



Staphylococcal scalded skin syndrome is an acute epidermolysis caused by a staphylococcal toxin. Infants and children are most susceptible. Symptoms are widespread bullae with epidermal sloughing. Diagnosis is by examination and sometimes biopsy. Treatment is antistaphylococcal antibiotics and local care. Prognosis is excellent with timely treatment.
")
")
")

 and Toxic Epidermal Necrolysis (TEN)")
(See also Overview of Bacterial Skin Infections.)
Staphylococcal scalded skin syndrome almost always affects children < 6 years (especially infants); it rarely occurs in older adults unless they have renal failure or are immunocompromised. Epidemics may occur in nurseries, presumably transmitted by the hands of personnel who are in contact with an infected infant or who are nasal carriers of Staphylococcus aureus. Sporadic cases also occur.
Staphylococcal scalded skin syndrome is caused by group II coagulase-positive staphylococci, usually phage types 55 and 71, which elaborate exfoliatin (also called epidermolysin), a toxin that splits the upper part of the epidermis just beneath the granular cell layer by targeting desmoglein-1 (see Staphylococcal Infections).
The primary infection often begins during the first few days of life in the umbilical stump or diaper area; in older children, the face is the typical site. Toxin produced in these areas enters the circulation and affects the entire skin.
Symptoms and Signs of Staphylococcal Scalded Skin Syndrome
When a localized area of infection can be found (eg, impetigo), the initial lesion is usually superficial and crusted. Within 24 hours, the surrounding skin becomes painful and erythematous, changes that quickly spread to other areas. The skin may be exquisitely tender and have a wrinkled tissue paper–like consistency.
Large, flaccid blisters arise on the erythematous skin and quickly break to produce erosions. Blisters are frequently present in areas of friction, such as intertriginous areas, buttocks, hands, and feet. Intact blisters extend laterally with gentle pressure (Nikolsky sign).
The epidermis may peel easily, often in large sheets. Widespread desquamation occurs within 36 to 72 hours, and patients may become very ill with systemic manifestations (eg, malaise, chills, fever). Desquamated areas appear scalded. Loss of the protective skin barrier can lead to sepsis and to fluid and electrolyte imbalance.

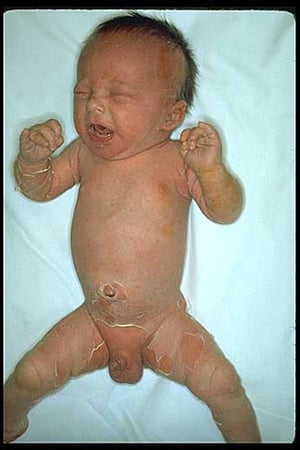
Staphylococcal scalded skin syndrome is epidermolysis caused by a staphylococcal toxin. Findings include erythema with overlying desquamation in sheets, particularly in the intertriginous area of the groin and axillae. Often there is also perioral peeling.
Image courtesy of Thomas Habif, MD.


This photo shows the leg of a patient with all three stages of the infection: erythema (at center), bullae (left), and desquamation (right).
SCIENCE PHOTO LIBRARY


This image shows staphylococcal scalded skin syndrome with superficial skin blistering caused by Staphylococcus aureus infection. This syndrome is rare in adults but can occur in people who are immunocompromised or who have renal failure or another chronic disease.
DermPics/SCIENCE PHOTO LIBRARY
Staphylococcal scalded skin syndrome is epidermolysis caused by a staphylococcal toxin. Findings include erythema with overlying desquamation in sheets, particularly in the intertriginous area of the groin and axillae. Often there is also perioral peeling.
Image courtesy of Thomas Habif, MD.
This photo shows the leg of a patient with all three stages of the infection: erythema (at center), bullae (left), and desquamation (right).
SCIENCE PHOTO LIBRARY
This image shows staphylococcal scalded skin syndrome with superficial skin blistering caused by Staphylococcus aureus infection. This syndrome is rare in adults but can occur in people who are immunocompromised or who have renal failure or another chronic disease.
DermPics/SCIENCE PHOTO LIBRARY
Diagnosis of Staphylococcal Scalded Skin Syndrome
Clinical examination
Cultures from areas of suspected primary infection
Diagnosis of staphylococcal scalded skin syndrome is suspected clinically, but confirmation may require biopsy (frozen section may give earlier results). Specimens show noninflammatory superficial splitting of the epidermis.
Cultures should be taken from the conjunctiva, nasopharynx, blood, urine, and areas of possible primary infection, such as the umbilicus in a neonate or suspect skin lesions. Cultures should not be taken from bullae because they are sterile, unlike in bullous impetigo, where cultures of the blister fluid yield a pathogen.
Differential diagnosis
Differential diagnosis includes drug hypersensitivity, viral exanthemas, scarlet fever, thermal burns, genetic bullous diseases (eg, some types of epidermolysis bullosa), acquired bullous diseases (eg, pemphigus vulgaris, bullous pemphigoid), and toxic epidermal necrolysis (see table Differentiating Staphylococcal Scalded Skin Syndrome (SSSS) and Toxic Epidermal Necrolysis (TEN) and see Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis (TEN)).
The mucosal surfaces are spared in staphylococcal scalded skin syndrome; however, they are affected in Stevens-Johnson syndrome and toxic epidermal necrolysis.
Differentiating Staphylococcal Scalded Skin Syndrome (SSSS) and Toxic Epidermal Necrolysis (TEN)
Feature | SSSS | TEN |
|---|---|---|
Patients affected | Infants, young children, and adults who are immunocompromised | Older adults |
Patient history | Recent staphylococcal infection | Medication use |
Level of epidermal cleavage (blister formation)* | Within the granular cell (outermost) layer of the epidermis | Between the epidermis and dermis or at the level of the basal cell |
* Determined by Tzanck test or by a frozen section of a fresh specimen. | ||
Treatment of Staphylococcal Scalded Skin Syndrome
Antibiotics
Gel dressings for weeping lesions
Penicillinase-resistant antistaphylococcal antibiotics given IV must be started immediately. Typically nafcillin is given until improvement is noted, followed by oral cloxacillin. Oxacillin and cephalosporins (eg, cefazolin) are alternatives. Most cases are caused by methicillin-susceptible Penicillinase-resistant antistaphylococcal antibiotics given IV must be started immediately. Typically nafcillin is given until improvement is noted, followed by oral cloxacillin. Oxacillin and cephalosporins (eg, cefazolin) are alternatives. Most cases are caused by methicillin-susceptibleS. aureus (MSSA), but vancomycin, linezolid, or other (MSSA), but vancomycin, linezolid, or otherantibiotics effective against MRSA should be considered in areas with a high prevalence of methicillin-resistant S. aureus (MRSA) or in patients whose initial therapy failed. Corticosteroids are contraindicated.
Emollients (eg, white petrolatum) are sometimes used to prevent further insensible water loss from ulcerated skin. However, topical therapy and patient handling must be minimized.
If disease is widespread and lesions are weeping, the skin should be treated as for burns. Hydrolyzed polymer gel dressings may be very useful; the number of dressing changes should be minimized. Patients should be monitored and treated for complications similar to those that occur with burns (eg, fluid and electrolyte imbalance, sepsis).
Steps to detect carriers and prevent or treat nursery epidemics are discussed elsewhere (see prevention of neonatal hospital-acquired infection).
Prognosis for Staphylococcal Scalded Skin Syndrome
With prompt diagnosis and therapy, death rarely occurs; the stratum corneum is quickly replaced, and healing usually occurs within 5 to 7 days after start of treatment.
Key Points
Generalized desquamation and systemic illness most often indicate staphylococcal scalded skin syndrome (SSSS) in infants and young children (and occasionally in adults who are immunocompromised), whereas in older adults, they most often indicate toxic epidermal necrolysis.
Culture the conjunctiva, nasopharynx, blood, urine, and areas of possible primary infection, such as the umbilicus and suspect skin lesions.
Treat patients with antistaphylococcal antibiotics and, if disease is widespread, in a burn unit if possible.
Monitor and treat for complications similar to those that occur with burns (eg, fluid and electrolyte imbalance, sepsis).







