

Chronic pancreatitis is long-standing inflammation of the pancreas that results in irreversible deterioration of the structure and function of the pancreas.
Heavy alcohol use and cigarette smoking are 2 major causes of chronic pancreatitis.
Abdominal pain may be persistent or come and go.
The diagnosis is based on the symptoms, a history of recurring acute pancreatitis and alcohol use, imaging tests, and pancreatic function tests.
Treatment involves avoiding alcohol and cigarettes, modifying the diet, taking pancreatic enzyme supplements, and measures to relieve the pain.
(See also Overview of Pancreatitis.)
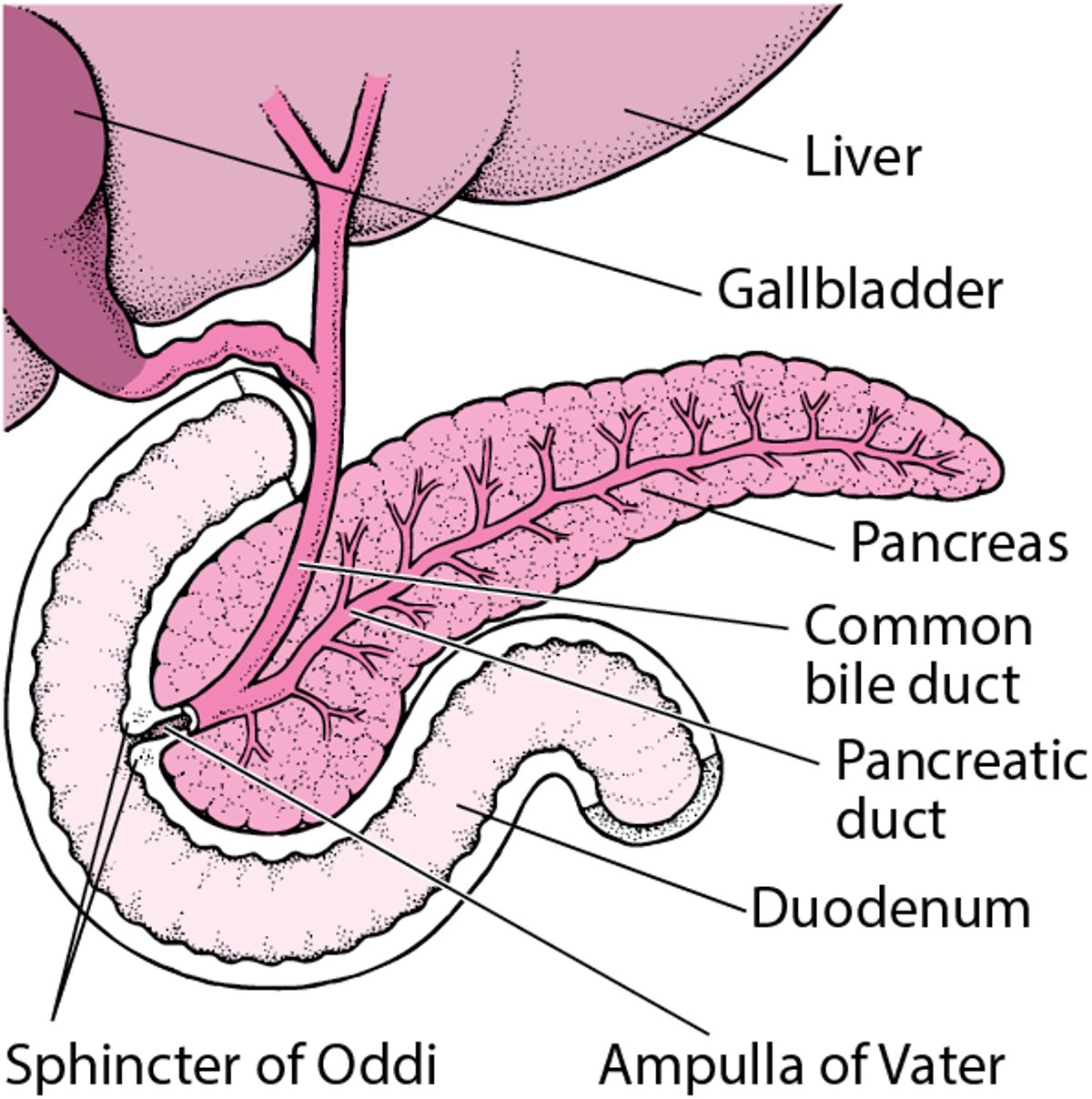
The pancreas is an organ in the upper abdomen that produces the hormone insulin and secretes pancreatic fluid through the pancreatic duct into the first part of the small intestine (duodenum). This pancreatic fluid contains digestive enzymes that help digest food.

In acute pancreatitis, inflammation develops quickly and subsides within a few days to a few weeks.
In chronic pancreatitis, inflammation is progressive and long-standing, which causes permanent damage and scarring (fibrosis) to the pancreas. This fibrosis is the hallmark of chronic pancreatitis. As chronic pancreatitis progresses, cells that secrete the digestive enzymes in the pancreatic fluid are slowly destroyed over time.
Locating the Pancreas

Causes of Chronic Pancreatitis
In the United States, about half of the cases of chronic pancreatitis are due to heavy alcohol consumption. People who smoke cigarettes also are at increased risk of developing chronic pancreatitis.
Less common causes of chronic pancreatitis include genetic disorders, such as cystic fibrosis, hereditary pancreatitis, or autoimmune pancreatitis. Rarely, an attack of severe acute pancreatitis causes permanent scarring (fibrosis) of the pancreas that leads to chronic pancreatitis. In some people, chronic pancreatitis develops when the pancreatic duct is blocked (obstructed) by stones or a tumor.
Some cases of chronic pancreatitis have no clear cause (are idiopathic). In tropical countries (for example, India, Indonesia, and Nigeria), chronic pancreatitis of unknown cause occurs among children and young adults (called tropical pancreatitis).
Symptoms of Chronic Pancreatitis
Abdominal pain is the main symptom of chronic pancreatitis. The upper abdominal pain may vary in intensity, and flare-ups (bouts or attacks) may last for many hours or several days. Later on in the illness, pain tends to become constant. The pain is usually worse after meals and may be lessened by sitting upright or leaning forward.
As chronic pancreatitis progresses and the cells that secrete the digestive enzymes are destroyed, the abdominal pain may stop.
Pancreatic insufficiency is the other main symptom of chronic pancreatitis. Pancreatic insufficiency is a decrease in the amount of digestive enzymes in pancreatic fluid. As the amount of digestive enzymes decreases, food is inadequately broken down. Food that is inadequately broken down is not absorbed properly (malabsorption), and the person may produce bulky, unusually foul-smelling, greasy stools (steatorrhea). The stool is light-colored and may even contain oil droplets. The inadequate absorption of food also leads to undernutrition, vitamin deficiencies, and weight loss.
Complications of chronic pancreatitis
A fluid collection called a pancreatic pseudocyst can develop. Pseudocysts can bleed or rupture, and ones that expand may cause pain or block the duodenum or bile ducts.
Eventually, the cells of the pancreas that secrete insulin may be destroyed, gradually leading to diabetes.
Patients with chronic pancreatitis are at increased risk of pancreatic cancer.
Diagnosis of Chronic Pancreatitis
Imaging tests
Pancreatic function tests
Sometimes blood tests
A doctor suspects chronic pancreatitis because of a person’s symptoms and history of acute pancreatitis flare-ups or heavy alcohol use. Doctors use the results of imaging tests and pancreatic function tests to make the diagnosis.
Did You Know...
|
Imaging tests
X-rays of the abdomen may be done to look for calcium deposits in the pancreas, which are present in some people with chronic pancreatitis.
Computed tomography (CT) of the abdomen may be done to show changes of chronic pancreatitis and to look for complications, such as a pseudocyst.
Many doctors now do a special magnetic resonance imaging (MRI) test called magnetic resonance cholangiopancreatography (MRCP). MRCP shows the bile and pancreatic ducts more clearly than does CT.
Endoscopic retrograde cholangiopancreatography (ERCP) allows doctors to view the bile duct and pancreatic duct. This test is rarely used for the diagnosis of chronic pancreatitis, but doctors may do it if a certain treatment for the pancreatic duct is needed, such as placing a tube (stent) through a blockage or removing a stone in the duct.
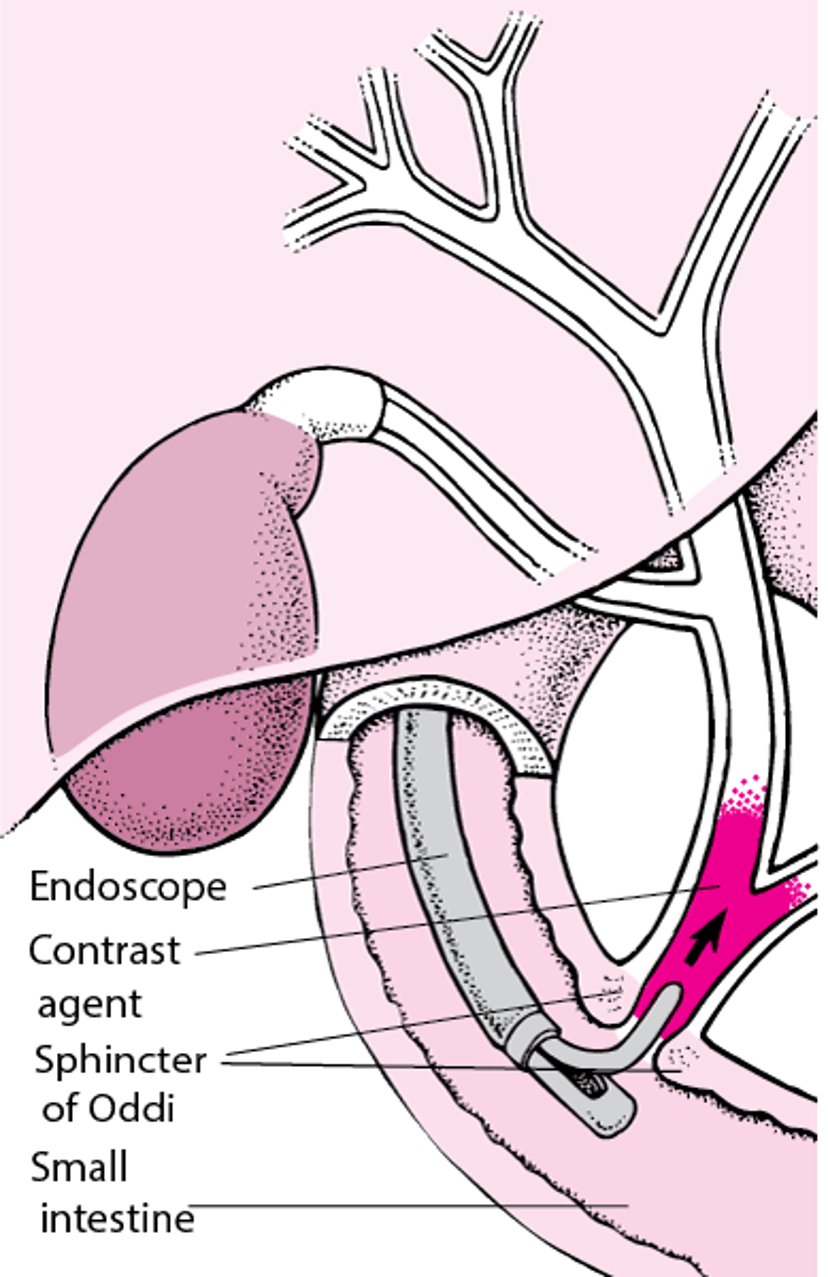
Understanding Endoscopic Retrograde Cholangiopancreatography (ERCP)
In endoscopic retrograde cholangiopancreatography (ERCP), a radiopaque contrast agent is introduced through an endoscope (a flexible viewing tube), which is inserted into the mouth and through the stomach into the duodenum (the first segment of the small intestine). The contrast agent is injected into the biliary tract just past the sphincter of Oddi. The contrast agent then flows back up the biliary tract and often shows the pancreatic ducts. Surgical instruments can also be used with the endoscope, allowing a doctor to remove a stone in a bile duct or insert a tube (stent) to bypass a bile duct blocked by scarring or cancer. |

Endoscopic ultrasonography (passage of a flexible viewing tube with an ultrasound probe attached to it through the mouth into the stomach and the first segment of the small intestine) is another test that helps detect abnormalities in the pancreas and pancreatic duct.
Because people with chronic pancreatitis are at increased risk of pancreatic cancer, any worsening of symptoms or narrowing of the pancreatic duct makes doctors suspect cancer. In such cases, a doctor is likely to do blood tests, an MRI scan, a CT scan, and/or endoscopic ultrasonography.
Pancreatic function tests
For chronic pancreatitis, doctors may also do tests of the pancreas to see how it is functioning. These tests help doctors determine whether there is pancreatic insufficiency that can cause malabsorption. Stool may be checked for levels of fat or a digestive enzyme such as elastase. Low levels of elastase indicate pancreatic insufficiency.
Blood tests
Blood tests are less useful in diagnosing chronic pancreatitis than in diagnosing acute pancreatitis, but they may indicate elevated levels of amylase and lipase (2 enzymes produced by the pancreas). Also, blood tests can be used to check the level of sugar (glucose) in the blood, which may be elevated.
Treatment of Chronic Pancreatitis
Pain control
Pancreatic enzyme supplements
Management of diabetes
The prognosis for chronic pancreatitis varies.
Even if alcohol is not the cause, all people with chronic pancreatitis should avoid drinking alcohol and stop smoking.
Pain control
Pain control is the most challenging part of managing chronic pancreatitis, and treatments are focused on reducing pain and slowing disease progression. Eating 4 or 5 meals a day consisting of food low in fat may reduce secretion of pancreatic enzymes and reduce pain.
Opioid analgesics are sometimes needed to relieve the pain. Too often, pain relief measures do not relieve the pain, requiring increased amounts of opioids, which may put the person at risk of addiction. Doctors may recommend additional pain medications, such as tricyclic antidepressants, gabapentin, pregabalin, and selective serotonin reuptake inhibitors (SSRIs), and prescribe them either alone or in combination with opioids to manage chronic pain, but results vary. Taking medications to treat pain caused by chronic pancreatitis is often unsatisfactory.are sometimes needed to relieve the pain. Too often, pain relief measures do not relieve the pain, requiring increased amounts of opioids, which may put the person at risk of addiction. Doctors may recommend additional pain medications, such as tricyclic antidepressants, gabapentin, pregabalin, and selective serotonin reuptake inhibitors (SSRIs), and prescribe them either alone or in combination with opioids to manage chronic pain, but results vary. Taking medications to treat pain caused by chronic pancreatitis is often unsatisfactory.
Doctors may give corticosteroids to treat autoimmune pancreatitis.
Sometimes doctors may use an endoscope (a flexible viewing tube) to carry out treatment. Endoscopic treatment with endoscopic retrograde cholangiopancreatography (ERCP) may be used to drain a duct that is blocked by scarring (stricture), stones, or both. This procedure may provide pain relief.
Lithotripsy (a procedure that involves the use of shock waves to break up stones) may be used to treat stones that are large or stuck in the pancreatic duct.
Surgical treatment may be an option if the pancreatic ducts are dilated or if there is an inflammatory mass in one region of the pancreas. For instance, when the pancreatic duct is dilated, creating a bypass from the pancreas to the small intestine relieves the pain in about 70 to 80% of people. When the duct is not dilated, part of the pancreas may have to be removed. Removing part of the pancreas means that cells that produce insulin are removed as well, and diabetes may develop. Doctors reserve surgical treatment for people who have stopped using alcohol and who can manage any diabetes that develops.
Sometimes a pancreatic pseudocyst can cause pain as it expands and may have to be drained (decompressed) endoscopically or through the overlying skin.
Pancreatic enzyme supplements
Pancreatic enzyme supplementation may reduce chronic pain by reducing the secretion of pancreatic enzymes. Although enzyme therapy is often tried because it is safe and has few side effects, it may not provide substantial pain relief.
For people who have pancreatic insufficiency, taking tablets or capsules of pancreatic enzyme extracts with meals can make the stool less greasy and improve food absorption, but these problems are rarely eliminated. The supplements should be taken with meals. Doctors sometimes recommend people take a histamine-2 (H2) blocker or a proton pump inhibitor (medications that reduce or prevent the production of stomach acid) with the pancreatic enzyme supplements. With pancreatic enzyme treatment, the person usually gains some weight, has fewer daily bowel movements, has no more oil droplets in the stool, and generally feels better. If these measures are ineffective, the person can try further decreasing fat intake. Supplements of the fat-soluble vitamins (A, D, E, and K) also may be needed.
Management of diabetes
(See also treatment of diabetes.)
Hypoglycemic medications taken by mouth rarely help treat diabetes caused by chronic pancreatitis. Insulin is generally needed but can cause a problem, because affected people also have decreased levels of Hypoglycemic medications taken by mouth rarely help treat diabetes caused by chronic pancreatitis. Insulin is generally needed but can cause a problem, because affected people also have decreased levels ofglucagon, which is a hormone that acts to balance the effects of insulin. An excess of insulin in the bloodstream causes low glucose (sugar) levels in the blood, which can result in a hypoglycemic coma (see symptoms of hypoglycemia).
Drugs Mentioned In This Article





