

Placenta previa is attachment (implantation) of the placenta over the opening of the cervix, in the lower rather than the upper part of the uterus.
Women may have painless, sometimes profuse bleeding late in the pregnancy.
Ultrasonography can usually confirm the diagnosis.
Modified activity may be all that is needed, but if bleeding is severe and continues or if the fetus or woman develop problems, cesarean delivery is done.
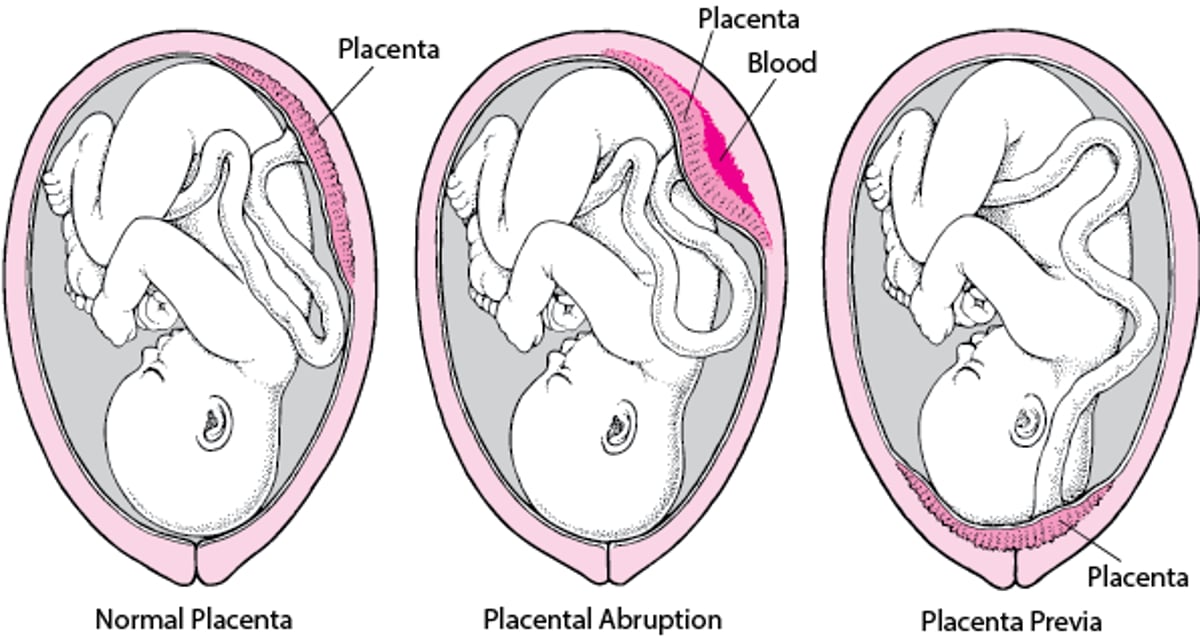
Normally, the placenta is located in the upper part of the uterus. In placenta previa, the placenta is located in the lower part. It covers the opening of the cervix—the entrance to the birth canal. Sometimes the placenta is located near the opening of the cervix, not over it (called a low-lying placenta).
Placenta previa occurs in about 1 of 800 deliveries. During the second trimester, as many as 2% of pregnant women have placenta previa. Placenta previa may be visible on ultrasonography. However, it resolves on its own in more than 90% of women before they deliver. If it does not resolve, the placenta may detach from the uterus, depriving the baby of its blood supply. Passage of the baby through the birth canal can also tear the placenta, causing severe bleeding.
Risk factors (conditions that increase the risk of a disorder) for placenta previa include the following:
Having had more than one pregnancy
Having had a cesarean delivery
Having a structural abnormality of the uterus, such as fibroids
Having had a procedure that involves the uterus such as removal of fibroids from the uterus (myomectomy) or dilation and curettage (D and C) done several times
Smoking
Being pregnant with twins, triplets, or more babies (multiple births)
Being older
Symptoms of Placenta Previa
Placenta previa often does not cause symptoms, and doctors discover it during a routine second-trimester ultrasound.
Placenta previa can cause painless bleeding from the vagina that starts suddenly. The blood may be bright red. Bleeding may become profuse, endangering the life of the woman and the fetus. Some women also have contractions.
Placenta previa can cause problems for the fetus, such as the following:
The fetus may be in an abnormal position.
The fetus may not grow as much as expected (intrauterine growth restriction).
Blood vessels connecting the umbilical cord and placenta may block the fetus's exit through the opening of the cervix (vasa previa).
If women previously had placenta previa with a cesarean delivery, the risk that the placenta will be too firmly attached to the uterus (placenta accreta) increases. Placenta accreta belongs to a group of disorders called the placenta accreta spectrum. These disorders differ in how firmly the placenta is attached to the uterus.
Diagnosis of Placenta Previa
Ultrasonography
Doctors suspect placenta previa in pregnant women with vaginal bleeding that starts during the second or third trimester of pregnancy. Ultrasonography helps doctors identify placenta previa and distinguish it from a placenta that has detached too early (placental abruption).
If women have vaginal bleeding and placenta previa is thought to be the cause, doctors monitor the fetus's heart rate to determine whether the fetus is having problems, such as not getting enough oxygen.
Problems With the Placenta
Normally, the placenta is located in the upper part of the uterus, firmly attached to the uterine wall until after delivery of the baby. The placenta carries oxygen and nutrients from the mother to the fetus. In placental abruption (abruptio placentae), the placenta detaches from the uterine wall earlier than it should, causing the uterus to bleed and reducing the fetus’s supply of oxygen and nutrients. Women who have this complication are hospitalized, and the baby may be delivered early. In placenta previa, the placenta is located over the cervix, in the lower part of the uterus. Placenta previa may cause painless bleeding that suddenly begins after 20 weeks of pregnancy. The bleeding may become profuse. The baby is usually delivered by cesarean. |

Treatment of Placenta Previa
Hospitalization and modified activity
Delivery at 36 to 37 weeks if bleeding has stopped
Immediate cesarean delivery if the woman or fetus is having problems
When bleeding is minor and occurs before about 36 weeks of pregnancy, doctors typically advise that the woman be admitted to the hospital and told to limit her activity until the bleeding stops. Limiting her activity (called modified activity or modified bed rest) means that she should stay off her feet for most of the day. If the bleeding stops, the woman may be allowed to gradually resume light activities. If bleeding does not recur, she is usually sent home, provided that she can return to the hospital easily. Doctors advise against sexual activity, which can trigger bleeding.
If bleeding recurs, the woman is usually readmitted to the hospital and may be kept there until delivery.
Some experts recommend giving corticosteroids to the mother to help the fetus's lungs mature if early delivery—usually before about 34 weeks of pregnancy—may become necessary.
If the woman is not having contractions and if bleeding has stopped, doctors may deliver the baby at 36 to 37 weeks of pregnancy.
Delivery is usually done immediately when one of the following occur:
Bleeding is profuse or does not stop.
The fetus's heart rate is abnormal.
The woman's blood pressure becomes too low.
In women with placenta previa, delivery is cesarean, done before labor starts. Vaginal delivery may be possible for women with a low-lying placenta.
Women who bleed profusely may need blood transfusions.
Women with Rh-negative blood are given Rho(D) immune globulin to prevent hemolytic disease of the fetus (erythroblastosis fetalis). This disorder occurs when a pregnant woman has Rh-negative blood and the fetus has Rh-positive blood.





