








Usually, bacteria are the cause of cystitis.
A frequent need to urinate and pain or burning while urinating are the most common symptoms.
Doctors can often base the diagnosis on the symptoms, but they usually examine a urine specimen.
Medications are needed to treat the infection and often the symptoms.
(See also Overview of Urinary Tract Infections [UTIs].)
Causes of Bladder Infection
Causes of bladder infection in women
Cystitis is common among women, particularly during the reproductive years. Some women have recurring episodes of cystitis. There are a number of reasons why women are susceptible, including the short length of the urethra and the closeness of the opening of the urethra to the vagina and anus, where bacteria are commonly found. Sexual intercourse can contribute, too, because the motion can cause bacteria to reach the opening of the urethra, from which they ascend to the bladder. Pregnant women are especially likely to develop cystitis because the pregnancy itself can interfere with emptying of the bladder.
Use of a diaphragm for contraception increases the risk of developing cystitis, possibly because spermicide used with the diaphragm suppresses the normal vaginal bacteria and allows bacteria that cause cystitis to flourish in the vagina. Having sex with a man who uses a condom coated with spermicide also increases the risk.
The decrease in estrogen production that occurs after menopause can thin the vaginal and vulvar tissues around the urethra, which can predispose a woman to repeated episodes of cystitis. In addition, a drooping (prolapsed) uterus or bladder may cause poor emptying of the bladder and predispose to cystitis. A prolapsed uterus or bladder is more common among women who have had many children.

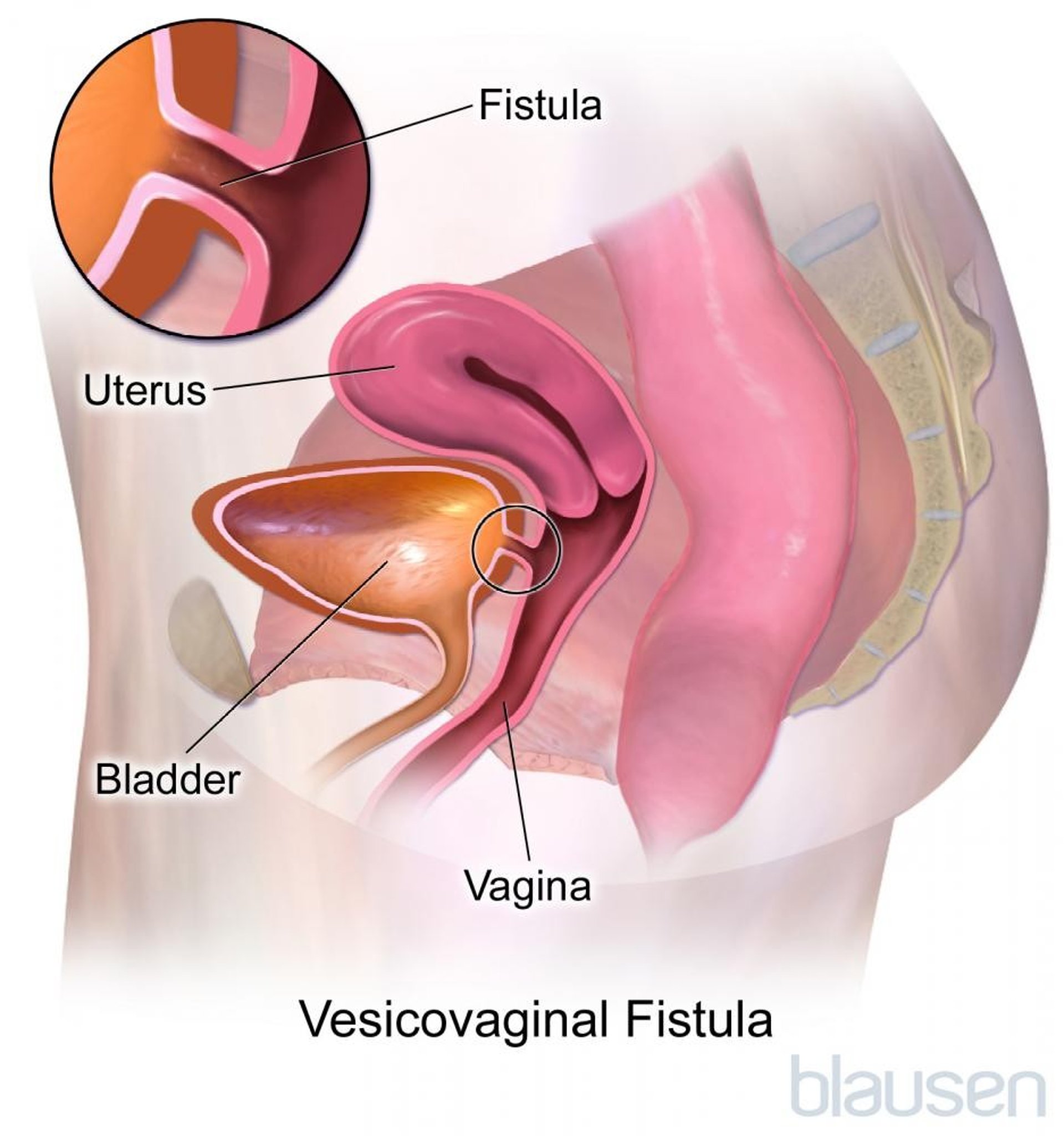
Rarely, cystitis recurs because of an abnormal connection between the bladder and the vagina (vesicovaginal fistula).
Causes of bladder infection in men

Cystitis is less common among men. In men, a common cause is bacterial infection of the prostate, which causes repeated episodes of cystitis and urethritis. Although antibiotics quickly clear bacteria from the urine in the bladder, most of these medications cannot penetrate well enough into the prostate to quickly cure an infection there. Usually antibiotics must be taken for weeks at a time. Consequently, if antibiotic therapy is stopped prematurely, bacteria that remain in the prostate tend to reinfect the bladder.
Causes of bladder infection in both sexes
If the flow of urine becomes partly blocked (obstructed) because of a stone in the bladder or urethra, an enlarged prostate (in men), or a narrowing (stricture) of the urethra, bacteria that enter the urinary tract are less likely to be flushed out with urine. Bacteria that are left in the bladder after urinating can multiply rapidly. People with long-standing or repeated obstruction of urine flow may develop a bladder outpouching (diverticulum). This pocket retains urine after urinating, further increasing the risk of infection.
Cystitis can also be caused by a catheter or any instrument inserted into the urinary tract that introduces bacteria into the bladder.
Sometimes the bladder can become inflamed without an infection being present, a disorder called interstitial cystitis.
Symptoms of Bladder Infection
Cystitis usually causes a frequent, urgent need to urinate and a burning or painful sensation while urinating. These symptoms usually develop over several hours or a day. The urgent need to urinate may cause an uncontrollable loss of urine (urge incontinence), especially in older adults. Fever is rarely present. Pain is usually felt above the pubic bone and often in the lower back as well. Frequent urination during the night (nocturia) may be another symptom. The urine may be cloudy in severe infection. Uncommonly, when infection results from an abnormal connection between the bladder and the intestine or the vagina (fistula), air can be passed in the urine (pneumaturia).
Sometimes cystitis causes no symptoms, particularly in older adults, and is discovered when urine tests are done for other reasons. Among older adults, cystitis may also cause no symptoms related to urinating and may cause symptoms such as fever or confusion. A person whose bladder is malfunctioning because of nerve damage (neurogenic bladder) or a person who has a catheter may have cystitis with no symptoms until a kidney infection or fever develops.
Diagnosis of Bladder Infection
Urinalysis
Urine culture
Doctors can usually diagnose cystitis based on its typical symptoms. A midstream (clean-catch) urine specimen is collected so that the urine is not contaminated with bacteria from the vagina or the tip of the penis. A strip of test paper is sometimes dipped into the urine to do 2 quick and simple tests for substances that are normally not found in the urine. The testing strip can detect nitrites that are released by bacteria. The testing strip can also detect leukocyte esterase (an enzyme found in certain white blood cells), which may indicate that the body is fighting the infection. In adult women, these may be the only tests necessary.
In addition, the urine specimen can be examined under a microscope to see the number of red and white blood cells and whether it contains bacteria. Sometimes, urine cultures, in which bacteria from a urine sample are grown in a laboratory, are done to identify the numbers and type of bacteria. If the person has an infection, one type of bacteria is usually present in large numbers.
In men, a midstream urine specimen is usually sufficient for a urine culture. In women, a specimen is more likely to be contaminated with bacteria from the vagina or vulva. When the urine contains several different types of bacteria simultaneously, the urine has likely been contaminated during the collection process. To ensure that the urine is not contaminated, doctors sometimes must obtain a specimen directly from the bladder with a catheter.

Finding the cause of cystitis
It is important for doctors to find the cause of cystitis in several different groups. The cause should be found in
Children
Men of any age
People who have fevers for at least 3 days or evidence of kidney damage
Some women with frequently recurring infections (3 or more per year), especially when accompanied by symptoms of urinary obstruction (including symptoms of a kidney stone)
In these types of people, there is a greater likelihood of finding a cause (for example, a large kidney stone) that requires treatment other than simply giving antibiotics to treat the infection.
Doctors may do an imaging study, usually
Ultrasonography
Computed tomography (CT)
Sometimes, instead of ultrasonography or CT, doctors do an intravenous urogram (IVU), an x-ray study in which a radiopaque contrast agent is injected into a vein, then excreted into the urine by the kidneys. (See also Imaging Tests of the Urinary Tract.) The x-rays then provide images of the kidneys, ureters, and bladder.
Voiding cystourethrography, which involves injecting a radiopaque contrast agent into the bladder and filming its exit, is a good way for doctors to investigate the backflow (reflux) of urine from the bladder, up the ureters, particularly in children, and may also identify any narrowing (stricture) of the urethra.
Retrograde urethrography, in which the radiopaque contrast agent is injected directly into the urethra, is useful for detecting stricture, outpouching, or an abnormal connection (fistula) of the urethra in both men and women.
Looking directly into the bladder with a flexible viewing tube (cystoscopy) may help diagnose the problem when cystitis does not resolve with treatment. Doctors also try to find a cause in men who have cystitis. Prostatitis, the most common cause, can usually be diagnosed by examination of the prostate and urine tests.
In women who have recurrent urinary tract infection (UTI), doctors do a pelvic examination to detect manageable conditions like vaginal atrophy (thinning, drying, and inflammation of the vaginal walls), urethral diverticulum (the formation of a pocket or sac along the urethra), fecal incontinence, and vaginal prolapse. Men with recurrent UTI should be evaluated for prostatitis, urethritis, and urinary retention (incomplete bladder emptying).
Treatment of Bladder Infection
Antibiotics
Analgesics as needed
Sometimes surgery
Cystitis is usually treated with antibiotics. Before prescribing antibiotics, the doctor determines whether the person has a condition that would make cystitis more severe, such as diabetes or a weakened immune system (which reduces the person's ability to fight infection), or more difficult to eliminate, such as a structural abnormality. Such conditions may require more potent antibiotics taken for a longer period of time. People with such conditions may also have infections caused by fungi or unusual bacteria and may thus require something other than the most commonly used antibiotics.
For women, taking an antibiotic by mouth for 3 days is usually effective if the infection has not led to any complications, although some doctors prefer to give a single dose. For more stubborn infections, an antibiotic is usually taken for 7 to 10 days. For men, cystitis usually is caused by prostatitis, and antibiotic treatment is usually required for weeks.
A variety of medications can relieve symptoms, especially the frequent, insistent urge to urinate and painful urination. Phenazopyridine may help reduce the pain by soothing the inflamed tissues and can be taken for a couple of days, until antibiotics control the infection. A variety of medications can relieve symptoms, especially the frequent, insistent urge to urinate and painful urination. Phenazopyridine may help reduce the pain by soothing the inflamed tissues and can be taken for a couple of days, until antibiotics control the infection.
Surgery may be necessary to relieve any physical obstruction to the flow of urine or to correct a structural abnormality that makes infection more likely, such as a drooping uterus or bladder. Until surgery can occur, draining urine from an obstructed area through a catheter helps control the infection. Usually, an antibiotic is given before surgery to reduce the risk of the infection spreading throughout the body.
Preventing Bladder Infections in Women
In women who experience 3 or more bladder infections in a year, these measures may help:
|
Prevention of Bladder Infection
If women tend to develop bladder infections after sexual intercourse, they may be advised to take an antibiotic dose immediately after intercourse. Spermicides and diaphragm use should be avoided, and women should urinate as soon as possible after sexual intercourse.
People who have frequent bladder infections may continually take low doses of antibiotics. Women who take antibiotics regularly to prevent bladder infections may need to discuss contraceptive options with their doctor. Postmenopausal women with frequent bladder infections and the genitourinary syndrome of menopause may benefit from estrogen creams applied to the vulva or estrogen suppositories inserted into the vagina.
Drinking plenty of fluids may help prevent cystitis. The flushing action of the urine washes many bacteria out of the bladder. The body's natural defenses eliminate the remainder of the bacteria.
The use of cranberry products may be helpful in preventing recurrent bladder infections, but more research is needed to clarify who would benefit from their use.The use of cranberry products may be helpful in preventing recurrent bladder infections, but more research is needed to clarify who would benefit from their use.
It is commonly believed that wiping from front to back, and avoiding the use of tight, nonporous underwear helps women prevent bladder infections.
Did You Know...
|
Drugs Mentioned In This Article






