



Portal hypertension is abnormally high blood pressure in the portal vein (the large vein that brings blood from the intestine to the liver) and its branches.
Topic Resources


Cirrhosis (scarring that distorts the structure of the liver and impairs its function) is the most common cause in Western countries.
Portal hypertension can lead to a swollen abdomen (ascites), abdominal discomfort, confusion, and bleeding in the digestive tract.
Doctors base the diagnosis on symptoms and results of a physical examination, sometimes with ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), or liver biopsy.
Drugs can reduce blood pressure in the portal vein, but if bleeding in the digestive tract occurs, emergency treatment is required.
Treatment sometimes includes liver transplantation or creation of a tract through which blood can bypass the liver (portosystemic shunt).
(See also Overview of Liver Disease.)

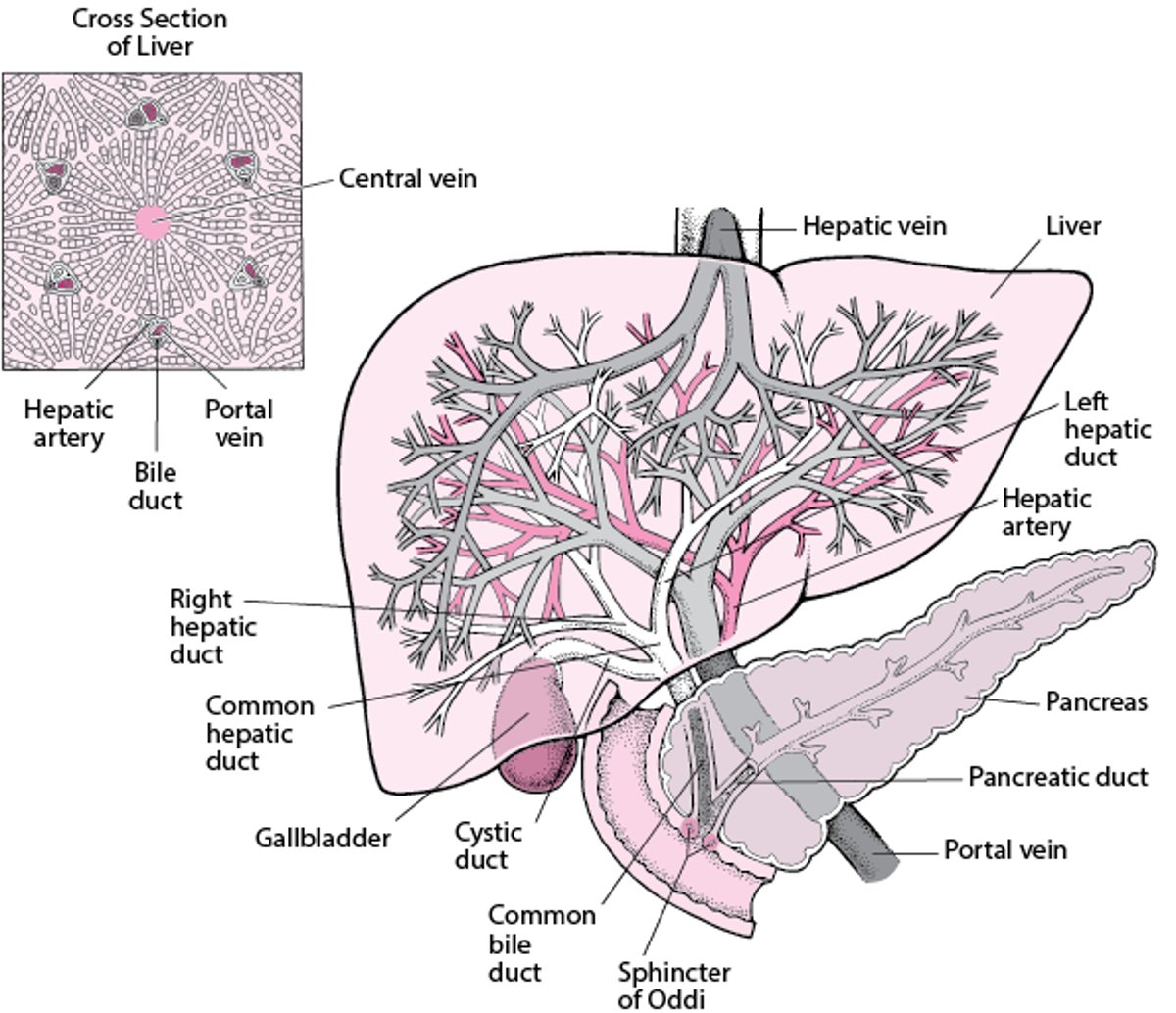
The portal vein receives blood from the entire intestine and from the spleen, pancreas, and gallbladder and carries that blood to the liver. After entering the liver, the vein divides into right and left branches and then into tiny channels that run through the liver. When blood leaves the liver, it flows back into the general circulation through the hepatic vein.
View of the Liver and Gallbladder

Two factors can increase blood pressure in the portal blood vessels:
An increased volume of blood flowing through the vessels
Increased resistance to the blood flow through the liver
In Western countries, the most common cause of portal hypertension is increased resistance to blood flow caused by extensive scarring of the liver in cirrhosis. Cirrhosis is most often caused by
Chronic hepatitis C (hepatitis that has lasted at least 6 months)
Drinking large amounts of alcohol over a long period of time
Portal hypertension leads to the development of new veins (called collateral vessels) that bypass the liver. These veins directly connect the portal blood vessels to veins that take blood away from the liver into the general circulation. Because of this bypass, substances (such as toxins) that are normally removed from the blood by the liver can pass into the general circulation. Collateral vessels develop at specific places. The most important are located at the lower end of the esophagus and at the upper part of the stomach. Here, the vessels enlarge and become full of twists and turns—that is, they become varicose veins in the esophagus (esophageal varices) or stomach (gastric varices). These enlarged vessels are fragile and prone to bleeding, sometimes seriously and occasionally with fatal results. Other collateral vessels may develop on the abdominal wall and at the rectum.
Portal hypertension often causes the spleen to enlarge because the pressure interferes with blood flow from the spleen into the portal blood vessels. When the spleen enlarges, the number (count) of white blood cells can decrease (increasing the risk of infections), and the number (count) of platelets can decrease (increasing the risk of bleeding).
Increased pressure in the portal blood vessels may cause protein-containing (ascitic) fluid to leak from the surface of the liver and intestine and to accumulate within the abdomen. This condition is called ascites.
Symptoms of Portal Hypertension
Portal hypertension itself does not cause symptoms, but some of its consequences do. If a large amount of fluid accumulates in the abdomen (called ascites), the abdomen swells (distends), sometimes noticeably and sometimes enough to make the abdomen greatly enlarged and taut. This distention can be uncomfortable or painful. An enlarged spleen may cause a vague sense of discomfort in the upper left part of the abdomen.
The varicose veins in the esophagus and stomach bleed easily and sometimes massively. Then, people may vomit blood or dark material that resembles coffee grounds. Stools may be dark and tarry. Much less commonly, varicose veins in the rectum bleed. Then, stools may contain red blood. Bleeding from these veins may result in death.
Collateral blood vessels may be visible on the skin of the abdomen or around the rectum.
When substances that are normally removed from the liver pass into the general circulation and reach the brain, they may cause confusion or drowsiness (hepatic encephalopathy). Because most people with portal hypertension also have severe liver malfunction, they may have symptoms of liver failure, such as a tendency to bleed.
Diagnosis of Portal Hypertension
A doctor's evaluation
Sometimes blood tests and tests to evaluate mental function
Imaging tests, such as ultrasonography
Usually, doctors can recognize portal hypertension based on symptoms and findings during the physical examination. Doctors can usually feel an enlarged spleen when they examine the abdomen. They can detect fluid in the abdomen by noting abdominal swelling and by listening for a dull sound when tapping (percussing) the abdomen.
Doctors may suspect hepatic encephalopathy based on symptoms (such as confusion), but blood tests and tests designed to evaluate mental function may be needed.
Ultrasonography may be used to examine blood flow in the portal vein and nearby blood vessels and to detect fluid in the abdomen. Ultrasonography, magnetic resonance imaging (MRI), or computed tomography (CT) can be used to look for and examine collateral vessels (see Imaging Tests of the Liver and Gallbladder).
Less commonly, a catheter is inserted through an incision in the neck and threaded through blood vessels into the liver to measure pressure in the portal blood vessels.
Treatment of Portal Hypertension
For bleeding, drugs to slow bleeding, blood transfusions, and/or endoscopy
Sometimes surgery to reroute blood flow (portosystemic shunting)
Sometimes liver transplantation
Control of bleeding
Bleeding from esophageal varices is a medical emergency. Drugs such as vasopressin or octreotide may be given intravenously to make the bleeding veins contract and thus slow the bleeding. Blood transfusions are given to replace lost blood. Doctors usually use a flexible viewing tube (endoscope), inserted through the mouth into the esophagus to confirm that the bleeding is from varices. Working through the endoscope, doctors can use rubber bands to tie off the veins.is a medical emergency. Drugs such as vasopressin or octreotide may be given intravenously to make the bleeding veins contract and thus slow the bleeding. Blood transfusions are given to replace lost blood. Doctors usually use a flexible viewing tube (endoscope), inserted through the mouth into the esophagus to confirm that the bleeding is from varices. Working through the endoscope, doctors can use rubber bands to tie off the veins.
To reduce the risk of bleeding from esophageal varices, doctors may try to reduce pressure in the portal vein. One way is to give beta-blocker drugs, such as timolol, propranolol, nadolol, or carvedilol.To reduce the risk of bleeding from esophageal varices, doctors may try to reduce pressure in the portal vein. One way is to give beta-blocker drugs, such as timolol, propranolol, nadolol, or carvedilol.
Doctors regularly monitor people who have had bleeding from varices because bleeding may recur.
Portosystemic shunting
If the bleeding continues or recurs repeatedly, a procedure called portosystemic shunting may be done to connect the portal vein or one of its branches to a vein in the general circulation. This procedure reroutes most of the blood that normally goes to the liver so that it bypasses the liver. This bypass (called a shunt) lowers pressure in the portal vein because pressure is much lower in the general circulation.
There are various types of portosystemic shunt procedures. In one type, called transjugular intrahepatic portosystemic shunting (TIPS), doctors, using x-rays for guidance, insert a catheter with a needle into a vein in the neck and thread it to veins in the liver. The catheter is used to create a passage (shunt) that connects the portal vein (or one of its branches) directly with one of the hepatic veins. Less commonly, portosystemic shunts are created surgically.
Shunt procedures are usually successful in stopping the bleeding but pose certain risks, particularly hepatic encephalopathy. The procedure may have to be repeated because the shunt may become blocked.
Liver transplantation
Some people require liver transplantation.







