











Contraceptive hormones can be
Taken by mouth (oral contraceptives)
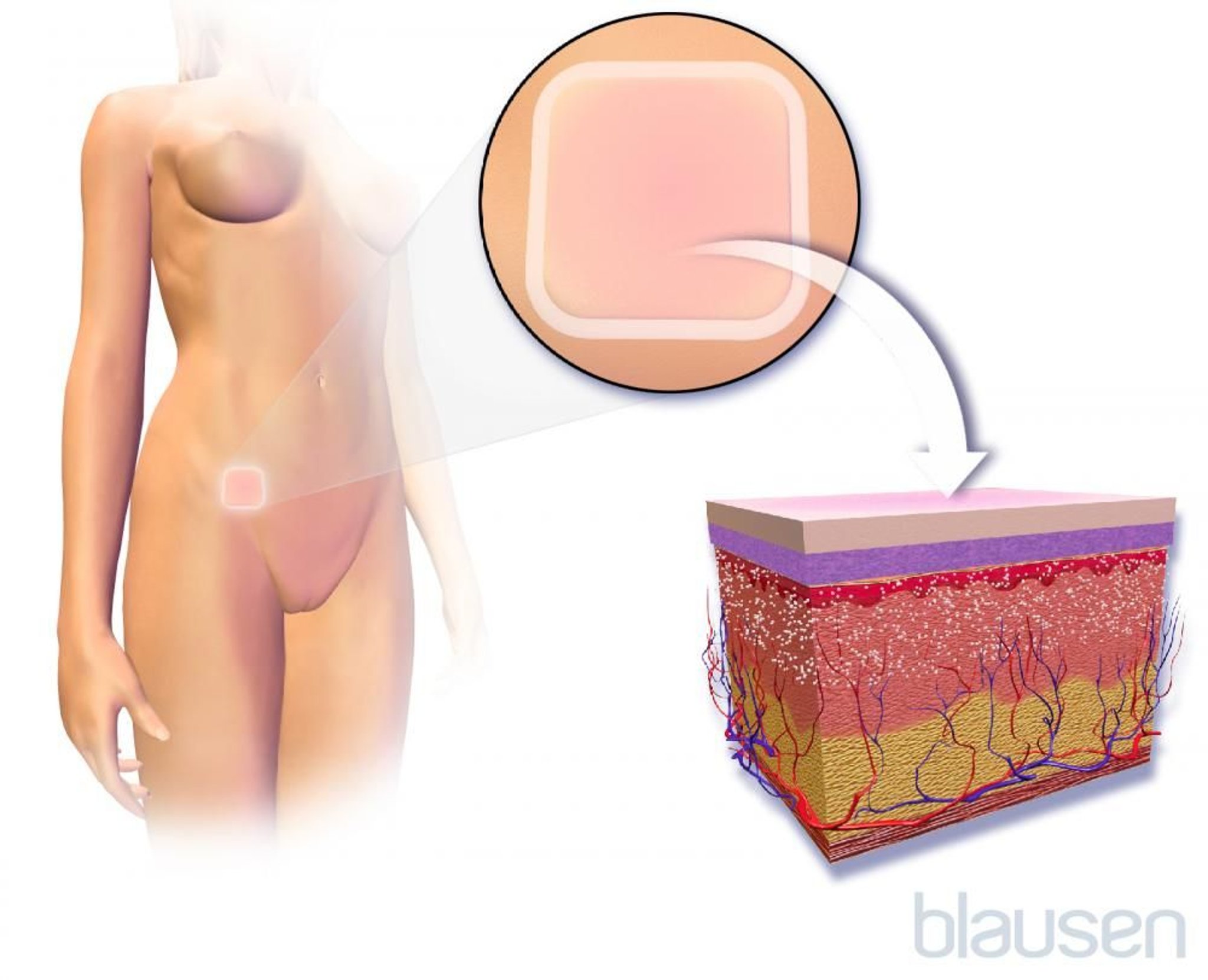
Inserted into the vagina (vaginal rings)
Applied to the skin (patch)
Implanted under the skin
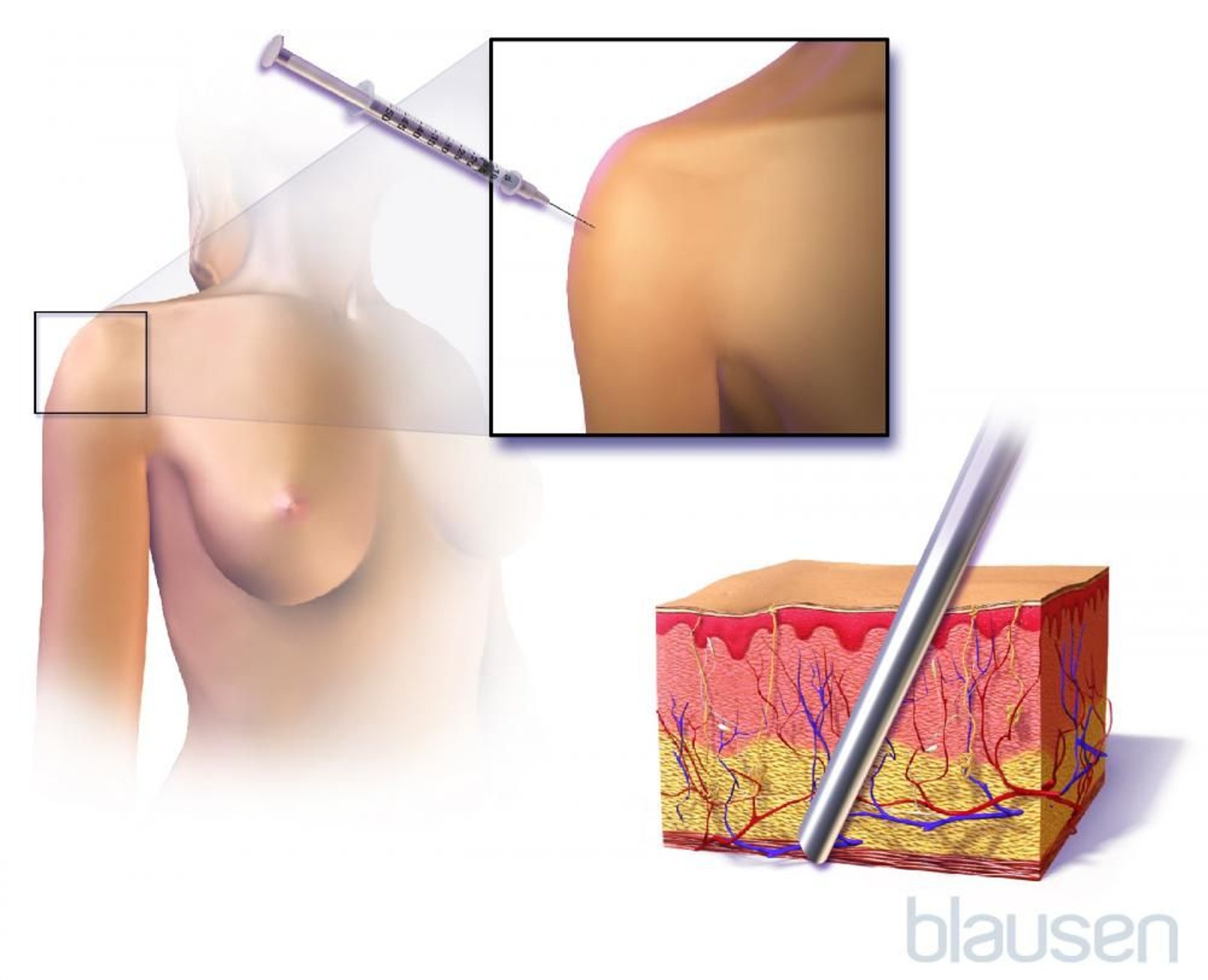
Injected into muscle
The hormones used to prevent conception include estrogen and progestins (medications similar to the hormone progesterone). Estrogen and progestins are the main hormones involved in the menstrual cycle. Hormonal methods prevent pregnancy mainly by stopping the ovaries from releasing eggs (ovulation) or by keeping mucus in the cervix thick so that sperm cannot pass through the cervix into the uterus. Thus, hormonal methods prevent the egg from being fertilized.
All hormonal methods can have similar side effects and restrictions on use.
Oral Contraceptives
Oral contraceptives, commonly known as birth control pills or just “the pill,” contain hormones—either a combination of estrogen and a progestin or a progestin alone.


Combination pills (pills that contain both estrogen and progestin) are typically taken once a day for 21 to 24 days, not taken for 4 to 7 days (allowing the menstrual period to occur), then started again. Inactive (placebo) pills are usually taken for the days when combination pills are not taken to establish a routine of taking one pill a day. The inactive pill may contain iron and folate. Iron is included to help prevent or treat iron deficiency because iron is lost in menstrual blood each month. Folate is included in case women, who may unknowingly have a folate deficiency, become pregnant. Folate deficiency in a pregnant woman increases the risk of birth defects such as spina bifida.
Sometimes combined estrogen-progestin contraceptive pills are taken daily for 12 weeks, then not taken for 1 week. Thus, menstrual periods occur only 4 times a year. Or they are taken as an active pill every day. With this type, there is no scheduled bleeding (no menstrual periods), but irregular bleeding is more likely to occur.
About 0.3% of women who take combination pills as instructed become pregnant during the first year of use. However, the chances of becoming pregnant increase substantially if women skip a pill, especially the first ones in a monthly cycle. With typical use (the way most people use them), about 9% of women become pregnant during the first year of use.
The dose of estrogen in combination pills varies. In combination pills, the estrogen dose ranges from 10 to 35 micrograms. Healthy women who do not smoke can take low-dose combination pills until menopause.
If women miss taking a combination pill one day, they should take two pills the next day. If they forget to take a pill for 2 days, they should resume taking one pill each day and should use a backup contraceptive method for the next 7 days. If women forget to take a pill for 2 days and have had unprotected intercourse in the 5 days before those 2 days, they can consider emergency contraception.
Women with current breast cancer should not use combined estrogen-progestin pills, patches, or rings.
Progestin-only pills are taken every day of the month, and it is important to take this type of contraceptive pill at the same time of day. They often cause irregular bleeding. Pregnancy rates with these pills and with combination pills are similar, if used as instructed. Progestin-only pills are usually prescribed only for women who should not take estrogen. For example, progestin-only pills may be used by women who have migraines with an aura (symptoms that occur before the headache), high blood pressure, or severe diabetes (see Conditions That Prohibit the Use of Combination Oral Contraceptives) and, therefore, should not take estrogen. If more than 27 hours go by between taking progestin-only pills, women should use a backup contraceptive method for the next 7 days in addition to taking the progestin-only pill each day. Women with current breast cancer should not take progestin-only pills, implants, or injections.
Starting oral contraceptives
Before starting oral contraceptives, a woman must see a doctor. Doctors ask the woman about her medical, social, and family history to determine whether she has any health problems that would make taking these contraceptives risky for her. They measure her blood pressure. If it is high, combination oral contraceptives (estrogen plus a progestin) should not be prescribed. A pregnancy test may be done to rule out pregnancy. Doctors also often do a physical examination, although this examination is not necessary before a woman starts taking oral contraceptives. Three months after starting oral contraceptives, the woman should have another examination to determine whether her blood pressure has changed. If it has not, she should then have an examination once a year. Oral contraceptives can be prescribed for 13 months at a time.
Women can start taking oral contraceptives at any time of month. However, if they start taking them more than 5 days after the first day of their period, they should use a backup contraceptive method for the next 7 days in addition to taking the oral contraceptive.
When women can start taking combination oral contraceptives after pregnancy varies:
After a miscarriage or an abortion during the 1st trimester of pregnancy: Start immediately
After a miscarriage, delivery, or an abortion during the 2nd trimester: Start within 1 week if they have no other risk factors for developing blood clots (such as smoking, diabetes, or high blood pressure)
For a delivery after 28 weeks: Wait 21 days (wait 42 days if women are breastfeeding or have risk factors for blood clots, including cesarean delivery)
Women with risk factors for blood clots should wait because blood clots are more likely to develop during pregnancy and after delivery. Taking combination oral contraceptives also makes blood clots more likely to develop.
Progestin-only oral contraceptives may be taken immediately after the delivery of a baby.
In most women who have recently given birth and are exclusively breastfeeding and who have not had a menstrual period, pregnancy is unlikely to occur for 6 months after the baby is delivered, even when no contraception is used. However, starting to use contraception within 3 months after delivery is recommended if bottle feeding has started or there are any interruptions in breastfeeding.
If a woman has coronary artery disease or diabetes or has risk factors for them (such as a close relative with either disorder), a blood test is usually done to measure levels of cholesterol, other fats (lipids), and sugar (glucose) before a combination contraceptive is prescribed. Even if these levels are abnormal, doctors may still prescribe a low-dose estrogen combination contraceptive. However, they periodically do blood tests to monitor the woman’s lipid and sugar levels. Women with diabetes can usually take combination oral contraceptives unless diabetes has damaged blood vessels or they have had diabetes for more than 20 years.
If a person has had a liver disorder, doctors do tests to evaluate how well the liver is functioning. If results are normal, oral contraceptives may be taken.
Also before starting oral contraceptives, a woman should talk with her doctor about the advantages and disadvantages of oral contraceptives for her situation.
Advantages
The main advantage of oral contraceptives (birth control pills) is reliable, continuous contraception if the pills are taken as instructed.
Also, taking oral contraceptives reduces the occurrence of the following:
Premenstrual dysphoric disorder (the severe form of premenstrual syndrome)
Abnormal uterine bleeding due to ovulatory dysfunction (abnormal bleeding that results from changes in the hormonal control of menstruation)
Infections of the fallopian tubes
Cancer of the uterus (endometrial cancer)
The risk of developing cancer of the uterus and cancer of the ovaries is reduced for at least 20 years after the contraceptives are stopped. Oral contraceptives reduce the risk of cancer of the uterus by 60% after at least 10 years of use and cancer of the ovaries by about 50% after taking them for 5 years and by 80% after taking them for 10 years or more.
Oral contraceptives taken early in a pregnancy do not harm the fetus. However, they should be stopped as soon as the woman realizes she is pregnant. Oral contraceptives do not have any long-term effects on fertility, although a woman may not release an egg (ovulate) for a few months after stopping the medications.
Did You Know...
|
Disadvantages
Although oral contraceptives may have some side effects, the overall risk of these effects is small. Bloating, breast tenderness, nausea, and headache are the most common side effects.
Progestin-only pills often cause irregular vaginal bleeding.
Breakthrough bleeding and missing periods (amenorrhea) is common during the first few months of combination oral contraceptive use, particularly if women forget to take the pills, but it usually stops as the body adjusts to the hormones. Breakthrough bleeding is bleeding that occurs between periods, when women are taking the active pill. Doctors may increase the dose of estrogen to manage both breakthrough bleeding and amenorrhea.
Some side effects are related to the estrogen in the pill. They may include nausea, bloating, fluid retention, an increase in blood pressure, breast tenderness, and migraine headaches. Others, such as acne and changes in appetite and mood, are related mostly to the type or dose of the progestin. Some women who take oral contraceptives gain 3 to 5 pounds because they retain fluid or because appetite increases. Many of these side effects are uncommon with the low-dose pills.
Oral contraceptives can also cause vomiting, headaches, depression, and problems sleeping.
In some women, oral contraceptives cause dark patches (melasma) on the face, similar to those that may occur during pregnancy. Exposure to the sun darkens the patches even more. If dark patches develop, doctors usually stop the oral contraceptives. The patches slowly fade after the contraceptives are stopped.
Taking oral contraceptives increases the risk of developing some disorders.
The risk of developing blood clots in veins may be 2 to 4 times higher for women who are taking combination oral contraceptives than it was before they started taking the contraceptives. If women have a disorder that causes blood clots or have family members who have had blood clots, further evaluation is needed. These women may not be able take oral contraceptives that contain estrogen. If a woman who is taking oral contraceptives develops swelling in one leg, chest pain, or shortness of breath, they should see a doctor immediately. If doctors suspect that a woman taking oral contraceptives has deep vein thrombosis (a blood clot, usually in the leg) or pulmonary embolism (a blood clot in the lungs), the contraceptives are stopped immediately. Tests are then done to confirm or rule out the diagnosis.
Surgery increases the risk of blood clots, so women should stop taking oral contraceptives before a surgical procedure. They should ask their doctor when to stop and restart the contraceptive pills. Limited movement (immobility) due to an injury or travel also increases the risk of blood clots. Thus, if a woman's movements are limited, she may need to try to move around as much as possible or take other measures to prevent blood clots from developing. For example, women can elevate their legs, flex and extend their ankles about 10 times every 30 minutes, and/or walk and stretch every 2 hours while traveling.
Cervical cancer is slightly more likely to develop in women who use oral contraceptives for more than 5 years. But 10 years after stopping use, this risk decreases to what it was before starting oral contraceptives. Also, whether the increased risk is related to the oral contraceptives is unclear. Women who are taking oral contraceptives should have Papanicolaou (Pap) tests as recommended by their doctor. Such tests can detect precancerous changes in the cervix early—before they lead to cancer.
Oral contraceptives should not be taken if cholestasis or jaundice developed with previous use. Women who have had cholestasis of pregnancy may become jaundiced if they take oral contraceptives, and oral contraceptives should be used with caution.
Gallstones are not more likely to form in women who take low-dose oral contraceptives.
The risk of having a heart attack is increased if women who are 35 years or older and who smoke take oral contraceptives. Typically, such women should not use oral contraceptives.
If women have a high triglyceride (a fat) level, taking combination oral contraceptives can increase the level even more. A high triglyceride level may increase the risk of a heart attack or stroke in people who have other risk factors for these disorders. Oral contraceptives increase the risk of blood clots (which can also contribute to heart attacks and strokes). So, women with a high triglyceride level should not take combination oral contraceptives.
Rarely, a noncancerous liver tumor (hepatocellular adenoma) develops. If this tumor suddenly ruptures and bleeds into the abdominal cavity, emergency surgery is required. However, such bleeding is rare. Taking oral contraceptives for a long time and in high doses increases the risk of developing this tumor. The tumor usually disappears after oral contraceptives are stopped.
Taking certain medications can make oral contraceptives less effective. These medications include the following:
Some antiseizure medications (mainly phenytoin, carbamazepine, primidone, topiramate, and oxcarbazepine)(mainly phenytoin, carbamazepine, primidone, topiramate, and oxcarbazepine)
A certain combination of medications used to treat human immunodeficiency virus (HIV) infection (ritonavir plus another protease inhibitor)(HIV) infection (ritonavir plus another protease inhibitor)
The antibiotics rifampin and rifabutinThe antibiotics rifampin and rifabutin
If women taking oral contraceptives have to take one of these medications, they should also use another contraceptive method while they are taking the medication, and they should continue using another contraceptive method until their first period occurs after they stop the medication. Women should not take lamotrigine (an antiseizure medication) with oral contraceptives. Oral contraceptives may make lamotrigine less effective in controlling seizures.If women taking oral contraceptives have to take one of these medications, they should also use another contraceptive method while they are taking the medication, and they should continue using another contraceptive method until their first period occurs after they stop the medication. Women should not take lamotrigine (an antiseizure medication) with oral contraceptives. Oral contraceptives may make lamotrigine less effective in controlling seizures.
Conditions that prohibit the use of combination oral contraceptives
A woman should not take combination oral contraceptives (pills that contain estrogen and a progestin) if any of the following conditions are present:
Recently postpartum (gave birth within the last 21 days)
Hereditary condition that increases risk of blood clots or current or past blood clots in the legs (deep vein thrombosis) or lungs (pulmonary embolism)
Active cancer, except for nonmelanoma skin cancer
Current breast cancer
Prolonged immobility due to major surgery
Migraines with an aura (symptoms that occur before the headache, such as seeing jagged, shimmering, or flashing lights or having unusual sensations in the skin)
Smokes cigarettes and is 35 years or older
High blood pressure that is severe
Peripartum cardiomyopathy (heart damage that occurred during pregnancy)
Heart valve disorder that is causing health problems
Diabetes for more than 20 years or diabetes that has damaged blood vessels, such as those in the eyes (causing loss of vision)
Systemic lupus erythematosus or risk factors for developing blood clots related to lupus
Organ transplant with complications
Hepatitis, cirrhosis that is severe, or a liver tumor
Active viral hepatitis
Other considerations
Other factors may pose health risks with use of combination oral contraceptives, and should be discussed with a doctor before starting this birth control method. These include
Risk factors for forming blood clots (especially soon after pregnancy)
Smoking
High blood pressure
Heart disease
Gallbladder or liver disorders
History bariatric surgery
Past breast cancer
Multiple sclerosis with mobility issues
Use of certain antibiotics or antiseizure medications
Progestin-only contraceptives have fewer risks and are often taken by women who cannot take estrogen. Some factors that may pose health risks with use of progestin-only contraceptives and should be discussed with a doctor include
Current abnormal vaginal bleeding
High blood pressure
Heart disease
Blood vessel disorders due to diabetes or lupus
Liver disorders
Bariatric surgery
History of breast cancer
Oral contraceptives cause no increase, or possibly a small increase, in the risk of breast cancer in women who are currently taking them or who took them within the past few years.
For healthy women who do not smoke, taking low-dose combination pills with a low dose of estrogen does not increase the risk of having a stroke or heart attack.
Contraceptive Skin Patches and Vaginal Rings
Combined estrogen-progestin contraceptives are available as skin patches and vaginal rings. They should be used for 3 weeks, then not used for 1 week to allow the menstrual period to occur. If women do not start using the patch or ring during the first 5 days of their period, they must use a backup method of birth control during the first 7 days that they use the patch or ring.
Contraceptive skin patches and vaginal rings are effective. Approximately 0.3% of women who use one of these methods as instructed become pregnant during the first year of use. With typical use (the way most people use them), about 9% become pregnant during the first year. Effectiveness is similar to that of oral contraceptives. The patch may be less effective in overweight women than in women with a lower weight.
Women are more likely to use the patch or ring as instructed compared with oral contraceptives, because dosing is every 1 to 3 weeks rather than daily.
Breakthrough bleeding is uncommon when the patch or ring is used. Irregular bleeding becomes more common the longer women use transdermal or ring contraception.
Women with certain conditions who should not use combination oral contraceptives should also not use contraceptive skin patches or vaginal rings.
Skin patches
A contraceptive skin patch is attached to the skin with an adhesive. It should be left in place for 1 week, then removed and replaced with a new patch, which is placed on a different area of the skin. A new patch is applied once a week (on the same day each week) for 3 weeks, followed by a week when no patch is used.

If more than 2 days go without using the patch, women should use a backup contraceptive method for 7 days in addition to the patch. If 2 days go by and women have had unprotected intercourse in the 5 days before those 2 days, they can consider emergency contraception.
Exercise and use of saunas or hot tubs do not displace the patch.
The patch may be less effective in women who weigh more than 198 pounds or have a body mass index (BMI) of 30 or more.
Spotting or bleeding between periods (breakthrough bleeding) is uncommon. Irregular bleeding becomes more common the longer women use the patch.
Skin under and around the patch may become irritated.

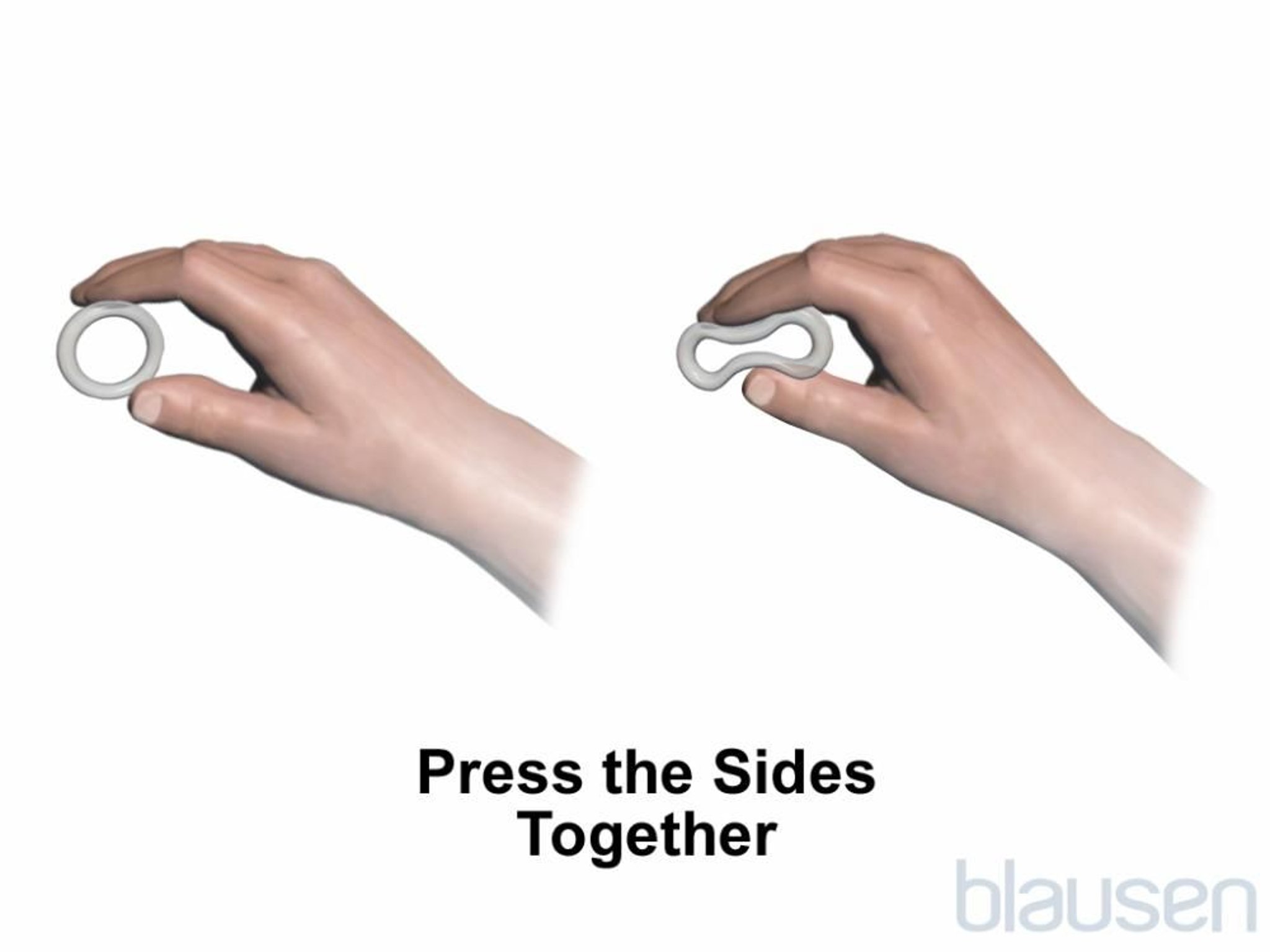
Vaginal rings
A vaginal ring is a small flexible, soft, transparent device that is placed in the vagina.
Two types of rings are available:
One that must be replaced each month
One that must be replaced only once a year
Both types of rings are typically left in place for 3 weeks, then removed for 1 week to allow the menstrual period to occur. The year-long ring is removed, left out for 1 week, and then the same ring is reinserted.
A woman can place and remove the vaginal ring herself. The ring comes in one size and can be placed anywhere in the vagina.
Women may wish to remove the vaginal ring at times other than after 3 weeks. However, if the ring is removed for more than 3 hours, women should use a backup contraceptive method for 7 days in addition to the ring.
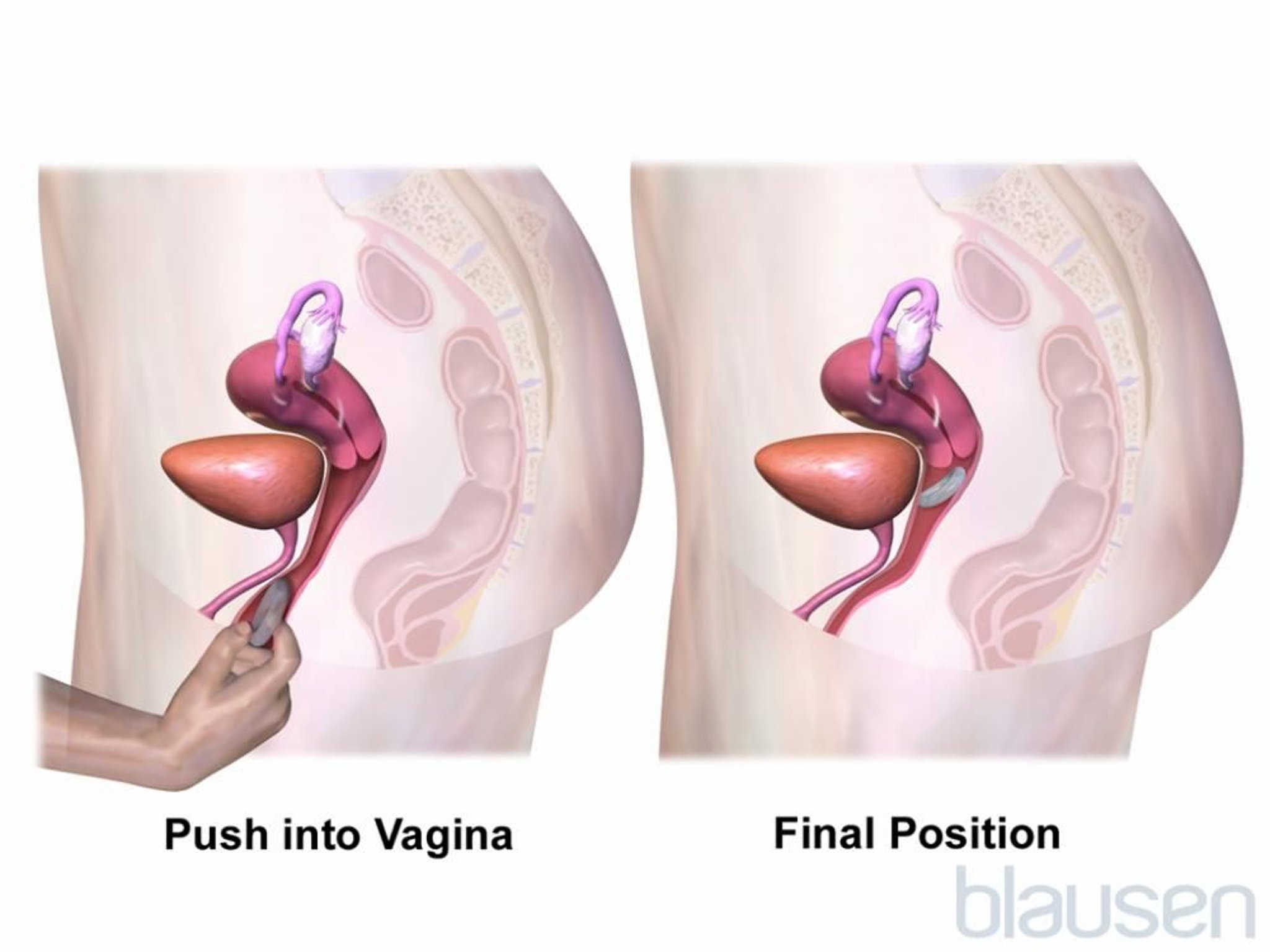
Usually, the vaginal ring is not felt by the woman’s partner during intercourse. The ring does not dissolve and cannot be pushed too far up.
Side effects
If women use a patch or a ring for 3 weeks (replacing it each week), followed by 1 week when no patch or ring is used, they typically have a regular menstrual period. Spotting or bleeding between periods (breakthrough bleeding) is uncommon. Irregular bleeding becomes more common the longer women use the ring.
Side effects, effects on the risk of developing disorders, and restrictions on use are similar to those of combination oral contraceptives.
Contraceptive Implants
A contraceptive implant is a single match-sized rod containing a progestin. The implant releases the progestin slowly into the bloodstream. The type of implant available in the United States is effective for 3 and possibly up to 5 years. Other contraceptive implants are available elsewhere in the world.
Only a very small percentage (0.05%) of women become pregnant during the first year of use.
After numbing the skin with an anesthetic, a doctor uses a needle-like instrument (trocar) to place the implant under the skin of the inner arm above the elbow. No incision or stitches are necessary. Doctors must receive special training before they can do this procedure.
If women have not had unprotected sex since their last period, an implant can be inserted at any time during the menstrual cycle. If women have had unprotected sex, they should use another form of contraception until their next menstrual period occurs or until a pregnancy test is done and rules out pregnancy. If women are not pregnant, the implant can be inserted. An implant can also be inserted immediately after a miscarriage, an abortion, or delivery of a baby.
If the implant is not inserted within 5 days after a woman's periods starts, she should use a backup contraceptive method for 7 days in addition to the implant.
The most common side effects are irregular or no menstrual periods and headaches. These side effects prompt some women to have the implant removed. Because the implant does not dissolve in the body, a doctor has to make an incision in the skin to remove it. Removal is more difficult than insertion because tissue under the skin thickens around the implant.
As soon as the implant is removed, the ovaries return to their normal functioning, and women become fertile again.
Contraceptive Injections
Various contraceptive progestin injections are available worldwide.
Depot medroxyprogesterone acetate (DMPA)Depot medroxyprogesterone acetate (DMPA) is available in the United States and is injected by a health care professional once every 3 months into a muscle of the arm or buttock or under the skin.
DMPA injections are very effective. If women get the injections as instructed, only about 0.2% of them become pregnant during the first year of use. With typical use (the way most people use it—with delays between injections), about 6% become pregnant.
An injection may be given immediately after a miscarriage, an abortion, or delivery of a baby. If the interval between injections is more than 4 months, a pregnancy test is done to rule out pregnancy before the injection is given. If women do not get the first injection within 5 to 7 days after their period starts, they must use a backup method of contraception for 7 days after they get the injection.
Noristerat (NET-EN), which is available in many countries but not in the United States, is a long-acting injectable contraceptive. Pregnancy rates are the same as with DMPA. NET-EN may be given as an injection deep into a muscle of the buttock, typically every 8 weeks, but the interval can be extended to 12 weeks after the first 6 months of use. If the interval between injections is more than 13 weeks, a pregnancy test is done to rule out pregnancy before the injection is given. Like DMPA, if women do not get the first injection within 5 to 7 days after their period starts, they must use a backup method of contraception for 7 days after they get the injection. And like DMPA, NET-EN may also be given immediately after a miscarriage, an abortion, or delivery of a baby.
Side effects
The progestin completely disrupts the menstrual cycle. About one third of women using this contraceptive have no menstrual bleeding during the 3 months after the first injection, and another third have irregular bleeding and spotting for more than 11 days each month. After this contraceptive is used for a while, irregular bleeding occurs less often. After 2 years, about 70% of the women have no bleeding at all. When the injections are stopped, a regular menstrual cycle resumes in about half the women within 6 months and in about three fourths within 1 year. Fertility may not return for up to 18 months after injections are stopped. For women using NET-EN, return to ovulation occurs more rapidly, with an average of 3 months, and return to fertility within 6 months
Women typically gain 3 to 9 pounds during the first year of use and continue to gain weight. The weight gain is probably due to changes in appetite. So to prevent this gain, women need to limit calories and increase the amount of exercise they do.
DMPA does not appear to worsen depression in women who have depression before they start this medication. Some studies have reported an increased risk of depression after pregnancy (postnatal depression) for NET-EN users.
Headaches are common, but they usually become less severe over time. If women have had tension headaches or migraines in the past, the injections do not make them worse.
Bone density temporarily decreases. However, the risk of fractures does not increase, and bones usually return to their previous density after the injections are stopped. Participating in physical activity and weight bearing exercise, and getting enough calcium and vitamin D daily to help maintain bone density is important for all women, but it is particularly important for adolescent and young women who are getting progestin injections. Calcium and vitamin D supplements are often needed to get the required amount.daily to help maintain bone density is important for all women, but it is particularly important for adolescent and young women who are getting progestin injections. Calcium and vitamin D supplements are often needed to get the required amount.
In some women, DMPA increases the levels of triglycerides and low-density lipoprotein (LDL) cholesterol. However, this effect appears to be temporary and improve within 36 months of DMPA use. A similar effect would be expected with NET-EN.
Benefits
DMPA does not increase the risk of developing breast, ovarian, or cervical cancer.
Contraceptive injections may lower the risk of developing
Cancer of the uterus (endometrial cancer)
Pelvic inflammatory disease (an infection of the upper female reproductive organs)
Interactions with other medications are uncommon.
Unlike combination oral contraceptives, progestin injections do not appear to increase the risk of high blood pressure or blood clots.
Contraceptive injections are currently considered safe for women who should not take estrogen and may be a good choice for women with a seizure disorder.







