






Urinalysis, the testing of urine, may be necessary in the evaluation of kidney and urinary tract disorders and can also help evaluate bodywide disorders such as diabetes or liver problems. A urine sample is usually collected using the clean-catch method or another sterile method. For example, a method to obtain an uncontaminated urine sample involves passing a catheter through the urethra into the bladder.
Urine cultures, in which bacteria from a urine sample are grown in a laboratory, are done to diagnose a urinary tract infection. Cultures are not part of routine urinalysis. The sample of urine must be obtained by the clean-catch method (see sidebar Obtaining a Clean-Catch Urine Sample) or by briefly inserting a sterile catheter through the urethra into the bladder.

Urinalysis involves
Chemical tests to detect and measure the level of various substances in the urine
Often, examining urine under a microscope
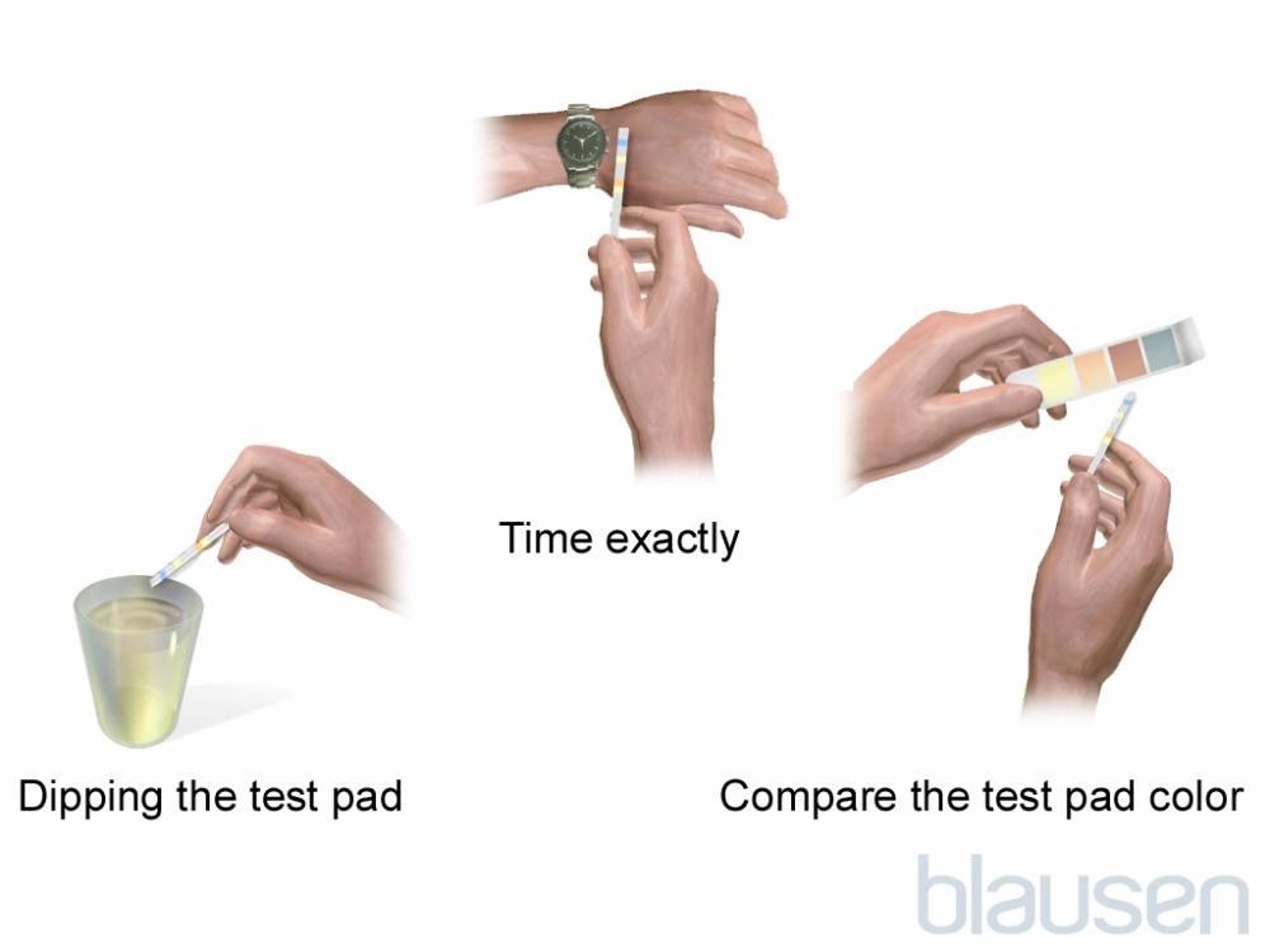
Chemical tests look for protein, glucose (sugar), ketones, blood, and other substances. These tests use a thin strip of plastic (dipstick) impregnated with chemicals that react with substances in the urine and quickly change color. Sometimes the test results are confirmed with more sophisticated and accurate laboratory analysis of the urine.
Examining the urine under a microscope may be done to check for the presence of red and white blood cells, crystals, and casts (impressions of the kidney tubules created when urinary cells, protein, or both precipitate out in the tubules and are passed in the urine).

Protein in the urine (proteinuria) can usually be detected by dipstick when present in large amounts. Protein may appear constantly or only intermittently in the urine, depending on the cause. Proteinuria may occur normally after strenuous exercise, such as marathon running, but is usually a sign of a kidney disorder. Small amounts of protein in the urine may be an early sign of kidney damage due to diabetes. Such small amounts may not be detected by dipstick. In these cases, urine will need to be collected over a period of 12 or 24 hours and tested by a laboratory.
Glucose in the urine (glucosuria) can be accurately detected by dipstick. The most common cause of glucose in the urine is diabetes mellitus, but absence of glucose does not mean a person does not have diabetes or that the diabetes is well controlled. Also, presence of glucose does not necessarily indicate diabetes or another problem.
Ketones in the urine (ketonuria) can often be detected by dipstick. Ketones are formed when the body breaks down fat. Ketones can appear in the urine as a result of starvation or fasting, uncontrolled diabetes mellitus, or in people who have had excessive amounts of alcohol (usually people with alcohol use disorder).
Blood in the urine (hematuria) is detectable by dipstick and confirmed by viewing the urine with a microscope and other tests. Sometimes the urine contains enough blood to be visible, making the urine appear red or brown.
Nitrites in the urine (nitrituria) are also detectable by dipstick. High nitrite levels indicate a urinary tract infection.
Leukocyte esterase (an enzyme found in certain white blood cells) in the urine can be detected by dipstick. Leukocyte esterase is a sign of inflammation, which is most commonly caused by a urinary tract infection.
The acidity (pH) of urine is measured by dipstick. Certain foods, chemical imbalances, and metabolic disorders may change the acidity of urine. Sometimes a change in acidity can predispose the person to kidney stones.
The concentration of urine (also called the osmolality, roughly indicated by specific gravity) can vary widely depending on whether a person is dehydrated, how much fluid a person has drunk, and other factors. Urine concentration is also sometimes important in diagnosing abnormal kidney function. The kidneys lose their capacity to concentrate urine at an early stage of a disorder that leads to kidney failure. In one special test, a person drinks no water or other fluids for 12 to 14 hours. In another test, a person receives an injection of vasopressin (also called antidiuretic hormone). Afterward, urine concentration is measured. Normally, either test should make the urine highly concentrated. However, in certain kidney disorders (such as nephrogenic diabetes insipidus), the urine cannot be concentrated even though other kidney functions are normal.
Sediment in urine can be examined under a microscope to provide information about a possible kidney or urinary tract disorder. Normally, urine contains a small number of cells and other debris shed from the inside of the urinary tract. A person who has a kidney or urinary tract disorder usually sheds more cells, which form a sediment if urine is spun in a centrifuge (a laboratory instrument that uses centrifugal force to separate components of a liquid) or allowed to settle.






