


In Bartter syndrome and Gitelman syndrome, a hereditary defect of the kidney tubules causes the kidneys to excrete excessive amounts of electrolytes (potassium, sodium, and chloride), resulting in growth, electrolyte, and sometimes nerve and muscle abnormalities.


These syndromes are caused by defective genes.
Symptoms include excessive urine production, mild dehydration, and low blood pressure.
Diagnosis is made by measuring electrolyte levels in the blood and urine and possibly by genetic testing.
All people are given supplements of sodium, potassium, and magnesium, and people who have Bartter syndrome are also given nonsteroidal anti-inflammatory drugs (NSAIDs).
(See also Introduction to Congenital Kidney Tubular Disorders.)

Bartter syndrome and Gitelman syndrome are hereditary and are usually caused by a recessive gene (see figure Non–X-Linked Recessive Disorders). Thus, a person with Bartter syndrome or Gitelman syndrome has usually inherited 2 recessive genes for the disorder, 1 from each parent. Because 2 genes are needed when a recessive gene is involved, the parents are carriers of the gene but do not have the syndrome. However, siblings of children with the disorder might have it. Although both are rare, Gitelman syndrome is more common than Bartter syndrome.
In Bartter syndrome and Gitelman syndrome, the kidneys cannot reabsorb salt (sodium chloride) normally from the kidney tubule. Thus, the kidneys excrete excessive amounts of the electrolytes sodium and chloride in the urine. The loss of sodium and chloride leads to excessive urine production and thus mild dehydration.
Mild dehydration causes the body to produce more of the enzyme renin and the hormone aldosterone, which help regulate blood pressure. The increase in aldosterone increases potassium and acid secretion in the kidneys, leading to low blood potassium (hypokalemia) and loss of acids in the blood that causes blood pH to be alkaline (a disorder called metabolic alkalosis). Although the tubules are affected in both syndromes, the kidneys are otherwise unaffected and filter out waste products normally.
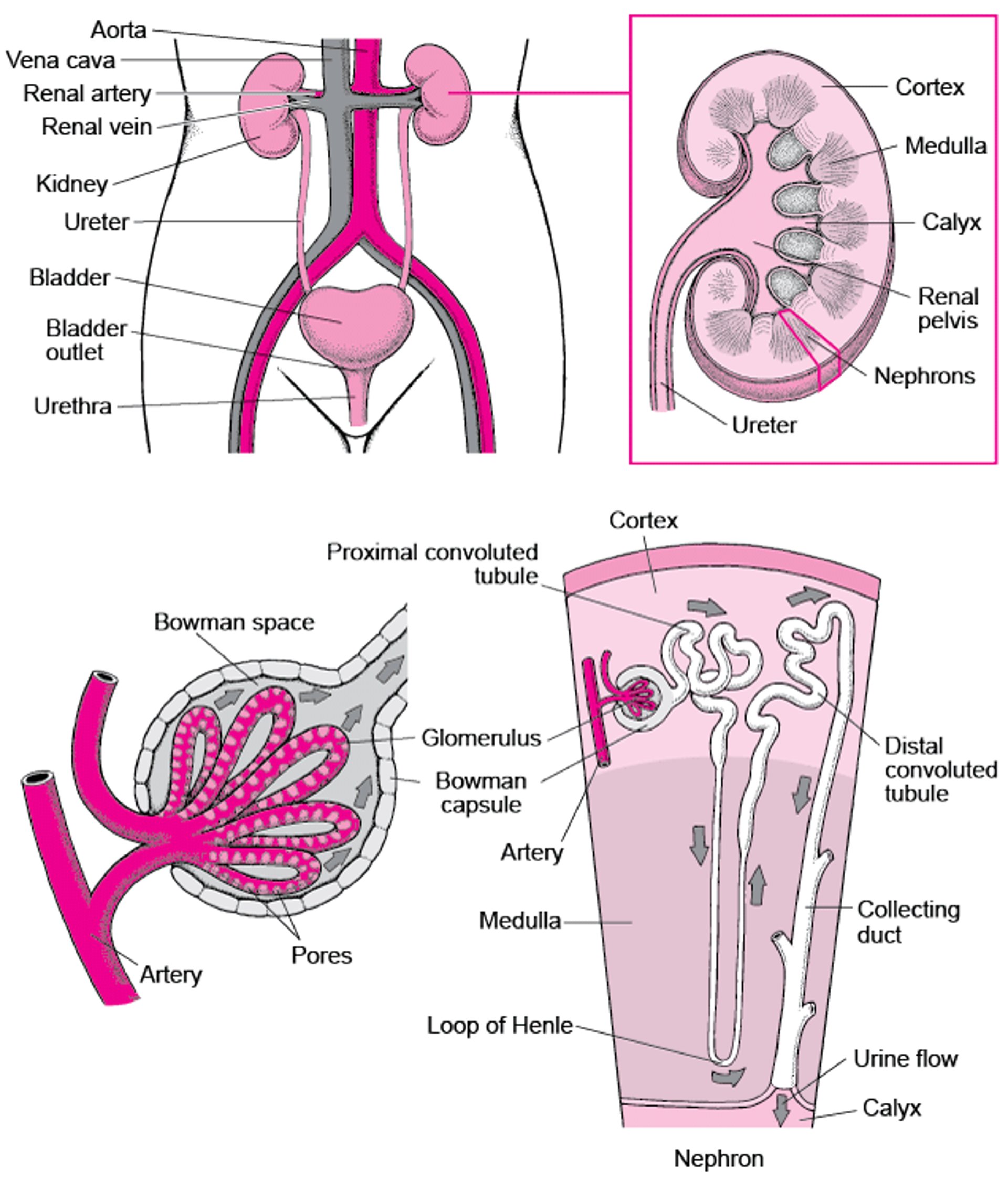
Viewing the Urinary Tract

The main differences between the 2 syndromes are
The genes that are involved
The part of the tubule that is affected
The age at which symptoms begin
Symptoms of Bartter Syndrome and Gitelman Syndrome
Symptoms of Bartter syndrome may appear before birth or during infancy or early childhood.
Symptoms of Gitelman syndrome may appear from late childhood to adulthood.
However, some people, particularly those who have Gitelman syndrome, have no symptoms and are diagnosed only after blood tests are done for other reasons.
Children with these syndromes have symptoms that are similar to those of people who take medications called diuretics, which increase urine output and can cause chemical imbalances in the blood. However, unlike in people taking diuretics, in people with Bartter syndrome or Gitelman syndrome, symptoms cannot be stopped by stopping a medication.
Fetuses with Bartter syndrome may grow poorly while in the womb. Some children are born prematurely and may be intellectually disabled.
Children with Bartter syndrome and sometimes those with Gitelman syndrome may have poor growth and developmental delays. The loss of magnesium, calcium, or potassium can lead to muscle weakness, cramping, spasms, or fatigue, particularly in people with Gitelman syndrome. Children with either syndrome may have excessive thirst, may produce large amounts of urine, may crave salt, and may have nausea and vomiting.
The loss of sodium and chloride leads to chronic mild dehydration. People with Bartter syndrome or Gitelman syndrome may have low blood pressure (hypotension).

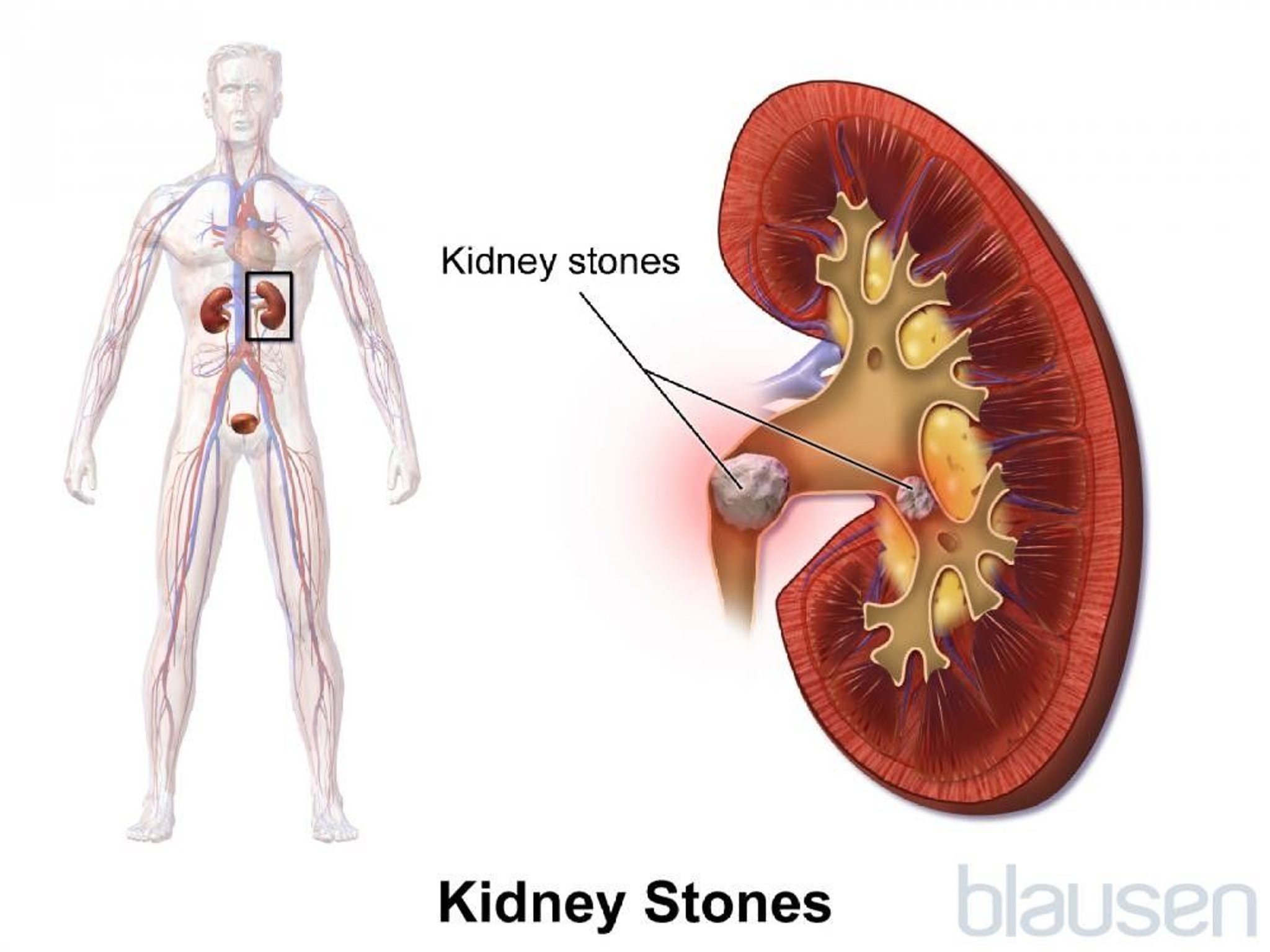
In addition, people with Bartter syndrome may develop kidney stones or a build up of calcium in the kidneys (called nephrocalcinosis) because they have large amounts of calcium in their urine. However, people with Gitelman syndrome do not develop these problems.
Diagnosis of Bartter Syndrome and Gitelman Syndrome
Measurement of electrolyte levels in the blood and urine
Genetic testing
Doctors suspect Bartter syndrome or Gitelman syndrome in children who have characteristic symptoms or who have abnormal levels of electrolytes in their blood and urine. Sometimes the abnormal electrolyte levels are found when laboratory tests are done for other reasons.

The diagnosis of either syndrome can be suggested by finding high levels of renin and aldosterone in the blood and high levels of sodium, chloride, and potassium in the urine.
The diagnosis is confirmed through genetic testing, which is becoming more widely available.
Family members can be evaluated by a genetic specialist or kidney specialist. Most often, genetic testing is done.
Treatment of Bartter Syndrome and Gitelman Syndrome
Supplements of sodium, potassium, and magnesium
For Bartter syndrome, nonsteroidal anti-inflammatory drugs
Because the defective functions of the tubule cells in the kidneys cannot be corrected, treatment is lifelong and is aimed at correcting the hormonal, fluid, and electrolyte abnormalities. People take supplements containing the substances that are lost in the urine, such as sodium, potassium, and magnesium, and also increase their fluid intake.
Certain medications can be helpful. People with Bartter syndrome are given nonsteroidal anti-inflammatory drugs (NSAIDs), such as indomethacin or ibuprofen. NSAIDs are not helpful in Gitelman syndrome. Certain medications can be helpful. People with Bartter syndrome are given nonsteroidal anti-inflammatory drugs (NSAIDs), such as indomethacin or ibuprofen. NSAIDs are not helpful in Gitelman syndrome.
Doctors may give growth hormone to children who are very short.







