



Shoulder dislocations occur when the ball-shaped head of the upper arm bone (humerus) pops out of its rounded socket in the shoulder blade (scapula).



When the shoulder is dislocated, it is usually forcefully pushed forward out of the joint.
The shoulder may look distorted and is usually very painful.
Often, doctors can diagnose a dislocated shoulder by examining it, but x-rays are taken to confirm it.
Doctors can usually put the joint back in place without surgery, often after people are given drugs to help them tolerate the procedure.
(See also Overview of Dislocations.)
The shoulder is the most commonly dislocated large joint. In over 95% of shoulder dislocations, the upper arm bone is pushed forward out of the joint (anterior dislocation). But occasionally, it is pushed backward or downward. Usually, a backward (posterior) dislocation occurs when a person has a seizure or receives an electric shock (for example, in a lightning injury). Downward dislocations are rare and usually obvious. Most people with a downward dislocation hold their arm over their head, typically with the forearm resting on the head.
The bone may be pushed all the way out of the joint—called a complete dislocation—or part way out—called a partial dislocation (subluxation).
The shoulder may be dislocated when strong force (such as a sudden blow) pulls, pushes, or twists the shoulder out, up, or back. Usually, the shoulder is pulled and rotated out. Common causes are sports injuries (such as blocking a shot while playing basketball), a car crash, and falls.
When a shoulder is dislocated, tissues around the joint, such as ligaments, tendons, blood vessels, and nerves, may also be stretched or torn. Sometimes a bone, usually the top of the arm bone, is broken, especially in people over 45.
If the injury was severe or if people, particularly those under 30, dislocate their shoulder several times (for example, by continuing to play sports), the shoulder may become unstable and more likely to be dislocated again.
Symptoms of a Dislocated Shoulder
The dislocated shoulder may be visibly out of place or look distorted. The area around the joint may be swollen or bruised. The pain is usually intense. People are unable or unwilling to move their arm away from their body. Shoulder dislocations may also make the muscle that covers the shoulder joint (the deltoid) feel numb.
The trauma of the dislocation may cause spasms in the shoulder muscles, often making the pain worse.
Diagnosis of a Dislocated Shoulder
Physical examination
X-rays
If people suspect that their shoulder is dislocated, they should see a doctor immediately. They should not try to move the shoulder back in place. Doing so can damage the area further. Until they can see a doctor, they should keep the arm as still as possible, possibly with a sling or splint, and apply ice. Ice may help relieve pain and reduce swelling.
Doctors ask people how the injury occurred, how severe the pain is, and whether they can move the arm. Doctors can often diagnose a dislocated shoulder by examining it. However, x-rays are usually taken to confirm the diagnosis and to exclude fractures. Doctors need to know whether any bones are fractured before they try to put the joint back into place.
Treatment of a Dislocated Shoulder
Maneuvers to put the joint back in place
A sling and swathe to immobilize the joint
Treatment of shoulder dislocations consists of putting the joint back in place (reduction). Before this maneuver, people are often given a sedative, strong pain-relievers, and/or an injection of anesthetic into the joint, but they remain conscious. Many techniques, such as the Davos or Hennepin technique, can be done without use of a sedative, but they require time (several minutes) for the affected muscles to relax enough that the shoulder can be reduced.
There are several ways to put the shoulder back in place. They include
Traction-countertraction: The person is held still while the practitioner pulls the affected arm down and out.
Putting a Shoulder Back in Place: Traction-Countertraction
The person lies down on an immobile surface. One practitioner pulls on a folded sheet wrapped around the person's chest to hold the person still as another practitioner pulls the affected arm down and out. The technique is called traction-countertraction. |

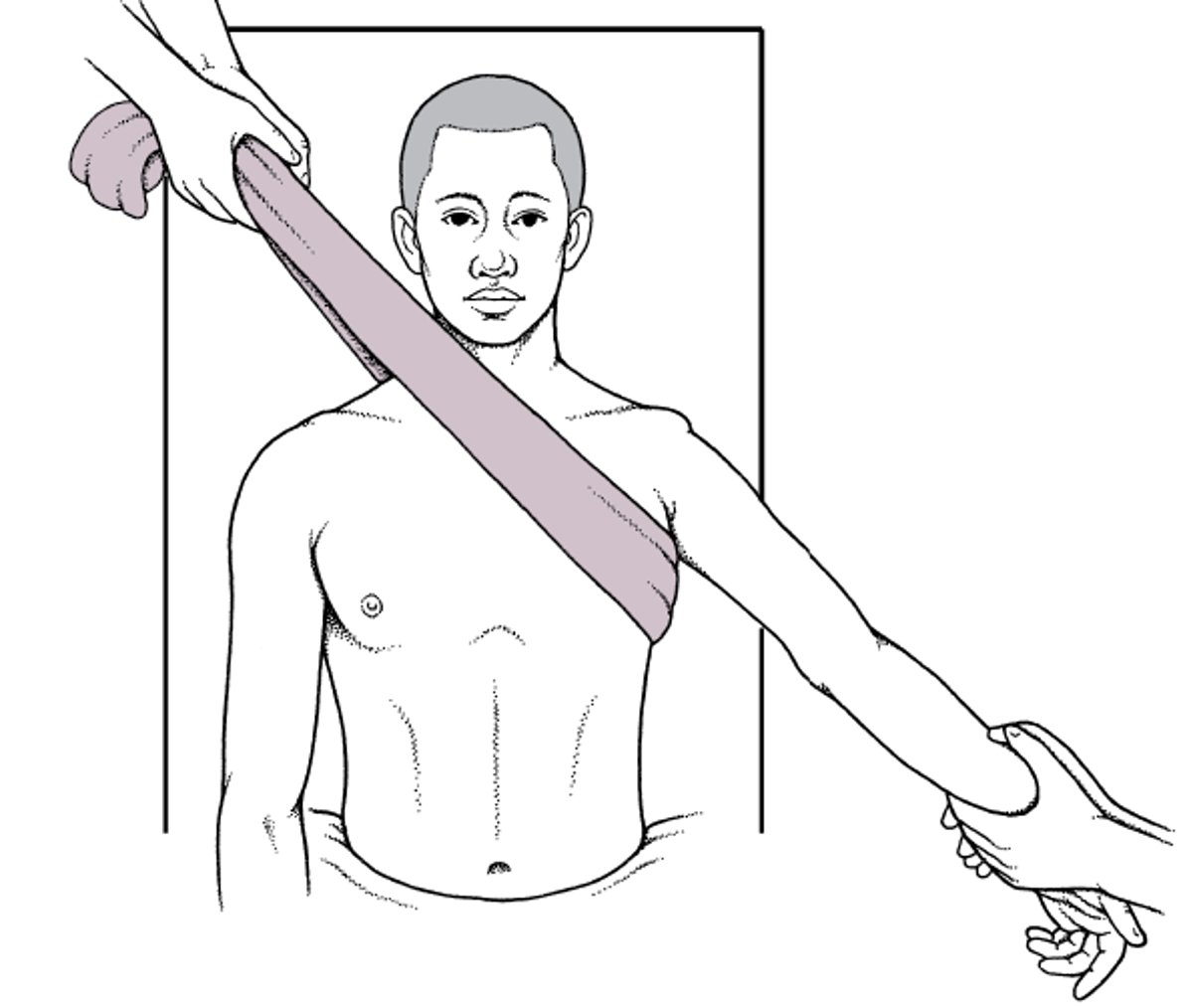
External rotation: An example is the Hennepin technique. The practitioner bends the arm at the elbow, then slowly rotates the arm away from the body.
Putting a Shoulder Back in Place: Hennepin Technique
The practitioner bends the arm, then slowly rotates the arm away from the body. |


Shoulder blade (scapular) manipulation: This maneuver can be done with the person sitting up or lying down. The practitioner moves the bottom tip of the shoulder blade toward the spine. An assistant pulls, rotates, and may apply gentle pressure to the arm.
Cunningham (massage) technique: The practitioner sits opposite the person and places the person's hand on the practitioner's shoulder. Then the practitioner massages the muscles in the upper arm and shoulder and instructs the person to relax and to shrug the shoulders back, trying to make the shoulder blades touch each other. Massage helps the muscles relax so that the person can slip the shoulder back in place.
Davos (autoreduction) technique: The person sits on a bed, bends the knee on the side of the affected shoulder, and puts that foot on the bed. The person clasps the hands in front of the knee with the elbows close to the thigh, and an elastic band is wrapped around the hands, tying them together and to the knee to hold the hands in place. The practitioner then sits on person's foot and instructs the person to lean the head back. By leaning their head back, people put pressure on the dislocated shoulder, which helps put it back in place.
Stimson (dangling weights) technique: The person lies on a bed face down with the arm of the dislocated shoulder hanging over the side of a bed. Weights are attached to the person's wrist. After about 30 minutes, the shoulder muscles usually relax enough for the shoulder to move back in place.
FARES (fast and reliable) technique: The person lies face up with the elbow extended and arm by the body. The practitioner holds the person's arm by the hand or wrist and slowly moves the arm away from the person's body. At the same time, the practitioner moves the arm up and down in small, slow, up-and-down oscillating movements. This movement helps the muscles relax.
After reduction, the joint is immobilized immediately with a sling and swathe. In people over age 40, the sling and swathe is used for less time than in younger people to encourage movement and help prevent complications (for example, frozen shoulder).
Sling and Swathe









