



Asthma is a condition in which the airways narrow—usually reversibly—in response to certain stimuli.









Coughing, wheezing, and shortness of breath that occur in response to specific triggers are the most common symptoms.
Doctors confirm the diagnosis of asthma by doing breathing (pulmonary function) tests.
To prevent attacks, people should avoid substances that trigger asthma and should take drugs that help keep airways open.
During an asthma attack, people need to take a drug that quickly opens the airways.
(See also Asthma in Children, Wheezing in Infants and Young Children, and Asthma During Pregnancy.)
Asthma affects more than 25 million people in the United States, and it is becoming more common. The reason for the increase in asthma is not known.

Although asthma is one of the most common chronic diseases of childhood, adults can also develop asthma, even at an old age. Asthma affects more than 5 million children (see also Asthma in Children) in the United States. Asthma can eventually resolve in children. However, sometimes asthma that appears to resolve recurs years later.
Asthma also occurs more frequently in non-Hispanic Blacks and Puerto Ricans. Although the number of people affected by asthma has increased, the number of deaths has decreased.

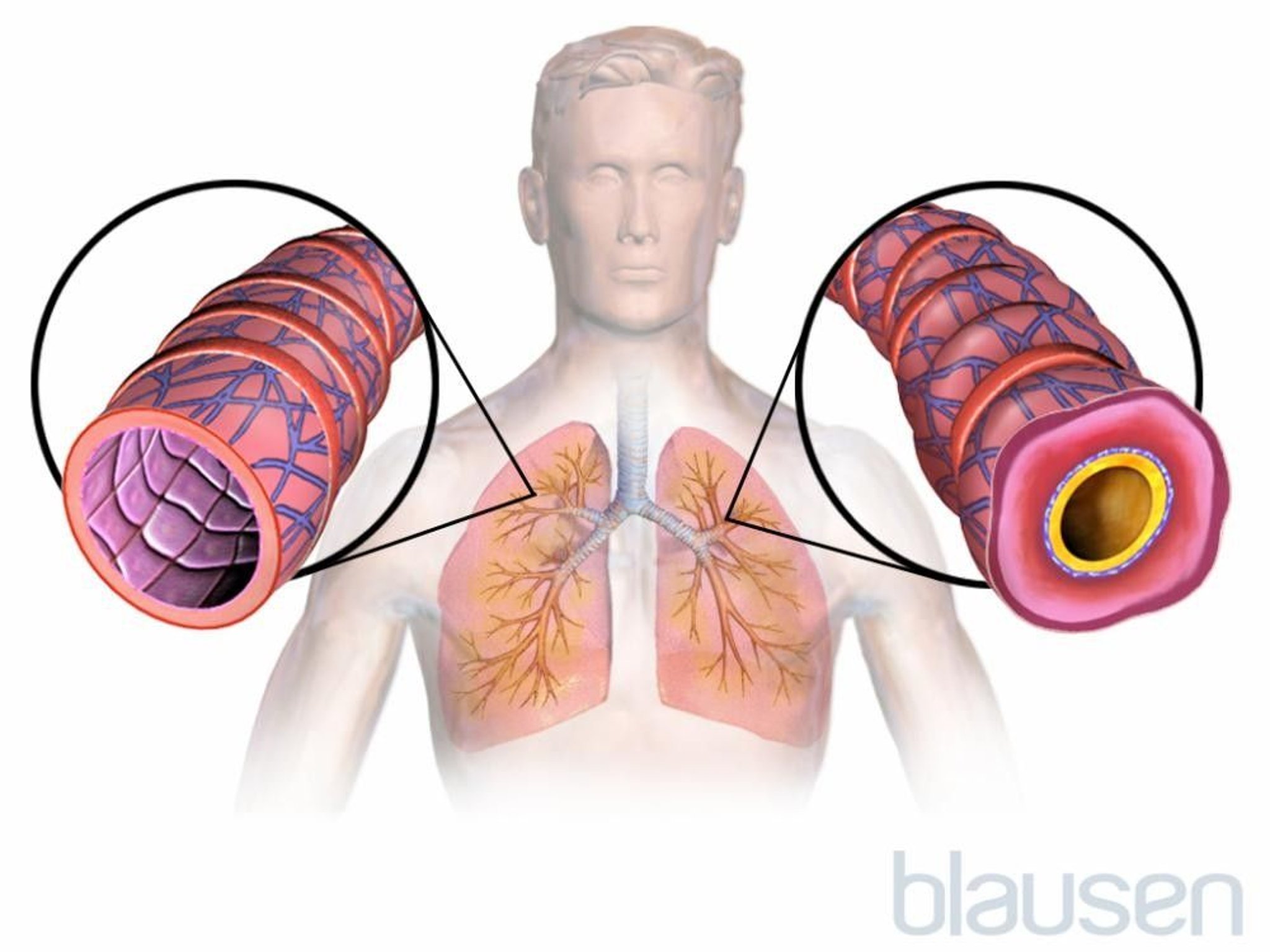
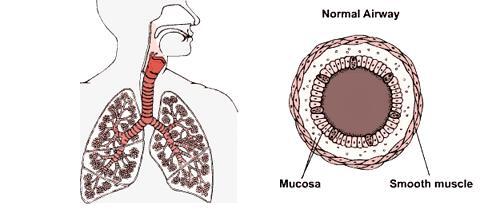
The most important characteristic of asthma is narrowing of the airways that can be reversed. The airways of the lungs (the bronchi) are basically tubes with muscular walls. Cells lining the bronchi have microscopic structures, called receptors. These receptors sense the presence of specific substances and stimulate the underlying muscles to contract or relax, thus altering the flow of air. There are many types of receptors, but two main types of receptors are important in asthma:
Beta-adrenergic receptors respond to chemicals such as epinephrine and make the muscles relax, thereby widening (dilating) the airways and increasing airflow.
Cholinergic receptors respond to a chemical called acetylcholine and make the muscles contract, thereby decreasing airflow.
Causes of Asthma
The causes of asthma are unknown, but asthma likely results from complex interactions between many genes, environmental conditions, and nutrition. Environmental conditions and circumstances around pregnancy, birth, and infancy have been associated with the development of asthma in childhood and later in adulthood. Risk appears to be higher if a person's mother became pregnant at a young age or had poor nutrition during pregnancy. Risk may also be higher if someone is born prematurely, had a low weight at birth, or was not breastfed. Environmental conditions such as exposures to household allergens (such as dust mites, cockroaches, and pet dander) and other environmental allergens have also been associated with the development of asthma in older children and adults. Diets low in vitamins C and E and in omega–3 fatty acids have been also linked to asthma, as has obesity. There is no evidence that dietary supplements of these substances prevent the development of asthma; however, it has been shown that weight loss can reduce the risk and severity of asthma. Thus, obesity is an important modifiable risk factor for asthma.
Having smaller families with fewer children, cleaner indoor environments, and use of vaccinations and antibiotics in early life may decrease the body's ability to develop resistance to allergens in the environment and may partly explain the increase in asthma in places where these conditions exist (the hygiene hypothesis).
Narrowing of the airways is often caused by abnormal sensitivity of cholinergic receptors, which cause the muscles of the airways to contract when they should not. Certain cells in the airways, particularly mast cells, are thought to be responsible for initiating the response. Mast cells throughout the bronchi release substances such as histamine and leukotrienes, which cause the following:
Smooth muscle to contract
Mucus secretion to increase
Certain white blood cells to move to the area
Eosinophils, a type of white blood cell found in the airways of people with asthma, release additional substances, contributing to airway narrowing.
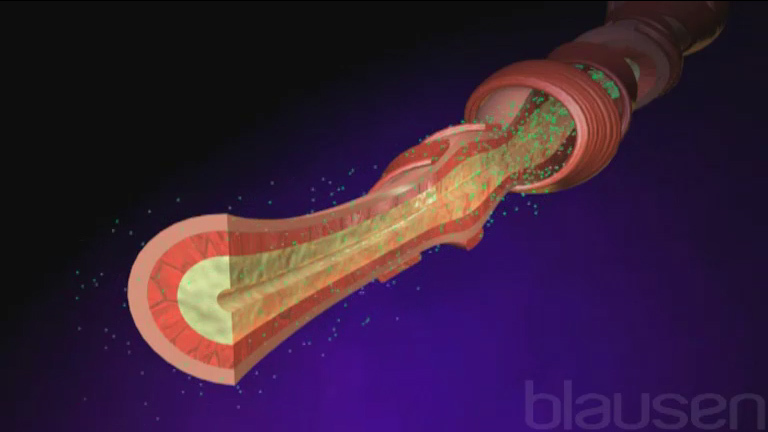
In an asthma attack (sometimes called a flare-up or an exacerbation), the smooth muscles of the bronchi contract, causing the bronchi to narrow (called bronchoconstriction). The tissues lining the airways swell due to inflammation and mucus secretion into the airways. The top layer of the airway lining can become damaged and shed cells, further narrowing the airway. A narrower airway requires the person to exert more effort to breathe. In asthma, the narrowing is reversible, meaning that with appropriate treatment or on their own, the muscular contractions of the airways stop, inflammation resolves so that the airways widen again, and airflow into and out of the lungs returns to normal.
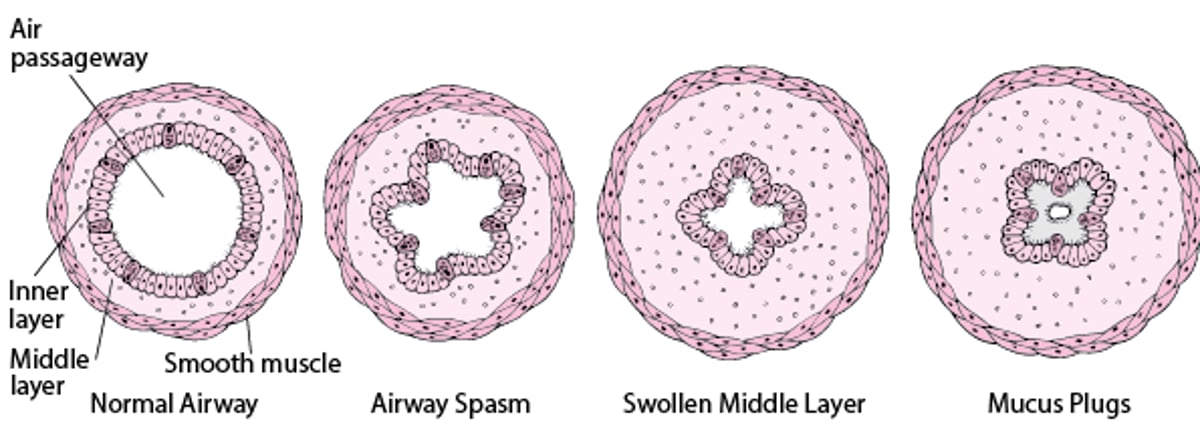
How Airways Narrow
During an asthma attack, the smooth muscle layer goes into spasm, narrowing the airway. The middle layer swells because of inflammation, and excessive mucus is produced. In some segments of the airway, mucus forms plugs that nearly or completely block the airway. |

Asthma triggers
In people who have asthma, the airways narrow in response to stimuli (triggers) that usually do not affect the airways in people without asthma. Such triggers include
Allergens
Infections
Irritants
Exercise (called exercise-induced asthma)
Stress and anxiety
AspirinAspirin
Many inhaled allergens, including pollens, particles from dust mites, body secretions from cockroaches, particles from feathers, and animal dander, can trigger an asthma attack. These allergens combine with immunoglobulin E (IgE, a type of antibody) on the surface of mast cells to trigger the release of asthma-causing chemicals. (This type of asthma is called allergic asthma.) Although food allergies induce asthma only rarely, certain foods (such as shellfish and peanuts) can induce severe attacks in people who are sensitive to these foods.
Infectious triggers are usually viral respiratory infections, such as colds, bronchitis, and, less commonly, pneumonia.
Irritants that can provoke an asthma attack include smoke from tobacco, marijuana, or cocaine; fumes (such as from perfumes, cleaning products, or air pollution); cold air; and stomach acid in the airways caused by Irritants that can provoke an asthma attack include smoke from tobacco, marijuana, or cocaine; fumes (such as from perfumes, cleaning products, or air pollution); cold air; and stomach acid in the airways caused bygastroesophageal reflux disease (GERD). Air pollution has been linked to asthma attacks.
Some people who have asthma can develop airway narrowing when exercising. This type of airway narrowing may be due to breathing drier, colder air through the mouth while exercising.
Stress and anxiety can trigger mast cells to release histamine and leukotrienes and stimulate the vagus nerve (which connects to the airway smooth muscle), which then contracts and narrows the bronchi.
Crying or hearty laughing may trigger symptoms in some people.
Aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) are triggers for almost 30% of people with severe asthma, but they are triggers in less than 10% of people with asthma overall.Aspirin and nonsteroidal anti-inflammatory drugs (NSAIDs) are triggers for almost 30% of people with severe asthma, but they are triggers in less than 10% of people with asthma overall.
Eosinophilic asthma
Eosinophilic asthma is a rare, severe subtype of asthma in which very high levels of eosinophils are present in the blood. The higher the level of eosinophils the more severe the person's symptoms.
Reactive airways dysfunction syndrome
Reactive airways dysfunction syndrome (RADS) is a rapid onset and persistent asthma-like disorder that occurs in people with no history of asthma. It is a form of environmental lung disease caused by a single large exposure to nitrogen oxide or volatile organic compounds (such as those in certain bleaches and cleaning products). People have symptoms similar to those of asthma, including cough, wheezing, and shortness of breath. Treatment is similar to usual treatment for asthma.
Symptoms of Asthma
Asthma attacks vary in frequency and severity. Some people who have asthma are symptom-free most of the time, with only an occasional brief, mild episode of shortness of breath. Other people cough and wheeze most of the time and have severe attacks after viral infections, exercise, or exposure to other triggers.
Wheezing is a musical sound that occurs when the person breathes out. Coughing may be the only symptom in some people (cough-variant asthma). Some people with asthma produce a clear, sometimes sticky (mucoid) phlegm (sputum).

In some people, asthma attacks occur primarily at night (nocturnal asthma). Attacks that occur during the night may indicate poorly controlled asthma.
Did You Know...
|
Symptoms of an asthma attack
Asthma attacks occur most often in the early morning hours when the effects of protective drugs wear off and the body is least able to prevent airway narrowing.
An asthma attack may begin suddenly with wheezing, coughing, and shortness of breath. At other times, an asthma attack may come on slowly with gradually worsening symptoms. In either case, people with asthma usually first notice shortness of breath, coughing, or chest tightness. The attack may be over in minutes, or it may last for hours or days. Itching on the chest or neck may be an early symptom, especially in children. A dry cough at night or while exercising may be the only symptom.
During an asthma attack, shortness of breath may become severe, creating a feeling of severe anxiety. The person instinctively sits upright and leans forward, using the muscles in the neck and chest to help in breathing, but still struggles for air. Sweating is a common reaction to the effort and anxiety. The heart rate usually quickens, and the person may feel a pounding in the chest.
In a very severe asthma attack, a person is able to say only a few words without stopping to take a breath. Wheezing may actually diminish, however, because hardly any air is moving in and out of the lungs. Confusion, lethargy, and a blue skin color (cyanosis) are signs that the person’s oxygen supply is severely limited, and emergency treatment is needed. Usually, a person recovers completely with appropriate treatment, even from a severe asthma attack. Rarely, some people develop attacks so quickly that they may lose consciousness before they can give themselves effective therapy. Such people should wear identification (such as a medical alert bracelet or necklace) and carry a cellular phone to call for emergency medical assistance.
Classification of Asthma
Unlike high blood pressure (in which one factor, the blood pressure value, defines the severity of the disorder and the effectiveness of treatment), asthma causes a number of symptoms and testing abnormalities. Also, asthma symptoms typically worsen and improve over time. Doctors evaluate the severity of asthma, and after treatment starts, they monitor how well the person's symptoms are controlled because that information helps doctors determine whether additional drugs are needed.
Asthma severity
Severity is a measure of how bad a disease is. Asthma severity is usually assessed before treatment is started, because people who have responded well to treatment have few symptoms. Asthma severity is categorized as
Intermittent: The person's symptoms occur two days per week or less and do not interfere with activities of daily life
Mild persistent: The person's symptoms occur more than twice per week but only slightly limit activities of daily life
Moderate persistent: The person's symptoms occur daily and limit some activities of daily life
Severe persistent: The person's symptoms occur throughout the day and interfere excessively with activities of daily life
It is important to remember that the severity category does not predict how serious an attack a person may have. Even a person who has mild asthma with long periods of no or mild symptoms and normal lung function may have a severe, life-threatening asthma attack.
Status asthmaticus
The most severe form of asthma is called status asthmaticus. It is severe, intense, prolonged airway narrowing that is resistant to treatment. In status asthmaticus, the lungs are no longer able to provide the body with adequate oxygen or to remove carbon dioxide adequately.
Without oxygen, many organs begin to malfunction. The buildup of carbon dioxide leads to acidosis, an acidic state of the blood that affects the function of almost every organ. Blood pressure may fall to dangerously low levels. The airways are so narrowed that it is difficult to move air in and out of the lungs.
Status asthmaticus may require that an artificial airway be passed through the person’s mouth and throat into the main airway leading to the lungs (the trachea) and that a mechanical ventilator be used to assist breathing. Sometimes breathing can be assisted by a machine without inserting a breathing tube (called noninvasive ventilation). Higher-than-normal doses of several drugs are also needed.
Asthma control
Control is the degree to which symptoms, effects on daily life, and risks of severe asthma attacks are minimized by treatment. Asthma control is similar to severity, but it is assessed after treatment has started. The goal is for all people to have well-controlled asthma regardless of disease severity. Control is classified as
Well controlled: Symptoms occur twice per week or less often
Not well controlled: Symptoms occur more than twice per week but not every day
Very poorly controlled: Symptoms occur daily
Impairment
Impairment refers to the limitations symptoms place on daily life. Impairment due to asthma is determined by asking
How often symptoms are experienced
How often the person awakens at night
How often the person uses a short-acting beta-2 agonist for symptom relief
How often asthma interferes with normal activity
Other factors, such as measures of lung function, responses to standardized questionnaires, and what drugs are used to treat asthma, are also used to determine the severity, control, and impairment of asthma.
Risk
Risk refers to the likelihood of future asthma attacks, decreases in lung function, and side effects related to the drugs taken to control asthma. Doctors monitor risk with spirometry measurements (which measure lung function) over time as well as factors such as how often the person needs to receive certain oral corticosteroids or to be hospitalized to control asthma symptoms.
Diagnosis of Asthma
Breathing tests, including spirometry
Doctors suspect asthma based largely on a person’s report of characteristic symptoms. Doctors confirm the diagnosis by doing breathing tests (pulmonary function tests). The most important of these tests are measures of the amount of air a person can blow out in one second. These tests are done before and after giving the person an inhaled drug, called a beta-adrenergic drug (or beta-adrenergic agonist), that reverses airway narrowing. If test results are significantly better after the person receives the drug, asthma is thought to be present.
If the airways are not narrowed at the time of the test, a challenge test can help confirm the diagnosis. In a challenge test, pulmonary function is measured before and after the person inhales a chemical (usually methacholine, but histamine, If the airways are not narrowed at the time of the test, a challenge test can help confirm the diagnosis. In a challenge test, pulmonary function is measured before and after the person inhales a chemical (usually methacholine, but histamine,adenosine, or bradykinin may be used) that can narrow the airways. The chemical is given in doses that are too low to affect a person with healthy lungs but that cause the airways to narrow in a person with asthma.
Repeatedly measuring lung function over time allows doctors to determine the severity of the airway obstruction and the effectiveness of treatment.
To test for exercise-induced asthma, an examiner uses pulmonary function tests to measure how much air the person can exhale in 1 second before and after the person exercises on a treadmill or stationary bicycle. If the volume of air decreases more than 15%, the person’s asthma can be induced by exercise.
Pulmonary function tests may also be useful when a diagnosis of asthma is not clear and wheezing and shortness of breath may be due to another disorder such as an interstitial lung disease, chronic obstructive pulmonary disease, or upper airway obstruction.
A chest x-ray is usually not helpful in diagnosing asthma. Doctors use chest x-rays when considering another diagnosis. However, a chest x-ray is often obtained when a person with asthma needs to be hospitalized for a severe attack.
Identifying asthma triggers with allergy testing
Determining what triggers a person’s asthma is often difficult.
Allergy testing is appropriate when there is a suspicion that some avoidable substance (for example, exposure to cat dander) is provoking attacks. Skin testing can help identify allergens that may trigger asthma symptoms. However, an allergic response to a skin test does not necessarily mean that the allergen being tested is causing the asthma. The person still has to note whether attacks occur after exposure to this allergen. If doctors suspect a particular allergen, a blood test that measures the level of antibody produced in response to the allergen (the radioallergosorbent test [RAST]) can be done to determine the degree of the person's sensitivity to the allergen.
Evaluating an asthma attack
Because people who are having a severe asthma attack commonly have low blood oxygen levels, doctors may check the level of oxygen by using a sensing monitor on a finger or ear (oximetry). In severe attacks, doctors also need to measure levels of carbon dioxide in the blood, and this test typically requires obtaining a sample of blood from an artery or, occasionally, a vein. However, carbon dioxide levels can sometimes be monitored in the person's breath using a sensor placed in front of the nose or mouth.
Doctors may also check lung function, usually with a spirometer (a mouthpiece and tubing connected to a recording device that is used to measure air flow in the lungs) or with a peak flow meter. Usually, a chest x-ray is needed only when asthma attacks are severe, in order to rule out other serious conditions (such as a lung collapse).
Diagnosing asthma in older people
Older people are more likely to have other lung diseases that also cause shortness of breath (such as chronic obstructive pulmonary disease), so doctors have to determine how much of the person's breathing difficulty is related to asthma and reversible with the appropriate anti-asthma therapy. Often, in these people diagnosis involves a brief trial of drugs that are used to treat asthma to see whether the person's condition improves.
Treatment of Asthma
(See also Drugs for Preventing and Treating Asthma.)
Drugs to reduce inflammation
Drugs to widen the airways
An array of drugs can be used to prevent and treat asthma in adults or in children (see also Treatment of Asthma in Children). Doctors may use the term "rescue treatment" to describe treatment of an acute attack and "maintenance treatment" to describe treatments aimed at preventing attacks. Most of the drugs used to prevent asthma attacks are also used to treat an asthma attack but in higher doses or in different forms. Some people need to use more than one drug to prevent and treat their symptoms. The Drugs for Preventing and Treating Asthma are discussed in more detail elsewhere.
Therapy is based on two classes of drugs:
Anti-inflammatory drugs
Bronchodilators
Anti-inflammatory drugs suppress the inflammation that narrows the airways. Anti-inflammatory drugs include corticosteroids (which can be inhaled, taken by mouth, or given intravenously), leukotriene modifiers, and mast cell stabilizers.
Bronchodilators help to relax and widen (dilate) the airways. Bronchodilators include beta-adrenergic drugs (both those for quick relief of symptoms and those for long-term control), anticholinergics, and methylxanthines.
Immunomodulators, drugs that directly alter the immune system are sometimes used for people with severe asthma, but most people do not need immunomodulators. These drugs block substances in the body that cause inflammation.

Education about how to prevent and treat asthma attacks is beneficial for all people who have asthma and often for their family members. Proper use of inhalers is essential for effective treatment. People should know
What can trigger an attack
What helps to prevent an attack
How to use drugs properly
When to seek medical care
Monitoring Asthma at Home
Some people use a handheld peak flow meter to evaluate their breathing and determine when they need intervention, before their symptoms become severe. People who experience frequent, severe asthma attacks should know how to reach help quickly.
Peak expiratory flow (the fastest rate at which air can be pushed out of the lungs) can be measured using a small handheld device called a peak flow meter. This test can be used at home to monitor the severity of asthma. Usually, peak flow rates are lowest between 4 AM and 6 AM and highest at 4 PM. However, more than a 30% difference in rates at these times is considered evidence of moderate to severe asthma. People with moderate to severe asthma, particularly those who need daily treatment to control symptoms, often use a peak flow meter to take measurements and compare them to their personal best to help identify signs of worsening asthma or the onset of an asthma attack.
All people with asthma should have a written treatment action plan that was devised in collaboration with their doctor. Such a plan allows them to take control of their own treatment and has been shown to decrease the number of times people need to seek care for asthma in the emergency department.
Treating Asthma Attacks
An asthma attack can be frightening, both to the person experiencing it and to others around. Even when relatively mild, the symptoms provoke anxiety and alarm. A severe asthma attack is a life-threatening emergency that requires immediate, skilled, professional care. If not treated adequately and quickly, a severe asthma attack can cause death.
An acute attack in a person whose asthma has been controlled by drugs is called an exacerbation or flare-up.
Mild attacks
People who have a mild asthma attack are usually able to treat it without assistance from a health care practitioner. Typically, they use an inhaler to deliver a dose of a short-acting beta-adrenergic drug such as albuterol, move into fresh air (away from cigarette smoke or other irritants), and sit down and rest. They can use the inhaler 3 times 20 minutes apart if needed. An attack usually subsides in 5 to 10 minutes. An attack that does not subside after using an inhaler 3 times or that gets worse is likely to require additional treatment supervised by a doctor.People who have a mild asthma attack are usually able to treat it without assistance from a health care practitioner. Typically, they use an inhaler to deliver a dose of a short-acting beta-adrenergic drug such as albuterol, move into fresh air (away from cigarette smoke or other irritants), and sit down and rest. They can use the inhaler 3 times 20 minutes apart if needed. An attack usually subsides in 5 to 10 minutes. An attack that does not subside after using an inhaler 3 times or that gets worse is likely to require additional treatment supervised by a doctor.
Severe attacks
People who have severe symptoms should typically go to an emergency department. For severe attacks, doctors give frequent treatment using inhaled beta-adrenergic bronchodilator drugs delivered by a device called a nebulizer. Doctors sometimes give these bronchodilator drugs in combination with anticholinergic drugs. People are also given a corticosteroid, such as prednisone, by mouth or by vein (intravenously). Supplemental oxygen may be given during attacks. People who have severe symptoms should typically go to an emergency department. For severe attacks, doctors give frequent treatment using inhaled beta-adrenergic bronchodilator drugs delivered by a device called a nebulizer. Doctors sometimes give these bronchodilator drugs in combination with anticholinergic drugs. People are also given a corticosteroid, such as prednisone, by mouth or by vein (intravenously). Supplemental oxygen may be given during attacks.
Generally, people who have a severe asthma attack are admitted to the hospital if their lung function does not improve after they have received an inhaled beta-adrenergic drug and corticosteroids by mouth or vein. People also are hospitalized if they have a seriously low blood oxygen level or a high blood carbon dioxide level.
Antibiotics may be needed if a doctor suspects a bacterial lung infection. However, most such infections are due to viruses for which (with a few exceptions) no treatment exists.
People experiencing very severe asthma attacks may need to have an artificial airway passed through their mouth and throat (intubation) and be placed on a mechanical ventilator.
Preventing Asthma Attacks
Asthma is a chronic condition that cannot be cured, but individual attacks can often be prevented. Prevention efforts depend on the frequency of attacks and the stimuli that trigger the attacks.
Identifying and eliminating or avoiding stimuli that trigger asthma attacks may commonly prevent them.
Irritating fumes: People who have asthma should avoid cigarette smoke and other irritating fumes and try to avoid exposure to people with upper respiratory infections.
House dust mites: When dust and allergens are triggers, air filters and barriers (such as mattress covers, which reduce the amount of particles from dust mites that are in the air) can help considerably. Exposure to house dust mites can be reduced by removing wall-to-wall carpets and curtains and using air conditioning to keep the relative humidity low (preferably below 50%) in the summer.
Animal dander: Animals with fur or hair, most commonly cats and dogs, often must be given away to decrease the overall exposure to animal dander. Other measures that can help include limiting the family pet to certain rooms of the house or, if possible, keeping it out of the house. Washing the pet weekly can also help.
Drugs: Avoiding aspirin and NSAIDs helps prevent attacks in people whose asthma is triggered by these drugs. Drugs that block the beneficial effects of beta-adrenergic drugs (called beta-blockers) may worsen asthma. Tartrazine, a yellow coloring used in some drug tablets and food, may also bring on an attack.Avoiding aspirin and NSAIDs helps prevent attacks in people whose asthma is triggered by these drugs. Drugs that block the beneficial effects of beta-adrenergic drugs (called beta-blockers) may worsen asthma. Tartrazine, a yellow coloring used in some drug tablets and food, may also bring on an attack.
Exercise: Often, attacks triggered by exercise can be blocked by taking asthma drugs beforehand, but exercise should not be avoided.
Cold: For outdoor activity in cold weather, people with asthma can wear a ski mask or scarf that covers the nose and mouth to help keep the air being breathed in warm and moist.
Sulfites: Sulfites—commonly added to foods as a preservative—may trigger attacks after a susceptible person eats a certain food or drinks beer or red wine. Sulfites can be avoided by careful attention to diet choices.
Allergen desensitization through the use of allergy shots may help prevent attacks in people whose asthma is triggered by allergies. A doctor-supervised desensitization program may also be used for people whose asthma is triggered by aspirin or NSAIDs.through the use of allergy shots may help prevent attacks in people whose asthma is triggered by allergies. A doctor-supervised desensitization program may also be used for people whose asthma is triggered by aspirin or NSAIDs.
Drugs, such as inhaled or oral corticosteroids, leukotriene modifiers, long-acting beta-adrenergic drugs, methylxanthines, anticholinergics, or mast cell stabilizers are used to prevent attacks in most people with asthma. A minority of people with asthma have severe disease that remains uncontrolled, causing repeated attacks despite treatment with a combination of therapies. These people may benefit from treatment with immunomodulator drugs that block substances that cause allergic inflammation.
Prognosis for Asthma
Many children outgrow asthma, but wheezing may persist into adulthood or asthma may return in later years. Female sex, smoking, earlier age of onset, and allergy to household dust mites increase the risk that asthma will persist or return.
Although people may die as a result of a severe asthma attack, most of these deaths are preventable with treatment. Thus, the prognosis is good with adequate access and adherence to treatment.
More Information
The following are some English-language resources that may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Allergy and Asthma Network: What is asthma?: General information about asthma, including what causes it, how to avoid asthma attacks, and treatment
American Academy of Allergy, Asthma and Immunology: Asthma Overview: Overview of asthma symptoms and diagnosis, management and treatment
Asthma & Allergy Foundation of America: Asthma: General information about asthma, including triggers and suggestions for preventing asthma attacks







