



")



Tinea capitis is a dermatophytosis that mainly affects children, is contagious, and can be epidemic.
Trichophyton tonsurans is the most common cause in the United States, followed by Microsporum canis and M. audouinii; other Trichophyton species (eg, T. schoenleinii, T. violaceum) are common elsewhere.
Tinea capitis causes the gradual appearance of round patches of dry scale, alopecia, or both. T. tonsurans infection causes black dot ringworm, in which hair shafts break at the scalp surface; M. audouinii infection causes gray patch ringworm, in which hair shafts break above the surface, leaving short stubs. Tinea capitis less commonly manifests as diffuse scaling, like dandruff, or in a diffuse pustular pattern.



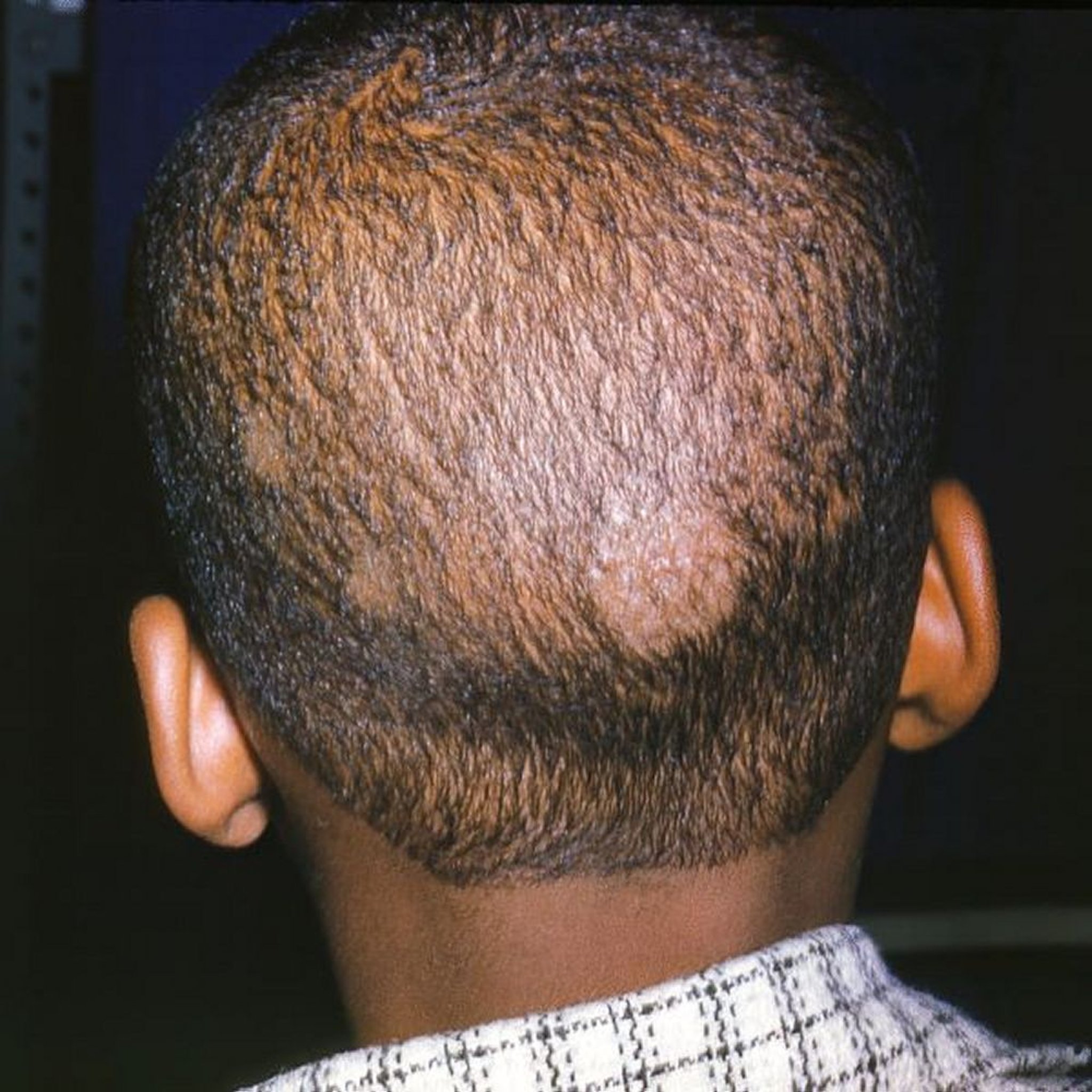
Image courtesy of Karen McKoy, MD.
Kerion
Dermatophyte infection occasionally leads to formation of a kerion, which is a large, boggy, inflammatory scalp mass caused by a severe inflammatory reaction to the dermatophyte. A kerion may have pustules and crusting and can be mistaken for an abscess. A kerion may result in scarring hair loss.




Image courtesy of Karen McKoy, MD.
Diagnosis of Tinea Capitis
Clinical appearance
Potassium hydroxide wet mount
Sometimes a Wood light examination and sometimes culture
Tinea capitis is diagnosed by clinical appearance and by potassium hydroxide wet mount of plucked hairs or of hairs and scale obtained by scraping or brushing. Spore size and appearance inside (endothrix) or outside (ectothrix) the hair shaft distinguish organisms and can help guide treatment.
Blue-green fluorescence during a Wood light examination is diagnostic for infection with M. canis and M. audouinii and can distinguish tinea from erythrasma.
Fungal culture of plucked hairs can be done when necessary. In a child, a scalp lesion that appears similar to an abscess may be a kerion; if necessary, cultures can help make the distinction.
Pearls & Pitfalls
|
Differential diagnosis of tinea capitis includes
Treatment of Tinea Capitis
Oral antifungals
Selenium sulfide shampoo
Sometimes prednisone
(See table Options for Treatment of Superficial Fungal Infections.)
Terbinafine is a first-line treatment in children because of its shorter treatment duration. Alternatively, children may be treated with oral griseofulvin, which is sometimes preferred by insurers because of its lower cost.Terbinafine is a first-line treatment in children because of its shorter treatment duration. Alternatively, children may be treated with oral griseofulvin, which is sometimes preferred by insurers because of its lower cost.
An imidazole or ciclopirox cream can be applied to the scalp to prevent spread, especially to other children, until tinea capitis is cured; selenium sulfide 2.5% shampoo should also be used at least twice a week. Children may attend school during treatment.An imidazole or ciclopirox cream can be applied to the scalp to prevent spread, especially to other children, until tinea capitis is cured; selenium sulfide 2.5% shampoo should also be used at least twice a week. Children may attend school during treatment.
Adults are treated with terbinafine, which is more effective for endothrix infections, or itraconazole. Treatment can also include selenium sulfide 2.5% shampoo.Adults are treated with terbinafine, which is more effective for endothrix infections, or itraconazole. Treatment can also include selenium sulfide 2.5% shampoo.
For severely inflamed lesions and for kerion, a short course of prednisone should be added (to lessen symptoms and perhaps reduce the chance of scarring), starting with 40 mg orally once a day (1 mg/kg for children) and tapering the dose over 2 weeks.For severely inflamed lesions and for kerion, a short course of prednisone should be added (to lessen symptoms and perhaps reduce the chance of scarring), starting with 40 mg orally once a day (1 mg/kg for children) and tapering the dose over 2 weeks.
Key Points
Tinea capitis affects mostly children and can be contagious and epidemic.
Confirm tinea capitis by potassium hydroxide wet mount, fungal culture, or sometimes Wood light examination.
Treat with oral terbinafine or griseofulvin in addition to a topical antifungal.Treat with oral terbinafine or griseofulvin in addition to a topical antifungal.
Add a short course of oral prednisone for a kerion or severe inflammation.Add a short course of oral prednisone for a kerion or severe inflammation.
Drugs Mentioned In This Article






