





Cavities are decayed areas in the teeth, the result of a process that gradually dissolves a tooth’s hard outer surface (enamel) and progresses toward the interior.






(See also Overview of Tooth Disorders.)
Bacteria and debris build up on tooth surfaces, and the bacteria produce acids that cause decay.
Tooth pain occurs after decay reaches the inside of the tooth.
Dentists can detect cavities by examining the teeth and taking x-rays periodically.
Good oral hygiene and regular dental care plus a healthy diet can help prevent cavities.
Fluoride treatments can help surface cavities in the enamel heal, but for deeper cavities, dentists must drill out the decay and fill the resulting space.
Along with the common cold and gum disease, cavities (which are caused by bacteria) are among the most common human afflictions. If cavities are not properly treated by a dentist, they continue to enlarge. Ultimately, an untreated cavity can lead to tooth loss. Cavities in children can lead to premature loss of baby teeth, which causes shifts in neighboring teeth and may interfere with the eruption of permanent teeth.
Risk factors for cavities
There are many risk factors for cavities:
Inadequate control of plaque and tartar
Defects in the tooth surface
Frequent intake of sugary and/or highly acidic foods and liquids
Too little oral fluoride intake
Reduced saliva flow (for example, due to certain medications, radiation therapy for cancer, or systemic disorders that cause salivary gland dysfunction)
Genetic factors
Plaque is a filmlike substance composed of bacteria, saliva, food debris, and dead cells that is continually being deposited on teeth.
Tartar, scientifically known as 'calculus, ' is hardened plaque. It may be white but is more often yellow and forms at the base of teeth.
For tooth decay to develop, a tooth must be susceptible, acid-producing bacteria must be present, and nutrients (such as sugar) must be available for the bacteria to thrive and produce acid. A susceptible tooth has relatively little protective fluoride incorporated into the enamel or has pronounced pits, grooves, or cracks (fissures) that retain plaque. Poor oral hygiene that allows plaque and tartar to accumulate can accelerate this process. Although the mouth contains large numbers of bacteria, only certain strains generate acid, which causes decay.
Spotlight on Aging: Tooth Loss
Only a generation ago, most people expected to go through old age with false teeth or no teeth at all. This expectation has changed greatly during the last several decades in most countries with available dental access. Although nearly half of people 85 or older have none of their natural teeth, the likelihood of losing teeth with aging is steadily decreasing. There are several reasons for this change: improved nutrition, better access to dental care, and better treatment for tooth decay and periodontal disease. When teeth are lost, chewing is greatly hindered, and speaking becomes a challenge. The face looks dramatically different without the support teeth normally provide for the lips, cheeks, nose, and chin. People who have lost some or all of their teeth can still eat, but they tend to eat soft foods. Soft foods tend to be relatively high in carbohydrates and low in protein, vitamins, and minerals. Foods that are high in protein, vitamins, and minerals, such as meats, poultry, grains, and fresh fruits and vegetables, tend to be harder to chew. Consequently, older adults who eat mainly soft foods may become undernourished. |
The nutrients that decay-causing bacteria need come from the person’s diet. When infants are put to bed with a bottle that contains anything but plain water, their teeth have prolonged contact with the formula, milk, or juice, which increases the likelihood of decay. Large amounts of sugar in the diet also provide food for the bacteria.
Acid in the diet accelerates tooth decay. (For example, soft drinks, sports drinks, and energy drinks, all of which are commonly acidic, tend to promote tooth decay.)
Reduced saliva flow due to medications or disorders (such as Sjögren syndrome) places people at greater risk of tooth decay. Older adults often take medications that reduce saliva flow, increasing their risk of cavities.
Some people have especially active decay-causing bacteria in their mouth. A parent may pass these bacteria to a child through kissing, sampling the child's food, or sharing eating utensils. The bacteria flourish in the child’s mouth after the first teeth come in and can then cause cavities. So, a tendency toward tooth decay that runs in families does not necessarily reflect poor oral hygiene or bad eating habits. These bacteria can also be spread (rarely) through social contact with people outside the family.
Gum recession also makes cavities more likely to develop because it can expose the roots of teeth, which are not protected by an outer enamel layer. Then bacteria can access the inner layers of the tooth more easily. Gum recession and a reduction in salivary flow make older adults prone to root cavities.
Progression of tooth decay
Decay in the enamel progresses slowly. After penetrating into the second layer of the tooth—the somewhat softer, less resistant dentin—decay spreads more rapidly and moves toward the pulp, the innermost part of the tooth, which contains the nerves and blood supply. Although a cavity may take 2 or 3 years to penetrate the enamel, it can travel from the dentin to the pulp—a much greater distance—in as little as a year. Thus, root decay that starts in the dentin can destroy a lot of tooth structure in a short time.
Types of Cavities
The illustration on the left shows a tooth with no cavities. The illustration on the right shows a tooth with the 3 types of cavities. |

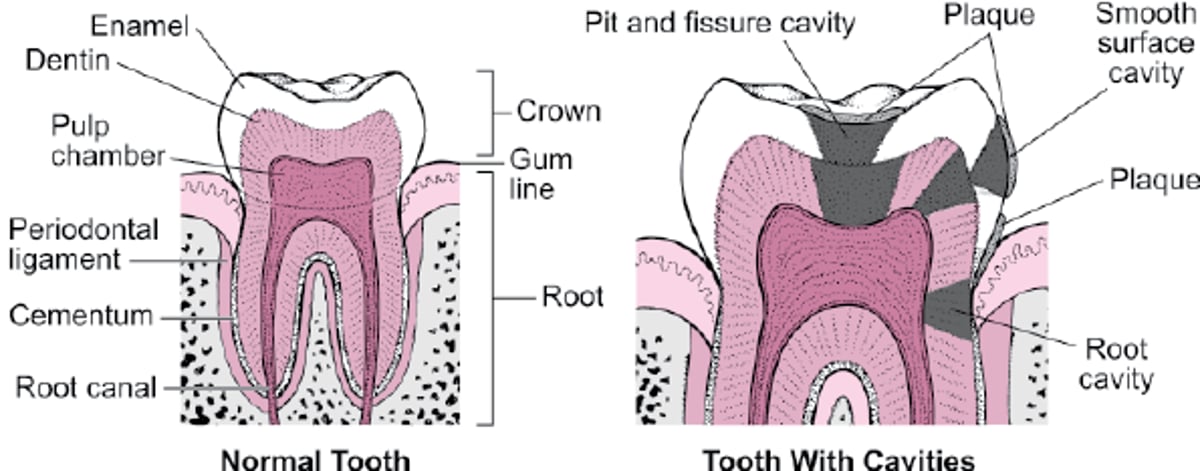
Smooth surface decay, the most preventable and reversible type, grows the slowest. In smooth surface decay, a cavity begins as a white spot where bacteria dissolve the calcium of the enamel. Smooth surface decay between the permanent teeth usually begins between the ages of 20 and 30.
Pit and fissure decay, which usually starts during the teen years in the permanent teeth, forms in the narrow grooves on the chewing surface and on the cheek side of the back teeth. Decay at these locations progresses rapidly. Many people cannot adequately clean these cavity-prone areas because the grooves are narrower than the bristles of a toothbrush.
Root decay begins on the root surface covering (cementum) that has been exposed by receding gums, usually in people past middle age. This type of decay often results from difficulty cleaning the root areas, a lack of adequate saliva flow, a diet high in sugar, or a combination of these factors. Root decay can be the most difficult type of tooth decay to prevent and treat.
Did You Know...
|
Symptoms of Cavities
Whether tooth decay causes pain depends on which part of the tooth is affected and how deeply the decay extends. A cavity in the enamel causes no pain. The pain starts when the decay reaches the dentin. At first, people may feel pain only when hot, cold, or sweet foods or beverages come in contact with the affected tooth. This type of pain often indicates that the inflammation in the pulp is reversible. If the cavity is treated at this stage, dentists can restore the tooth, and most likely no further pain or chewing difficulties will develop.
A cavity that gets close to or actually reaches the pulp causes irreversible damage. Pain lingers even after a stimulus (such as cold water) is removed. The tooth may hurt even without stimulation (spontaneous toothache).


Image provided by Jonathan A. Ship, DMD.
If irreversible damage to the pulp occurs and the pulp subsequently dies, the pain may stop temporarily. The tooth then may become sensitive when people bite or when the tongue or a finger presses on it because the area at the end of the root has become inflamed or because infection has developed at the root. Infection may produce a collection of pus (periapical abscess), which causes constant pain that is worse when people bite.
Diagnosis of Cavities
A dentist's evaluation
Regular dental x-rays
Sometimes special testing instruments
If a cavity is treated before it starts to hurt, the chance of damage to the pulp is reduced, and more of the tooth structure is saved. To detect cavities early, a dentist inquires about pain, examines the teeth, probes the teeth with dental instruments, and may take x-rays. Some dentists also use special dyes, fiberoptic lights, and/or new devices that detect cavities by changes in electrical conductivity or laser reflectivity.
People should have a dental examination every 3 to 12 months, depending on their susceptibility to cavities and their dentist's recommendations. Not every examination includes x-rays, but x-rays are still important for detecting cavities (even those under existing restorations) and determining the depth of those cavities. The dentist’s assessment of a person’s teeth will determine how often x-rays should be taken. (They are taken less frequently in people with a low risk for new cavities.)
Did You Know...
|
Treatment of Cavities
Fluoride
Fillings
Root canal or tooth extraction
If decay is halted before the enamel surface breaks down, the enamel can actually repair itself (remineralization) if people use fluoride. Fluoride treatment requires use of prescription-strength toothpastes containing a higher concentration of sodium fluoride and many applications of sodium fluoride at the dentist's office. Products containing calcium and phosphates can also be applied to the teeth, but they are less effective in remineralizing teeth than fluoride. Silver diamine fluoride (SDF) can stop the development of cavities and remineralize affected teeth. However, because SDF permanently stains caries black, it is applied primarily to baby teeth. If decay is halted before the enamel surface breaks down, the enamel can actually repair itself (remineralization) if people use fluoride. Fluoride treatment requires use of prescription-strength toothpastes containing a higher concentration of sodium fluoride and many applications of sodium fluoride at the dentist's office. Products containing calcium and phosphates can also be applied to the teeth, but they are less effective in remineralizing teeth than fluoride. Silver diamine fluoride (SDF) can stop the development of cavities and remineralize affected teeth. However, because SDF permanently stains caries black, it is applied primarily to baby teeth.
Once decay reaches the dentin and causes an actual hole in the tooth, dentists drill out the decayed material inside the tooth and then fill the resulting space with a filling (restoration). Treating the decay at an early stage helps maintain the strength of the tooth and limits the chance of damage to the pulp.
Fillings
Fillings are made of various materials and may be put inside the tooth or around it. The choice of filling varies depending on the location and size of the cavity.
Silver amalgam (a combination of silver, mercury, copper, tin, and occasionally, zinc, palladium, or indium) is most commonly used for fillings in back teeth, where strength is important and the silver color is relatively inconspicuous. Silver amalgam is relatively inexpensive and lasts an average of 14 years. However, the amalgam can last for more than 40 years if it is carefully placed using a rubber dam and the person’s oral hygiene is good.
Overall, amalgam fillings last longer and are more resistant to additional cavities than composite resins. Even so, amalgam use is decreasing for several reasons:
Their cosmetic results are not as pleasing as those achieved with composite resins or glass ionomers.
Composite resins are more durable than they used to be.
Dental schools now routinely teach about the alternatives to amalgam fillings.
Environmental concerns about the removal and disposal of the mercury content of amalgam are now more commonly taken into consideration.
It is important to note that blood mercury levels do not correlate with the number of amalgam fillings a person has, so concerns of "mercury poisoning" may be overblown. The very tiny amount of mercury that escapes from silver amalgam is too small to affect health. Dentists do not recommend replacing amalgam because the procedure is expensive, damages tooth structure, actually increases a person's exposure to mercury, and requires the use of amalgam separators to prevent release of its mercury content into the environment.
Gold fillings (inlays and onlays) are excellent but are more expensive. Also, at least 2 dental visits are required to permanently place them.
Composite resins are used typically in the front teeth, where silver would be conspicuous. Increasingly, these fillings are also being used in back teeth. Although they have the advantage of being the color of the teeth and they allow dentists to conserve more of the tooth structure than amalgam fillings do, composite resins are more expensive than silver amalgam and possibly more likely to develop decay around the margins. This is because the composite resin shrinks when it hardens. Composite resins also may not last as long as silver amalgam, particularly in the back teeth, which take the full force of chewing. Improvements in composite resins have limited some of the shrinkage that occurred with some earlier versions of the material.
Reinforced glass ionomer, a tooth-colored filling, is formulated to release fluoride once in place, a benefit for people especially prone to tooth decay. Glass ionomer is also used to restore areas damaged by overzealous brushing. Resin-modified glass ionomer materials are also available and provide better cosmetic results than conventional glass ionomers.
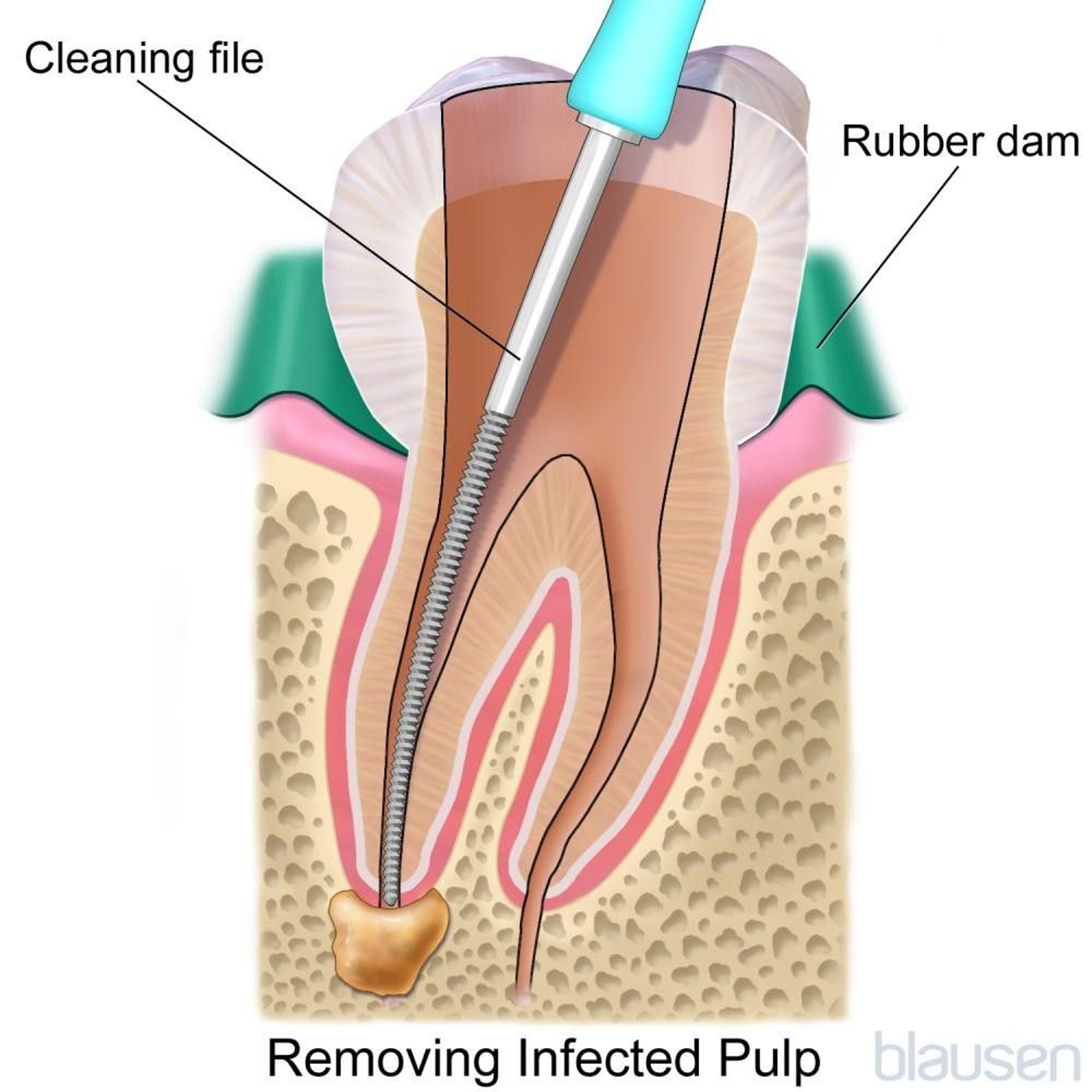
Root canal treatment and tooth extraction
When tooth decay advances far enough to permanently harm the pulp, the only way to eliminate pain is to remove the pulp by root canal (endodontic) treatment or tooth removal (extraction).
The tooth is numbed (anesthetized), and a rubber dam is placed around the tooth to isolate it from bacteria in the rest of the mouth. A hole is then drilled through the chewing surface of a back tooth or the tongue side of a front tooth.
Next, the canal is cleaned and tapered from the opening to the end of the root. Fine instruments are passed through the hole into the pulp canal space, and all the remaining pulp is removed. The canal is then sealed with a flexible material (gutta percha) that hardens over time.



If a tooth is extracted, it should be evaluated for replacement as soon as possible. Otherwise, neighboring or opposing teeth may change position and alter the person’s bite. There are many options for replacement of extracted teeth (see Dental Appliances).
Prevention of Cavities
Several general strategies are key to preventing cavities:


Good oral hygiene and regular dental care
Healthy diet
Fluoride (in water, toothpaste, or both)
Sometimes fluoride, treatments sealants, and antibacterial therapy
Oral hygiene
Good oral hygiene, which involves brushing before or after breakfast and before bedtime and flossing daily to remove plaque, can effectively control smooth surface decay. Brushing helps prevent cavities from forming on the top and sides of the teeth, and flossing gets between the teeth where a brush cannot reach.
Electric and ultrasonic toothbrushes are excellent, but an ordinary toothbrush, used properly, is quite sufficient. Normally, proper brushing takes only about 3 to 4 minutes. People should avoid using too much toothpaste, especially abrasive types, which may erode the teeth (particularly if brushing occurs immediately after exposure to acidic drinks). Floss is gently moved between the teeth, then wrapped around the tooth and root surfaces in a “C” shape at the gum line. When the floss is moved up and down 3 times, it can remove plaque and food debris. There are many small, toothpick-like devices (called interproximal brushes) with bristles or plastic projections on the ends that can be used to clean between teeth. These devices are effective but can be used only if there is enough space between the teeth to accommodate them. They come in many sizes and shapes and can be used alone or with different toothpastes or rinses. Water-flossing devices may prove helpful for people who have difficulty manipulating dental floss. These types of devices are considered an adjunct, not a replacement for conventional dental floss.
Initially, plaque is quite soft, and removing it with a soft-bristled toothbrush and dental floss at least once every 24 hours makes decay unlikely. Once plaque begins to harden, a process that begins after approximately 72 hours, removing it becomes more difficult.
Diet
Although all carbohydrates can cause tooth decay to some degree, the biggest culprits are sugars. All simple sugars, including table sugar (sucrose) and the sugars in honey (levulose and dextrose), fruit (fructose), and milk (lactose), have the same effect on the teeth. Whenever sugar comes in contact with plaque, Streptococcus mutans bacteria in the plaque produce acid. The amount of sugar eaten is less important than how often people eat sugar because what matters is the amount of time sugar is in contact with the teeth. Thus, sipping a sugary soft drink over an hour is more damaging than eating a candy bar in 5 minutes, even though the candy bar may contain more sugar. Infants who go to bed with a bottle, even if it contains only milk or formula, are also at risk of cavities. Bedtime bottles should contain only water.
People who tend to develop cavities should eat sweet snacks less often. Rinsing the mouth with water after eating a snack removes some of the sugar, but brushing the teeth is more effective. Drinking artificially sweetened soft drinks also helps, although diet colas contain acid that can promote tooth decay. Drinking tea or coffee without sugar also can help people avoid cavities, particularly on exposed root surfaces.
Fluoride
Fluoride can make the teeth, particularly the enamel, more resistant to the acid that helps cause cavities. Fluoride taken internally is effective while the teeth are growing and hardening. Water fluoridation is the most efficient way to supply children with fluoride, and over half of the population of the United States now has drinking water that contains fluoride. However, many people may not consume enough of this water to significantly reduce tooth decay. Conversely, if a water supply has too much fluoride, the teeth can become spotted or discolored (fluorosis). The discoloration may range from mild to severe.
If a child’s water supply does not have enough fluoride, doctors or dentists can prescribe sodium fluoride in drops, gels, toothpastes, or tablets. Tablets should be chewed or allowed to dissolve in the mouth before swallowing. Children begin taking the drops or tablets at about 6 months and can take them through age 16. For people of any age who are prone to tooth decay, dentists may apply fluoride directly to the teeth or have them wear, at night, a custom-made mouth guard that holds fluoride. If a child’s water supply does not have enough fluoride, doctors or dentists can prescribe sodium fluoride in drops, gels, toothpastes, or tablets. Tablets should be chewed or allowed to dissolve in the mouth before swallowing. Children begin taking the drops or tablets at about 6 months and can take them through age 16. For people of any age who are prone to tooth decay, dentists may apply fluoride directly to the teeth or have them wear, at night, a custom-made mouth guard that holds fluoride.
Fluoridated toothpaste is beneficial for adults as well as children. Because young children may swallow toothpaste when brushing, they are prone to fluorosis (the development of white or brown spots on the teeth from too much fluoride). To prevent this problem, they should use children's toothpastes, which contain lower amounts of fluoride.
Sealants
Dentists sometimes apply sealants to protect hard-to-reach pits and fissures, particularly on the back teeth. After thoroughly cleaning the area to be sealed, dentists roughen the enamel with an acid solution to help the sealant adhere to the teeth. Dentists then place a liquid plastic in and over the pits and fissures of the teeth. When the liquid hardens, it forms such an effective barrier that any bacteria inside a pit or fissure stop producing acid because food can no longer reach them. About 90% of the sealant remains after 1 year and 60% remains after 10 years. The occasional need for repair or replacement of sealants can be assessed at periodic dental examinations.
Antibacterial therapy
People who are very prone to tooth decay may need antibacterial therapy. Dentists first remove cavities and seal all pits and fissures in the teeth. Then dentists may prescribe a powerful antiseptic mouth rinse (chlorhexidine) that is used for 2 weeks to kill off the cavity-causing bacteria that remain in plaque. A long-acting form of chlorhexidine can also be applied by a dentist. The hope is that less harmful bacteria will replace the cavity-causing bacteria. However, the effectiveness of chlorhexidine in preventing caries in adults is inconsistent. Another way to keep bacteria under control is to have people who are prone to cavities chew gum or hard candy containing People who are very prone to tooth decay may need antibacterial therapy. Dentists first remove cavities and seal all pits and fissures in the teeth. Then dentists may prescribe a powerful antiseptic mouth rinse (chlorhexidine) that is used for 2 weeks to kill off the cavity-causing bacteria that remain in plaque. A long-acting form of chlorhexidine can also be applied by a dentist. The hope is that less harmful bacteria will replace the cavity-causing bacteria. However, the effectiveness of chlorhexidine in preventing caries in adults is inconsistent. Another way to keep bacteria under control is to have people who are prone to cavities chew gum or hard candy containingxylitol (a sweetener that inhibits the cavity-causing bacteria in plaque).
Antibacterial therapy can be used by pregnant women who have a history of severe cavities. Pregnant women who cannot tolerate antibacterial therapy can use xylitol as mentioned above. Xylitol is used from the time the child is born until the age at which the mother no longer samples the child’s food. Xylitol may help prevent the mother's bacteria from being passed to the child.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Mouth Healthy: This general resource provides information on oral health, including nutrition and guidance on selecting products that carry the American Dental Association's seal of approval. There is also advice on finding a dentist and how and when to see one.







