some of the medications used to treat Parkinson disease. Clozapine is most effective, but its use is limited because it has serious side effects (such as a low white blood cell count) and requires frequent blood tests to check for these effects. Recent evidence suggests that pimavanserin can effectively treat psychotic symptoms without worsening the symptoms of Parkinson disease. Also, frequent blood tests are not required.or that may be caused by some of the medications used to treat Parkinson disease. Clozapine is most effective, but its use is limited because it has serious side effects (such as a low white blood cell count) and requires frequent blood tests to check for these effects. Recent evidence suggests that pimavanserin can effectively treat psychotic symptoms without worsening the symptoms of Parkinson disease. Also, frequent blood tests are not required.
Antidepressants are used to treat depression. Antidepressants with anticholinergic effects (such as amitriptyline) are sometimes used. They may also help lessen the tremor. However, many other antidepressants are very effective and have fewer side effects. They include selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine, paroxetine, citalopram, and escitalopram, and other Antidepressants are used to treat depression. Antidepressants with anticholinergic effects (such as amitriptyline) are sometimes used. They may also help lessen the tremor. However, many other antidepressants are very effective and have fewer side effects. They include selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine, paroxetine, citalopram, and escitalopram, and otherantidepressants, such as venlafaxine, mirtazapine, selegiline, and bupropion., such as venlafaxine, mirtazapine, selegiline, and bupropion.
Treatment of mental symptoms can help lessen problems with movement, improve quality of life, and sometimes delay the need for institutional care.
Caregiver and end-of-life issues
Because Parkinson disease is progressive, people eventually need help with normal daily activities, such as eating, bathing, dressing, and toileting. Caregivers can benefit from learning about the physical and psychological effects of Parkinson disease and about ways to enable people to function as well as possible. Because such care is tiring and stressful, caregivers may benefit from support groups.
Eventually, most people with Parkinson disease become severely disabled and immobile. They may be unable to eat, even with assistance. Dementia develops in about one-third of people with Parkinson disease. Because swallowing becomes increasingly difficult, death due to aspiration pneumonia (a lung infection due to inhaling fluids from the mouth or stomach) is a risk. For some people, a nursing home may be the best place for care.
Before people with Parkinson disease become incapacitated, they should establish advance directives, indicating what kind of medical care they want at the end of life.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Drug Information for the Topic





