

Atrial flutter is a rapid regular atrial rhythm due to an atrial macroreentrant circuit. Symptoms include palpitations and sometimes weakness, effort intolerance, dyspnea, and presyncope. Atrial thrombi may form and embolize. Diagnosis is by electrocardiography. Treatment involves rate control with medication, prevention of thromboembolism with anticoagulants, and often conversion to sinus rhythm with medication, cardioversion, or atrial flutter substrate ablation.
(See also Overview of Arrhythmias.)
Atrial flutter is much less common than atrial fibrillation, but its causes and hemodynamic consequences are similar. Many patients with atrial flutter also have periods of atrial fibrillation. In a population-based study of patients with a first diagnosis of atrial flutter, 69% were already known to have atrial fibrillation and, of those not known to have had atrial fibrillation, 40% were found to have atrial fibrillation over the next 3 years (1).
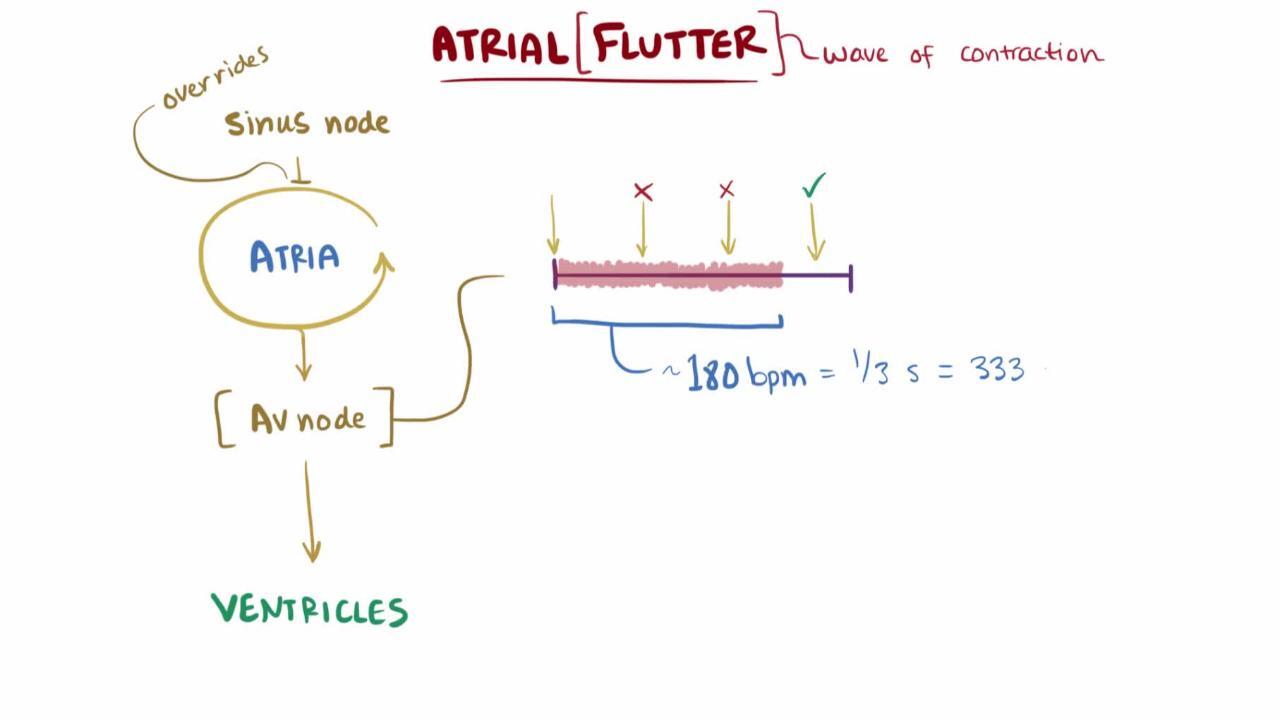
Typical atrial flutter is due to a large reentrant circuit involving most of the right atrium and requires conduction between the orifice of the inferior vena cava and the annulus of the tricuspid valve (the cavotricuspid isthmus). The atria depolarize at a rate of 250 to 350 beats/minute (typically 300 beats/minute). Because the atrioventricular (AV) node cannot usually conduct at this rate, typically half of the impulses get through (2:1 block), resulting in a regular ventricular rate of 150 beats/minute. Sometimes, the block varies from moment to moment, causing an irregular ventricular rhythm. Less commonly, a fixed 3:1, 4:1, or 5:1 block may be present.
The probability of a thromboembolic event in isolated atrial flutter is thought to be about half of that in atrial fibrillation (2). However, many patients with atrial flutter also have (or will develop) atrial fibrillation. Accordingly, guidelines for anticoagulation make no distinction between patients with atrial flutter and those with atrial fibrillation (3).
General references
1. Gula LJ, Redfearn DP, Jenkyn KB, et al: Elevated Incidence of Atrial Fibrillation and Stroke in Patients With Atrial Flutter—A Population-Based Study. Can J Cardiol 34(6):774–783, 2018. doi: 10.1016/j.cjca.2018.01.001
2. Biblo LA, Yuan Z, Quan KJ, et al: Risk of stroke in patients with atrial flutter. Am J Cardiol 87(3):346–349, 2001. doi: 10.1016/s0002-9149(00)01374-6
3. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193
Symptoms and Signs of Atrial Flutter
Symptoms of atrial flutter depend primarily on ventricular rate and the nature of any underlying heart disorder. If ventricular rate is < 120 beats/minute and regular, there are likely to be few or no symptoms. Faster rates and variable AV conduction usually cause palpitations. Decreased cardiac output may cause symptoms of hemodynamic compromise (eg, chest discomfort, dyspnea, weakness, syncope). Close inspection of the jugular venous pulse reveals flutter a waves.
Diagnosis of Atrial Flutter
ECG
The diagnosis of atrial flutter is by electrocardiography (ECG). In typical flutter, ECG shows continuous and regular atrial activation with a sawtooth pattern, most obvious in leads II, III, and aVF (see figure Atrial Flutter).
Atrial Flutter
(Note: Conducted with right bundle branch block.) |

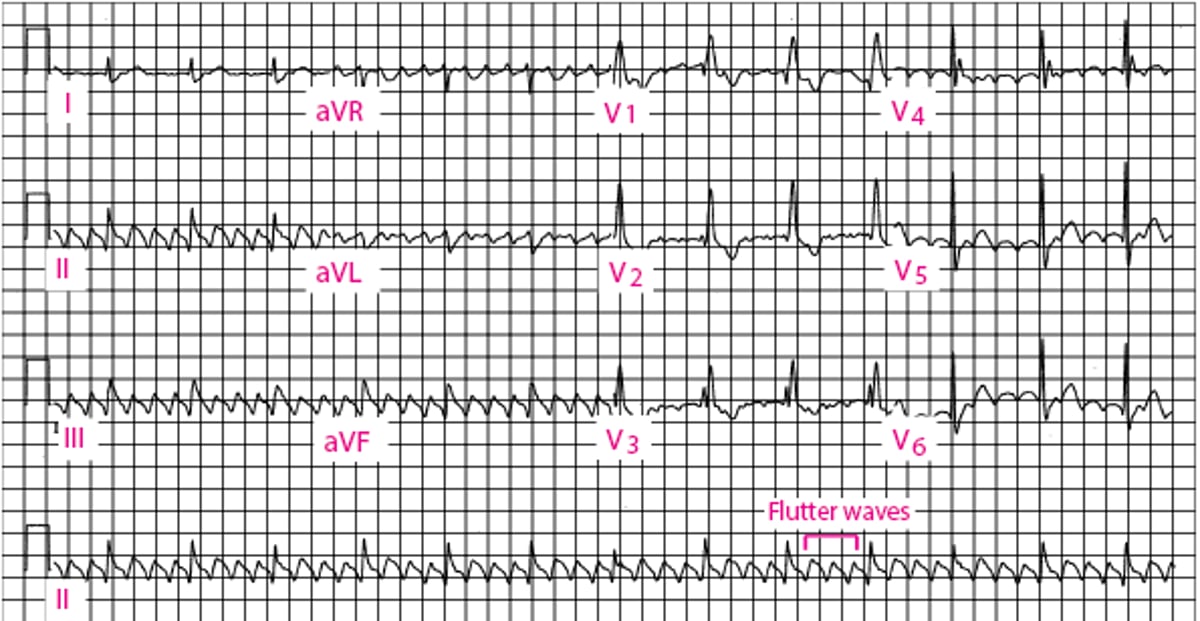
Carotid sinus massage can increase AV block and better expose the typical flutter waves. A similar response may follow pharmacologic AV nodal blockade (eg, with adenosine), but such therapy does not usually terminate atrial flutter.
Treatment of Atrial Flutter
Rate control with medication
Rhythm control with cardioversion, medication, or ablation
Prevention of thromboembolism
Treatment of atrial flutter focuses on ventricular rate control, rhythm control, and prevention of thromboembolism.
Pharmacologic rate control is more difficult to achieve in atrial flutter than in atrial fibrillation. Thus, for most patients, electrical conversion (using synchronized cardioversion or overdrive pacing) is the treatment of choice for an initial episode and is mandatory with 1:1 AV conduction or hemodynamic compromise. Typically, low-energy (50 joules) conversion is effective. Anticoagulation, as in atrial fibrillation, is necessary before cardioversion (1).
If medication is used to restore sinus rhythm, rate must first be controlled with beta-blockers or nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem). Many of the If medication is used to restore sinus rhythm, rate must first be controlled with beta-blockers or nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem). Many of theantiarrhythmic medications that can restore sinus rhythm (especially class Ia and Ic) can slow atrial flutter, shorten AV nodal refractoriness (by their vagolytic effects), or do both enough to allow 1:1 conduction with paradoxical increase in ventricular rate and hemodynamic compromise. These medications may be used for long-term maintenance as required to prevent recurrence in association with medication to prolong AV nodal refractoriness (class II, III, IV, or digoxin) (that can restore sinus rhythm (especially class Ia and Ic) can slow atrial flutter, shorten AV nodal refractoriness (by their vagolytic effects), or do both enough to allow 1:1 conduction with paradoxical increase in ventricular rate and hemodynamic compromise. These medications may be used for long-term maintenance as required to prevent recurrence in association with medication to prolong AV nodal refractoriness (class II, III, IV, or digoxin) (1).

An antitachycardia pacing system is an alternative to long-term use of antiarrhythmics and is a rare therapy used in patients with atrial flutter and an independent indication for pacing, such as a bradycardia, who are ineligible or in whom other approaches to rhythm control have failed.
Ablation procedures designed to interrupt the atrial reentrant circuit may effectively prevent atrial flutter, particularly typical atrial flutter. Because typical atrial flutter is dependent on conduction through the relatively narrow cavotricuspid isthmus, placement of an ablation line of block across the isthmus will cure typical atrial flutter in > 95% of patients. However, atrial fibrillation may recur in up to 60% of patients in the 10 years that follow successful atrial flutter ablation (2).
To prevent thromboembolism, patients with chronic or recurrent atrial flutter require an oral anticoagulant (warfarin titrated to an INR of 2 to 3, a direct patients with chronic or recurrent atrial flutter require an oral anticoagulant (warfarin titrated to an INR of 2 to 3, a directthrombin inhibitor, or a factor Xa inhibitor). The choice among the therapies is based on the same considerations as in the treatment of atrial fibrillation (1).
Treatment references
1. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193
2. Seara JG, Roubin SR, Sampedro FG, et al: Risk of atrial fibrillation, stroke, and death after radiofrequency catheter ablation of typical atrial flutter. Clin Res Cardiol 103(7):543–552, 2014. doi: 10.1007/s00392-014-0682-6
Key Points
Atrial flutter is a rapid, regular atrial rhythm that may cause an regular, irregular, tachycardic, or nontachycardic QRS response, depending on the degree and type of block present.
After initial rate control with medications such as beta-blockers and nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem), most patients should have pharmacologic or direct current cardioversion.After initial rate control with medications such as beta-blockers and nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem), most patients should have pharmacologic or direct current cardioversion.
Anticoagulation is usually necessary before cardioversion.
Long-term oral anticoagulation to prevent stroke is required for patients with chronic or recurrent atrial flutter.
Recurrent episodes are prevented with class Ia, Ic, or III antiarrhythmic medications along with AV nodal suppression or, more effectively, by cavotricuspid isthmus ablation.
Drugs Mentioned In This Article





