



- Anal Cancer
- Colorectal Cancer
- Colorectal Cancer Screening
- Esophageal Cancer
- Esophageal Tumors That Are Noncancerous
- Familial Adenomatous Polyposis
- Gastrointestinal Stromal Tumors
- Pancreatic Cancer
- Polyps of the Colon and Rectum
- Small-Intestine Cancer
- Small-Intestine Tumors That Are Noncancerous
- Stomach Cancer
- Stomach Tumors That Are Noncancerous
")




Family history and some dietary factors (low fiber, high fat) increase a person’s risk of colorectal cancer.
Typical symptoms include bleeding during a bowel movement, fatigue, and weakness.
Screening tests are important for people over age 45.
Colonoscopy is often used to make the diagnosis.
Surgery is usually done to remove the cancer.
Cancer that is caught early is most curable.
Screening, lifestyle changes, and possibly low-dose aspirin may decrease the risk of colorectal cancer.
Almost all cancers of the large intestine and rectum (colorectal) are adenocarcinomas, which develop from the lining of the large intestine (colon) and rectum.
Colorectal cancer usually begins as a polyp, which is a buttonlike growth on the surface of the intestinal or rectal lining. As the cancer grows, it begins to invade the wall of the intestine or rectum. Nearby lymph nodes also may be invaded. Because blood from the wall of the intestine and much of the rectum is carried to the liver, colorectal cancer can spread (metastasize) to the liver after spreading to nearby lymph nodes.
In Western countries, cancer of the large intestine and rectum is one of the most common types of cancer and the second leading cause of cancer death. The incidence of colorectal cancer begins to rise sharply around age 40 to 50. In 2024, an estimated 106,590 new cases of colon cancer and 46,220 new cases of rectal cancer were diagnosed. The number of deaths due to colorectal cancer has steadily decreased in the last several decades. This decrease is believed to be the result of improved screening and thus diagnosis at earlier stages of disease.
Colorectal cancer is slightly more common among men than women. About 5% of people with colon cancer or rectal cancer have cancer in 2 or more sites in the colon and rectum that do not seem to simply have spread from one site to another.
Risk Factors for Colorectal Cancer
People with a family history of colorectal cancer have a higher risk of developing the cancer themselves. Several hereditary disorders are risk factors for colorectal cancer:
Juvenile polyposis syndrome
People with ulcerative colitis or Crohn disease of the colon are at greater risk as well. This risk is related to the length of time the person has had the disease and the amount of colon that is affected.
People at highest risk tend to consume a diet that is high in fat, animal protein, and refined carbohydrates and low in fiber.
Lynch syndrome (hereditary nonpolyposis colorectal carcinoma [HNPCC])
Lynch syndrome comes from an inherited gene mutation. People with Lynch syndrome have a 70 to 80% lifetime risk of developing colorectal cancer, often before age 50. They are also at increased risk of other types of cancer, particularly endometrial cancer and ovarian cancer, but also stomach cancer and cancer of the small intestine, brain, pancreas, gallbladder, bile ducts, and urinary tract.
MUTYH polyposis syndrome
MUTYH polyposis syndrome is a rare genetic disorder that is an uncommon cause of colorectal cancer. It is due to genetic mutations of the MUTYH gene. More than half of the people who have this syndrome develop colorectal cancer starting in their 60s. They are also at increased risk of developing other types of cancer, such as other digestive tract cancers, bone cancers, and also cancer of the ovaries, bladder, thyroid, and skin.
Symptoms of Colorectal Cancer
Colorectal cancer grows slowly and does not cause symptoms for a long time. Symptoms depend on the type, location, and extent of the cancer and on complications.
Fatigue and weakness resulting from occult bleeding (bleeding not visible to the naked eye) may be the person’s only symptoms.
A tumor in the left (descending) colon is likely to cause obstruction at an earlier stage, because the left colon has a smaller diameter and the stool is semisolid. The person may seek medical treatment because of crampy abdominal pain or severe abdominal pain and constipation.
A tumor in the right (ascending) colon does not cause obstruction until later in the course of the cancer, because the ascending colon has a large diameter and the contents flowing through it are liquid. By the time the tumor is discovered, therefore, it may be larger than a tumor in the left.
Most colon cancers bleed, usually slowly. The stool may be streaked or mixed with blood, but often the blood cannot be seen.
The most common first symptom of rectal cancer is bleeding during a bowel movement. Whenever the rectum bleeds, even if the person is known to have hemorrhoids or diverticular disease, doctors must consider cancer as a possible diagnosis. Painful bowel movements and a feeling that the rectum has not been completely emptied are other symptoms of rectal cancer. Sitting may be painful, but otherwise the person usually feels no pain from the cancer itself unless it spreads to tissue outside the rectum.
Diagnosis of Colorectal Cancer
Colonoscopy
CT scan if cancer is found
Genetic testing for Lynch syndrome
People who have symptoms that suggest colon cancer or who have a positive screening test need a diagnostic test to confirm whether they do or do not have cancer.
People with blood in their stool require colonoscopy, as do those with abnormalities seen during a sigmoidoscopy or an imaging study. Any growths or abnormalities seen should be completely removed during the colonoscopy.

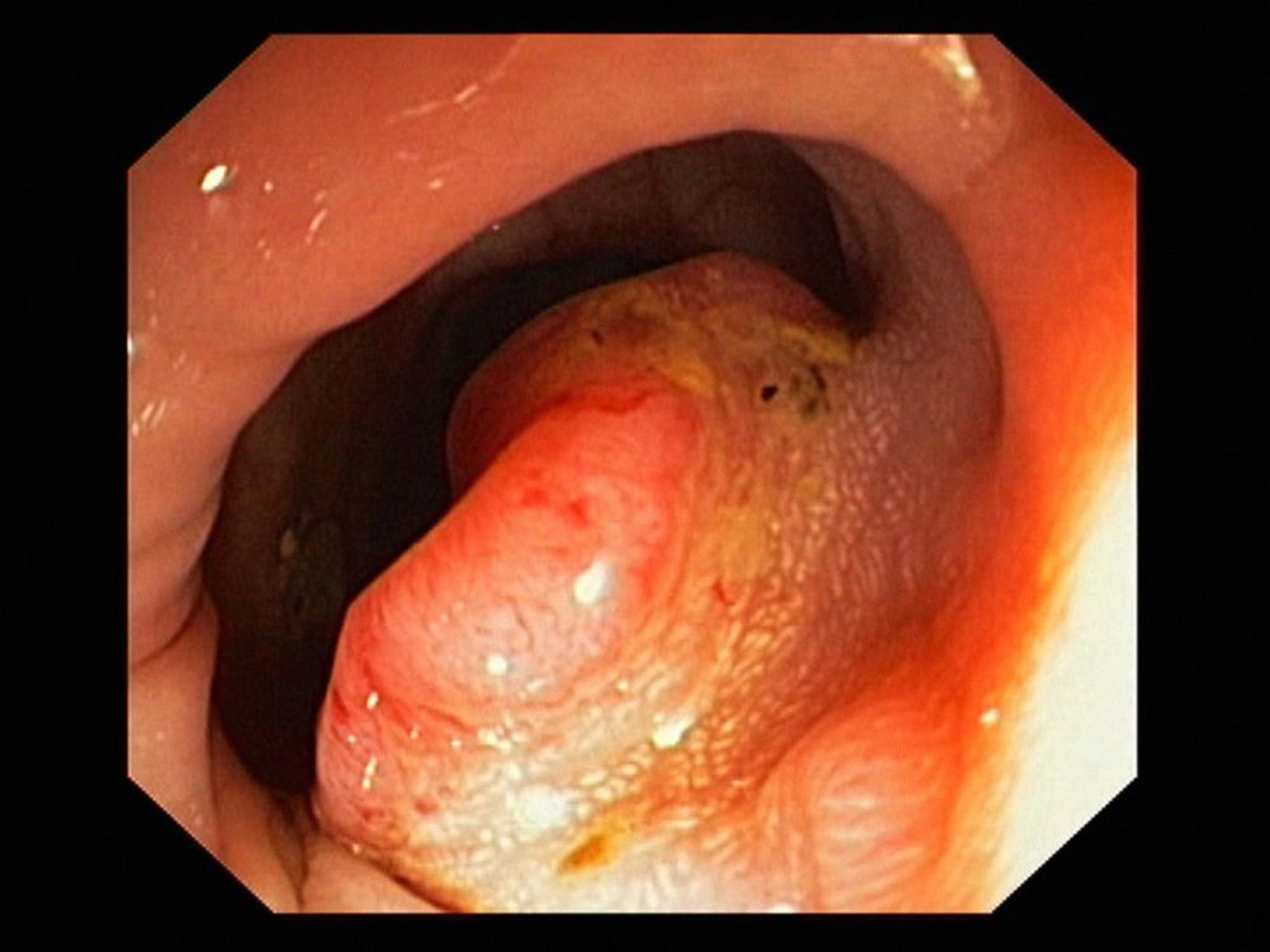
GASTROLAB/SCIENCE PHOTO LIBRARY
Barium enema x-rays may be taken to detect tumors in the lower part of the large intestine. However, colonoscopy is the preferred diagnostic test because during colonoscopy doctors can take tissue samples to see whether a growth is cancerous or not.
Once cancer is diagnosed, doctors usually do a CT scan of the chest, abdomen, and pelvis and do routine laboratory tests to look for cancer that has spread, to detect a low blood count (anemia), and to evaluate the person’s overall condition. Doctors typically also refer the person to a health care professional who specializes in treating colorectal cancer (for example, a colorectal surgeon or surgical oncologist).
Blood tests are not used to diagnose colorectal cancer, but they can help the doctor monitor the effectiveness of treatment after a tumor has been removed. For example, if levels of the cancer marker carcinoembryonic antigen (CEA) are high before surgery to remove a known cancer but are low after surgery, monitoring for another increase in the CEA level after surgery may help detect an early recurrence of the cancer.

Colon cancers that were removed during surgery are now routinely tested for the gene mutations that cause Lynch syndrome. People with relatives who developed colon, ovarian, or endometrial cancer at a young age or who have multiple relatives with those cancers should be tested for Lynch syndrome.
Diagnosis of MUTYH polyposis syndrome is established by genetic testing.
Treatment of Colorectal Cancer
Surgery
Sometimes chemotherapy, radiation therapy, or both
In most cases of colon cancer, the cancerous segment of the intestine and any nearby lymph nodes are removed surgically, and the remaining ends of the intestine are joined. If the cancer has penetrated the wall of the large intestine and spread to a very limited number of nearby lymph nodes, chemotherapy after surgical removal of all visible cancer may lengthen survival time, although the effects of these treatments are often modest.
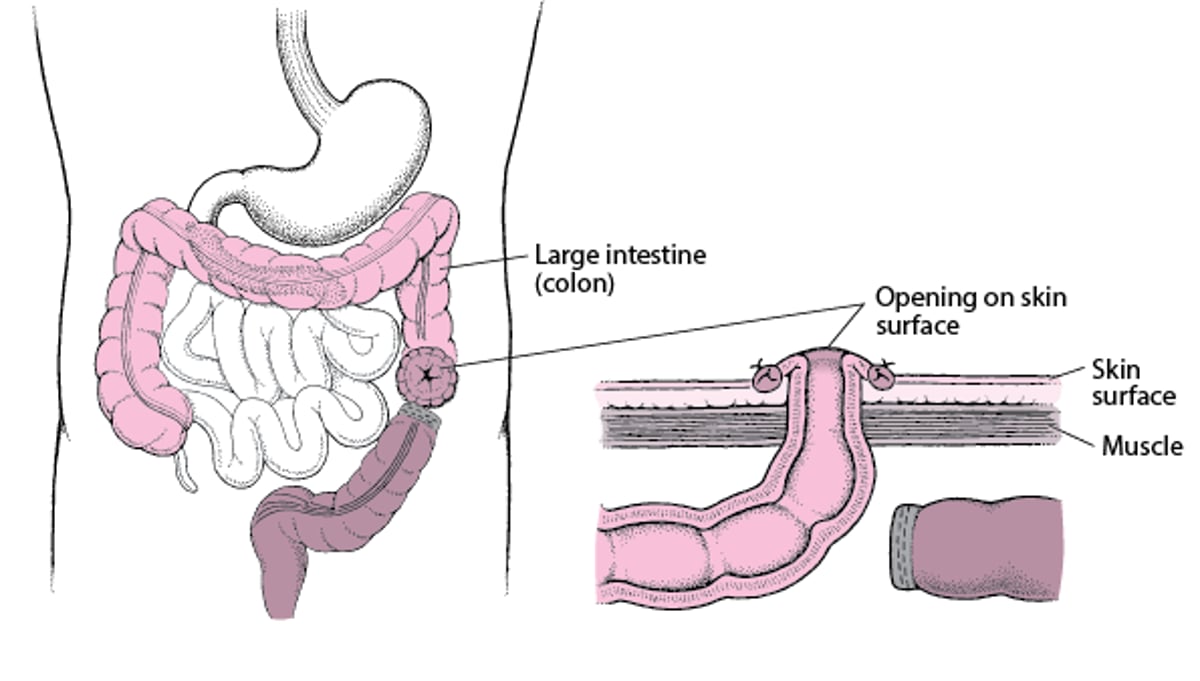
For rectal cancer, the type of operation depends on how far the cancer is located from the anus and how deeply it has grown into the rectal wall. The complete removal of the rectum and anus means the person needs a permanent colostomy. A colostomy is a surgically created opening between the large intestine and the abdominal wall. The contents of the large intestine empty through the abdominal wall into a colostomy bag. If doctors can leave part of the rectum and the anus is intact, the colostomy may be temporary. After these tissues have had time to heal (over several months), another surgery can be done to rejoin the rectal stump to the end of the large intestine, and the colostomy can be closed.
Understanding Colostomy
In a colostomy, the large intestine (colon) is cut. The healthy end of the large intestine, which is before the blockage, is brought to the skin surface through a surgically created opening in the abdominal wall. It is then stitched to the skin of the opening. Stool passes through the opening and into a disposable bag. The colostomy allows the remaining part of the large intestine to rest while the person recovers. After the person recovers from the surgery and the colon heals, the 2 ends can be reattached so that stool can pass normally. |

When rectal cancer has penetrated the rectal wall and spread to a very limited number of nearby lymph nodes, giving chemotherapy plus radiation therapy (see Combination Cancer Therapy) before or after surgical removal of all visible cancer may lengthen survival time.
When cancer has spread to lymph nodes far from the colon or rectum, to the lining of the abdominal cavity, or to other organs, the cancer cannot be cured by surgery alone. However, surgery is sometimes done to relieve any intestinal obstruction and ease symptoms. Chemotherapy with a single medication or combination of medications may shrink the cancer and prolong life for several months. The doctor usually discusses end-of-life care with the person, the family, and other health care professionals (see Treatment Options at the End of Life).
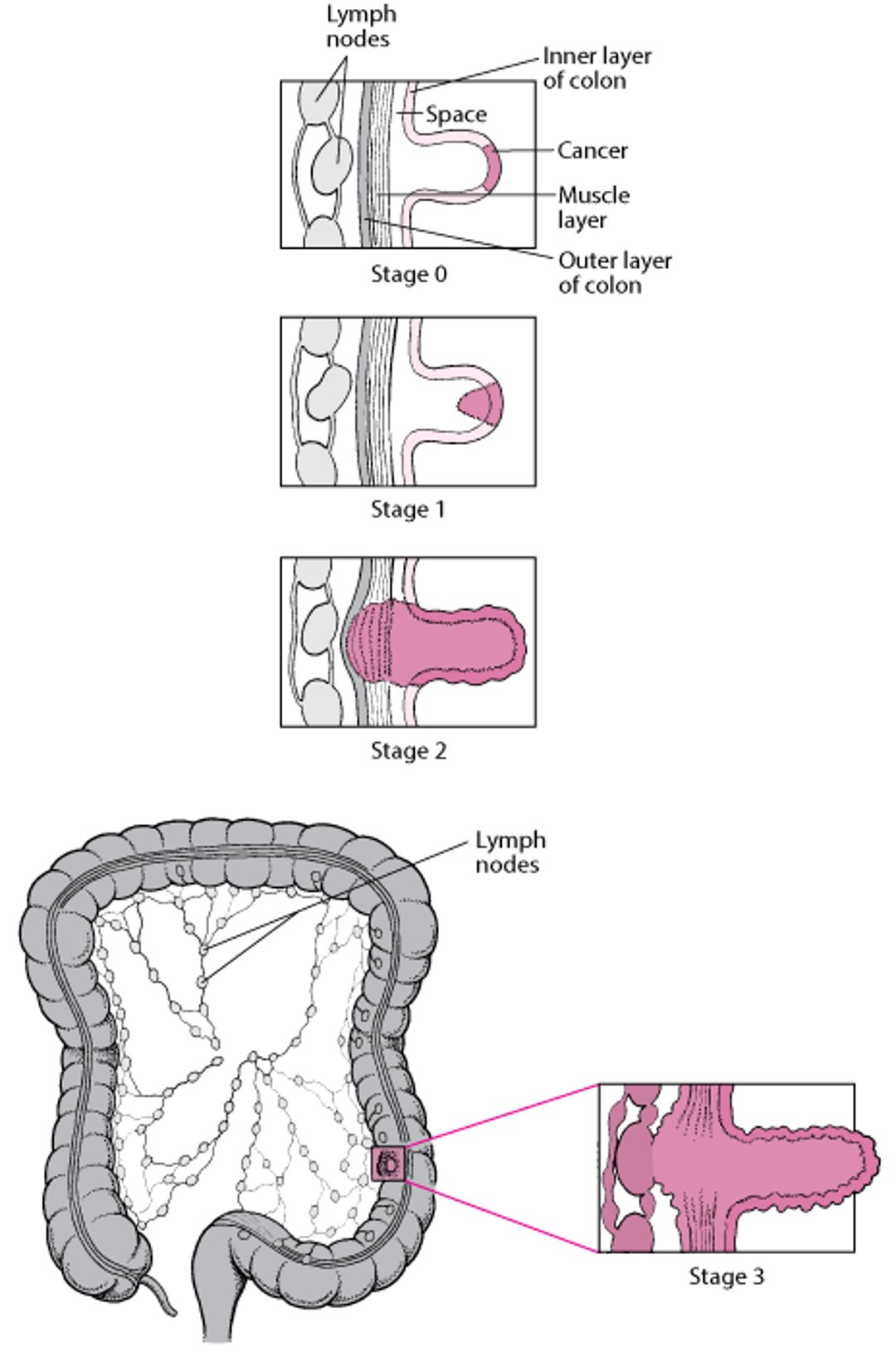
Staging Colon Cancer
|

When the cancer has spread (metastasized) only to the liver, doctors sometimes remove tumors surgically. Alternatively, doctors may inject chemotherapy agents or radioactive beads directly into the artery supplying the liver with blood. A small pump inserted surgically beneath the skin or an external pump worn on a belt allows the person to be mobile during the treatment. This treatment may provide more benefit than ordinary chemotherapy, but more research is needed. Radiofrequency ablation, which uses high-frequency alternating electric current (AC current) to heat and destroy tissue, is an alternative therapy for selected people who have liver tumors. Also, radiation therapy focused on the tumors can be used for palliation (to help relieve symptoms without necessarily aiming for a cure).
If the cancer is obstructing the colon in a person who cannot tolerate surgery because of poor health, doctors may try to relieve symptoms in other ways. One treatment involves shrinking the tumor with a probe that applies an electric current (electrocautery) or sometimes with a laser. Alternatively, doctors may use an expandable wire mesh tube (stent) to hold open the obstructed area. All of these treatments can be done through a colonoscope. Although the person often feels better for a while, these treatments do not lengthen survival time.
After surgery
After surgery, colonoscopy should be done within 1 year. A second colonoscopy should be done 3 years after that if no polyps or tumors are found. Thereafter, colonoscopy should be done every 5 years.
Doctors also do a physical examination and blood tests such as a complete blood count, liver tests, and carcinoembryonic antigen level at regular intervals after surgery.
Imaging tests (CT or MRI) are done every 6 to 12 months for 5 years.
Prognosis for Colorectal Cancer
Colon cancer is most likely to be cured if it is removed early, before it has spread. Cancers that have grown deeply or through the wall of the colon have often spread, and sometimes these cancers cannot be detected.
The 5-year survival rate is about 90% when the cancer is only in the lining of the bowel wall, about 73 to 74% when the cancer extends through the bowel wall, and it is less than 20% when the cancer has metastasized to other organs.
Prevention of Colorectal Cancer
Screening
Modification of lifestyle habits
Sometimes low-dose aspirin
People may reduce their risk of developing colorectal cancer by getting screened.
Habits related to diet, weight, and exercise are linked to colorectal cancer risk. People may be able to reduce their risk by doing the following:
Increasing physical activity
Maintaining a healthy weight
Limiting alcohol consumption
Avoiding tobacco
Eating less red meat (such as beef, pork, and lamb) and processed meats (such as hot dogs and some lunch meats)
Eating more fiber (such as vegetables, fruits, and whole grains)
In addition to screening and lifestyle changes, doctors may recommend certain adults 50 to 59 years of age who have an increased risk of heart disease take a daily low dose of aspirin. In these adults, In addition to screening and lifestyle changes, doctors may recommend certain adults 50 to 59 years of age who have an increased risk of heart disease take a daily low dose of aspirin. In these adults,aspirin may prevent heart disease and colorectal cancer.
Drugs Mentioned In This Article






