



- Overview of Abnormal Heart Rhythms
- Medications to Treat Abnormal Heart Rhythms
- Artificial Pacemakers
- Cardioversion-Defibrillation
- Implantable Cardioverter-Defibrillator (ICD)
- Destroying Abnormal Heart Tissue (Ablation)
- Atrial Fibrillation and Atrial Flutter
- Atrial Premature Beats
- Cardiac Channelopathies
- Torsades de Pointes Ventricular Tachycardia
- Long QT Interval Syndromes
- Paroxysmal Supraventricular Tachycardia (SVT, PSVT)
- Sinus Node Dysfunction
- Ventricular Fibrillation
- Ventricular Premature Beats
- Ventricular Tachycardia
- Wolff-Parkinson-White (WPW) Syndrome
- Arrhythmogenic Cardiomyopathies
- Overview of Heart Block
- Atrioventricular Block
- Bundle Branch Block



")
A heart disorder is the most common cause of an abnormal heart rhythm.
Sometimes people are aware of abnormal heart rhythms, but many times they feel only their consequences, such as weakness or fainting.
The diagnosis is based on electrocardiography (ECG).
Treatment involves restoring the heart to a normal rhythm and preventing further episodes.
The heart is a muscular organ with 4 chambers designed to work efficiently, reliably, and continuously over a lifetime. The muscular walls of each chamber contract in a regulated sequence, pumping blood as required by the body while expending as little energy as possible during each heartbeat.
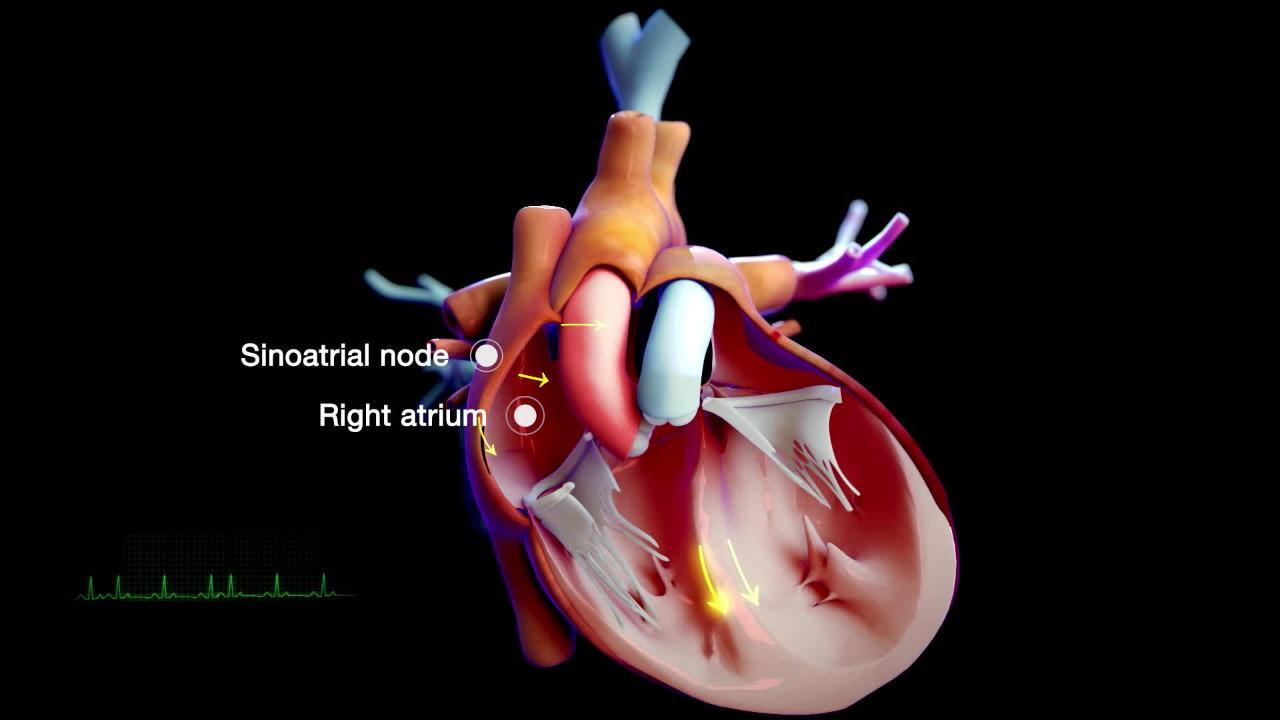
Contraction of the muscle fibers in the heart is controlled by electricity that flows through the heart in a precise manner along distinct pathways at a controlled speed. The electrical current that begins each heartbeat originates in the heart’s pacemaker (called the sinus node or sinoatrial node), located in the top of the upper right heart chamber (right atrium). The rate at which the pacemaker discharges the electrical current determines the heart rate. This rate is influenced by nerve impulses and by levels of certain hormones in the bloodstream.
The heart rate is regulated automatically by the autonomic nervous system, which consists of the sympathetic and parasympathetic divisions. The sympathetic division increases the heart rate through a network of nerves called the sympathetic plexus. The parasympathetic division decreases the heart rate through a single nerve, the vagus nerve.
Heart rate is also influenced by hormones released into the bloodstream by the sympathetic division:
Epinephrine (adrenaline)
Norepinephrine (noradrenaline)
Epinephrine and norepinephrine increase the heart rate. Thyroid hormone, which is released into the bloodstream by the thyroid gland, also increases the heart rate.
In an adult at rest, the normal heart rate is usually between 60 and 100 beats per minute. However, lower rates may be normal in young adults and those who are physically fit. A person’s heart rate varies normally in response to exercise and such stimuli as pain and anger. Heart rhythm is considered abnormal only when the heart rate is inappropriately fast (called tachycardia), slow (called bradycardia), or irregular or when electrical impulses travel along abnormal pathways.

Normal electrical pathway
The electrical current from the sinoatrial node flows first through the right atrium and then through the left atrium, causing the muscles of these chambers to contract and blood to be pumped from the atria into the lower heart chambers (ventricles). The electrical current then reaches the atrioventricular node, located in the lower part of the wall between the atria near the ventricles. The atrioventricular node provides the only electrical connection between the atria and ventricles. Otherwise, the atria are insulated from the ventricles by tissue that does not conduct electricity. The atrioventricular node delays transmission of the electrical current so that the atria can contract completely and the ventricles can fill with as much blood as possible before the ventricles are electrically signaled to contract.
Tracing the Heart’s Electrical Pathway
The sinoatrial (sinus) node (1) initiates an electrical impulse that flows through the right and left atria (2), making them contract. When the electrical impulse reaches the atrioventricular node (3), it is delayed slightly. The impulse then travels down the bundle of His (4), which divides into the right bundle branch for the right ventricle (5) and the left bundle branch for the left ventricle (5). The impulse then spreads through the ventricles, making them contract. |

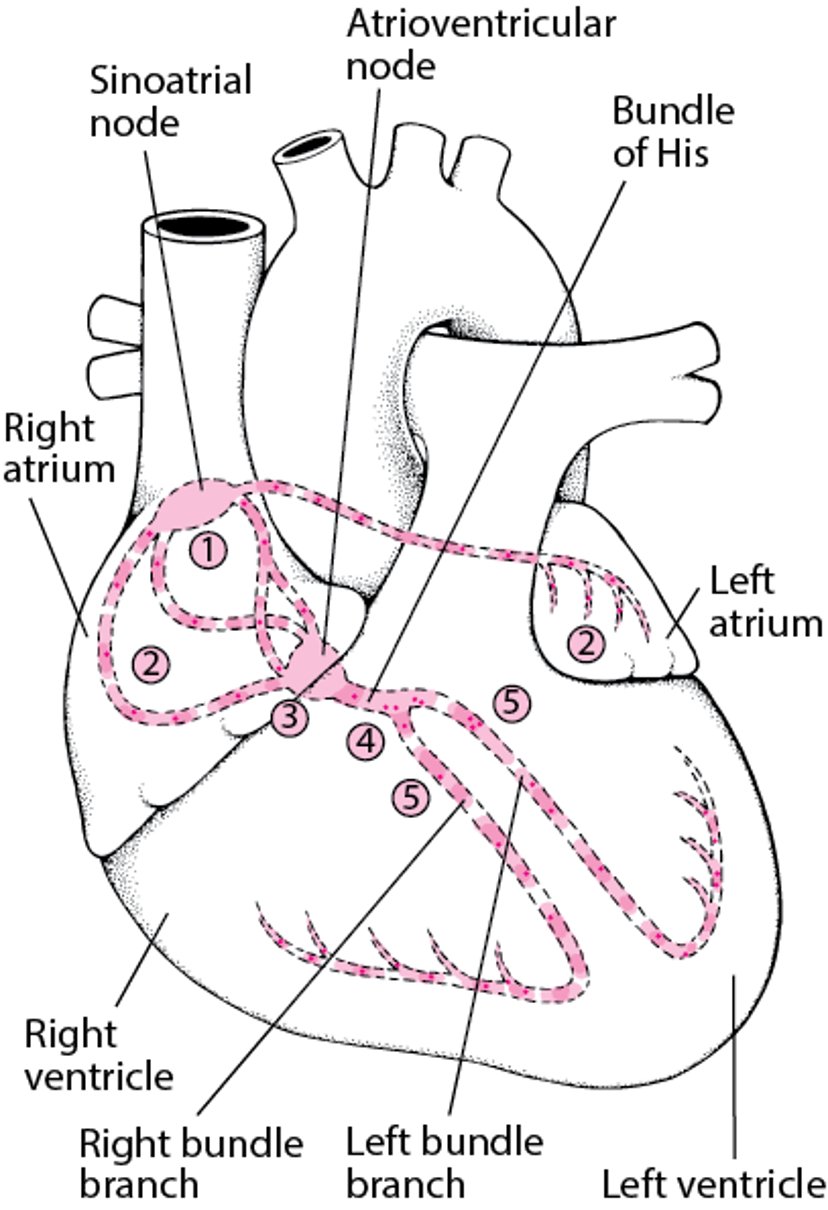
After passing through the atrioventricular node, the electrical current travels down the bundle of His, a group of fibers that divide into a left bundle branch for the left ventricle and a right bundle branch for the right ventricle. The electrical current then spreads in a regulated manner over the surface of the ventricles, from the bottom up, initiating contraction of the ventricles, which eject blood from the heart.
Causes of Abnormal Heart Rhythms
The most common cause of an abnormal heart rhythm (arrhythmia) is a heart disorder, particularly coronary artery disease, heart valve disorders, and heart failure. Many medications, prescription or nonprescription, including those used to treat heart disorders, can lead to arrhythmias. Some arrhythmias are caused by anatomic abnormalities present at birth (congenital birth defects). Age-related changes in the heart’s electrical system make some arrhythmias more likely.
Sometimes no cause for an arrhythmia can be identified.
Fast arrhythmias
Fast arrhythmias (tachyarrhythmias) may start on their own or be triggered by exercise, emotional stress, excessive alcohol consumption, smoking, or use of medications or drugs that contain stimulants, including cold and hay fever remedies.
An overactive thyroid gland (hyperthyroidism), producing high levels of thyroid hormone, may cause fast arrhythmias.
Slow arrhythmias
Slow arrhythmias (bradyarrhythmias) may be triggered by pain, hunger, fatigue, digestive disorders (such as diarrhea and vomiting), or swallowing, which can stimulate the vagus nerve excessively. With enough stimulation, which is rare, the vagus nerve can cause the heart to stop for a moment. In most of these circumstances, the arrhythmia tends to resolve on its own.
An underactive thyroid gland (hypothyroidism), producing low levels of thyroid hormone, may cause slow arrhythmias.
Symptoms of Abnormal Heart Rhythms
Some people who have an abnormal heart rhythm (arrhythmia) may be aware of it. However, awareness of heartbeats (called palpitations) varies widely among people. Some people can feel normal heartbeats, and most people can feel heartbeats when they lie on their left side.
Arrhythmias have consequences that range from harmless to life threatening. The seriousness of an arrhythmia may not be closely linked with the severity of the symptoms it causes. Some life-threatening arrhythmias cause no symptoms, and some otherwise inconsequential arrhythmias may cause severe symptoms. The nature and severity of the underlying heart disorder are often more important than the arrhythmia itself.
When arrhythmias impair the heart’s ability to pump blood, they can cause weakness, a reduced capacity for exercise, shortness of breath, light-headedness, dizziness, fainting (syncope), or death. Fainting occurs when the heart is pumping so inefficiently that it can no longer maintain adequate blood pressure. If such an arrhythmia persists, death may result. Arrhythmias may also aggravate the symptoms of an underlying heart disorder, including chest pain and shortness of breath. Arrhythmias that cause symptoms require prompt attention.
Did You Know...
|
Diagnosis of Abnormal Heart Rhythms
Electrocardiography
Often, a person’s description of symptoms can help doctors make a preliminary diagnosis and determine the severity of the abnormal heart rhythm (arrhythmia). The most important considerations are whether the palpitations are
Fast or slow
Regular or irregular
Brief or prolonged
Another important consideration is whether the arrhythmia causes symptoms.
Doctors also need to know whether the palpitations occur at rest or only during strenuous or unusual activity and whether they start and stop suddenly or gradually.
Certain diagnostic procedures are usually needed to determine the exact nature of the arrhythmia and its cause.
Electrocardiography (ECG or EKG) is the main diagnostic procedure for detecting arrhythmias and determining their cause. This procedure provides a graphic representation of the electrical current producing each heartbeat. Usually, ECG records the heart rhythm for only a very short time.
Because arrhythmias are often intermittent, a portable ECG monitor (called a Holter monitor or an event monitor) may be used to record heart rhythm continuously or when the wearer senses an abnormal heart rhythm and activates the monitor. These monitors may be worn for 24 or 48 hours or as long as 2 weeks, depending on the type of monitor and what disorders the doctor is looking for. All long-term monitors can record sporadic arrhythmias as the person engages in normal daily activities. During the recording period, the person also keeps a diary of symptoms and activities, so the doctor can see whether those symptoms are correlated with the arrhythmias.
To detect dangerous arrhythmias that occur very infrequently, doctors sometimes implant a recording device under the skin below the left collarbone (clavicle). The device can be left in place for long periods. It electronically transmits stored recordings of abnormal heart rhythms painlessly through the skin.
People with suspected life-threatening arrhythmias are usually hospitalized. Their heart rhythm is continuously recorded and displayed on a television-type monitor by the bedside or at the nursing station. Thus, any problems can be identified promptly.
Other diagnostic procedures include
Blood pressure measurement during exercise
Echocardiography to detect anatomic abnormalities
During electrophysiologic testing, catheters with tiny electrodes at their tip are inserted through a vein and threaded into the heart. The electrodes are used to stimulate the heart, and the heart’s response is monitored, so that the type of arrhythmia and the preferred treatment options can be determined.
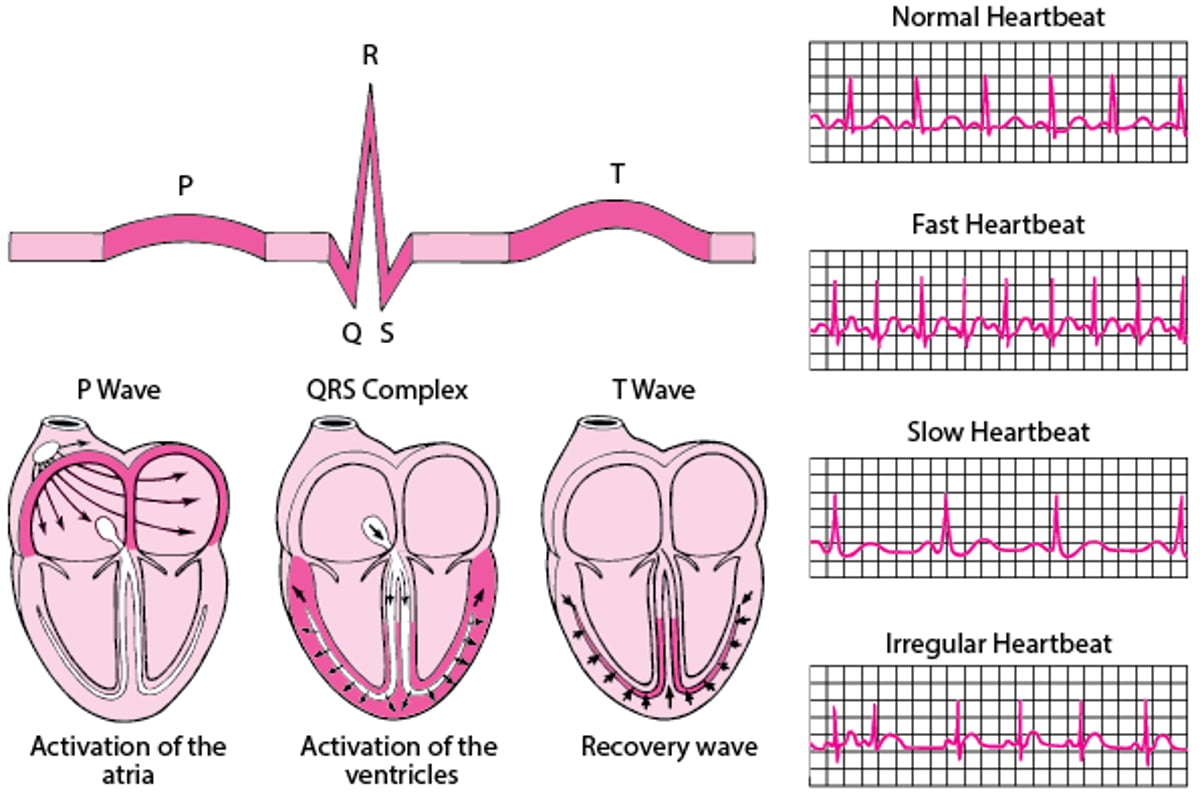
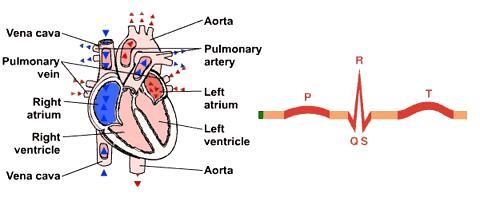
ECG: Reading the Waves
An electrocardiogram (ECG) represents the electrical current moving through the heart during a heartbeat. The current's movement is divided into parts, and each part is given an alphabetic designation in the ECG. Each heartbeat begins with an impulse from the heart's pacemaker (sinus or sinoatrial node). This impulse activates the upper chambers of the heart (atria). The P wave represents activation of the atria. Next, the electrical current flows down to the lower chambers of the heart (ventricles). The QRS complex represents activation of the ventricles. The electrical current then spreads back over the ventricles in the opposite direction. This activity is called the recovery wave, which is represented by the T wave. Many kinds of abnormalities can often be seen on an ECG. They include a previous heart attack (myocardial infarction), an abnormal heart rhythm (arrhythmia), an inadequate supply of blood and oxygen to the heart (ischemia), and excessive thickening (hypertrophy) of the heart's muscular walls. Certain abnormalities seen on an ECG can also suggest bulges (aneurysms) that develop in weak areas of the heart's walls. Aneurysms may result from a heart attack. If the rhythm is abnormal (too fast, too slow, or irregular), the ECG may also indicate where in the heart the abnormal rhythm starts. Such information helps doctors begin to determine the cause. |

Treatment of Abnormal Heart Rhythms
Antiarrhythmic medications, usually for a fast heart rate
An artificial pacemaker, usually for a slow heart rate
Delivering an electric shock, usually for a fast heart rate
Sometimes, destroying abnormal tissue responsible for the arrhythmia (ablation)
For people who have a harmless yet bothersome abnormal heart rhythm (arrhythmia), reassurance that the arrhythmia is harmless may be treatment enough. Sometimes arrhythmias occur less often or even stop when doctors change a person’s medications or adjust the dosages. Avoiding alcohol,caffeine (in beverages and foods), and smoking may also help. Avoiding strenuous exercise may help if palpitations occur only during exercise. Sometimes people need to stop driving until doctors can determine whether treatment is effective.
Antiarrhythmic medications are useful for suppressing fast arrhythmias that cause intolerable symptoms or pose a risk. No single medication suppresses all arrhythmias in all people. Sometimes several medications must be tried until the response is satisfactory. Sometimes antiarrhythmic medications can worsen or even cause arrhythmias. This effect is called proarrhythmia. Antiarrhythmic medications may also cause other side effects.
Artificial pacemakers are electronic devices that act in place of the heart’s own pacemaker, the sinoatrial node. These devices are implanted surgically under the skin, usually below the left or right collarbone. They are connected to the heart by wires (leads) running inside a vein. The tips of the wires are implanted in the wall of one or more heart chambers. The pacemaker sends an electrical signal that makes the heart muscle contract.
Electrical shocks to the heart (cardioversion and defibrillation) can sometimes stop a fast arrhythmia and restore normal rhythm. The shock briefly stops the heart from beating and, after a second or 2, the heart starts beating again on its own. Often, it starts back in a normal rhythm, but sometimes the arrhythmia starts again. Electrical shocks cannot restart a heart that has no electrical activity at all (asystole). Cardioversion and defibrillation are usually done using an external device, but people with dangerous arrhythmias may have a device, called an implantable cardioverter-defibrillator (ICD), permanently placed in their body.
Certain types of arrhythmias are due to a localized abnormal area in the heart’s electrical system. Destroying or removing that area (ablation) can sometimes eliminate the arrhythmia.
Prognosis for Abnormal Heart Rhythms
Most abnormal heart rhythms (arrhythmias) neither cause symptoms nor interfere with the heart’s ability to pump blood. Thus, they usually pose little or no risk, although they can cause considerable anxiety if a person becomes aware of them. However, some arrhythmias, harmless in themselves, can lead to more serious arrhythmias.
Any arrhythmia that impairs the heart’s ability to pump blood adequately is serious. How serious depends in part on whether the arrhythmia originates in the sinoatrial node, in the atria, in the atrioventricular node, or in the ventricles. Generally, arrhythmias that originate in the ventricles are more serious than those that originate in the atria, which are more serious than those that originate in the sinoatrial node or atrioventricular node. However, there are many exceptions.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: Arrhythmia: Information to help people understand their risks of arrhythmias as well as information on diagnosis and treatment






