


Topic Resources



Acid-base disorders are pathologic changes in partial pressure of carbon dioxide (Pco2) or serum bicarbonate (HCO3−) that typically produce abnormal arterial pH values.
Acidemia is serum pH < 7.35.
Alkalemia is serum pH > 7.45.
Acidosis refers to physiologic processes that cause acid accumulation or alkali loss.
Alkalosis refers to physiologic processes that cause alkali accumulation or acid loss.
Actual changes in pH depend on the degree of physiologic compensation and whether multiple processes are present.
(See also Acid-Base Regulation.)
Classification of Acid-Base Disorders
Primary acid-base disturbances are defined as metabolic or respiratory based on clinical context and whether the primary change in pH is due to an alteration in serum HCO3− or in Pco2.
Metabolic acidosis is serum HCO3−< 24 mEq/L (< 24 mmol/L). Causes are
Increased acid production
Acid ingestion
Decreased renal acid excretion
Gastrointestinal or renal HCO3− loss
Metabolic alkalosis is serum HCO3−> 28 mEq/L (> 28 mmol/L). Causes are
Acid loss
HCO3− retention
Respiratory acidosis is Pco2> 40 mm Hg (hypercapnia). Cause is
Decrease in minute ventilation (hypoventilation)
Respiratory alkalosis is Pco2< 38 mm Hg (hypocapnia). Cause is
Increase in minute ventilation (hyperventilation)
Compensatory mechanisms begin to correct the pH (see table Primary Changes and Compensations in Simple Acid-Base Disorders) whenever an acid-base disorder is present. Compensation cannot return pH completely to normal and never overshoots.

A simple acid-base disorder is a single acid-base disturbance with its accompanying compensatory response.
Mixed (sometimes called complex) acid-base disorders comprise ≥ 2 primary disturbances.
Pearls & Pitfalls
|
Primary Changes and Compensations in Simple Acid-Base Disorders
Primary Disturbance | pH | Bicarbonate (HCO3−) | Pco2 | Expected Compensation |
|---|---|---|---|---|
< 7.35 | Primary decrease | Compensatory decrease | 1.2 mm Hg decrease in Pco2 for every 1 mEq/L (1 mmol/L) decrease in HCO3− or* Pco2= (1.5 × HCO3−) + 8 (± 2) or Pco2= HCO3−+ 15 or Pco2= last 2 digits of pH ×100 | |
> 7.45 | Primary increase | Compensatory increase | 0.6–0.75 mm Hg increase in Pco2 for every 1 mEq/L (1 mmol/L) increase in HCO3− (Pco2 should not rise above 55 mm Hg in compensation) | |
< 7.35 | Compensatory increase | Primary increase | Acute: 1–2 mEq/L (1–2 mmol/L) increase in HCO3− for every 10-mm Hg increase in Pco2 Chronic: 3–4 mEq/L (3–4 mmol/L) increase in HCO3− for every 10-mm Hg increase in Pco2 | |
> 7.45 | Compensatory decrease | Primary decrease | Acute: 1–2 mEq/L (1–2 mmol/L) decrease in HCO3− for every 10-mm Hg decrease in Pco2 Chronic: 4–5 mEq/L (4–5 mmol/L) decrease in HCO3− for every 10-mm Hg decrease in Pco2 | |
* Imprecise but convenient rules of thumb. | ||||
HCO3- = bicarbonate; Pco2 = partial pressure of carbon dioxide. | ||||
Symptoms and Signs of Acid-Base Disorders
Compensated or mild acid-base disorders usually associated with this cause no noticeable symptoms or signs.
Severe, uncompensated disorders have multiple cardiovascular, respiratory, neurologic, and metabolic consequences (see table Clinical Consequences of Acid-Base Disorders and figure Oxyhemoglobin dissociation curve).
Clinical Consequences of Acid-Base Disorders
System | Acidemia | Alkalemia |
|---|---|---|
Cardiovascular | Impaired cardiac contractility Arteriolar dilation Venoconstriction Centralization of blood volume Increased pulmonary vascular resistance Decreased cardiac output Decreased systemic blood pressure Decreased hepatorenal blood flow Decreased threshold for cardiac arrhythmias Attenuation of responsiveness to catecholamines | Arteriolar constriction Reduced coronary blood flow Reduced anginal threshold Decreased threshold for cardiac arrhythmias |
Metabolic | Insulin resistance Inhibition of anaerobic glycolysis Reduction in ATP (adenosine triphosphate) synthesis Protein degradation Bone demineralization (chronic) | Stimulation of anaerobic glycolysis Formation of organic acids Decreased oxyhemoglobin dissociation Decreased ionized calcium |
Neurologic | Inhibition of metabolism and cell-volume regulation Obtundation and coma | Tetany Seizures Lethargy Delirium Stupor |
Respiratory | Compensatory hyperventilation with possible respiratory muscle fatigue | Compensatory hypoventilation with hypercapnia and hypoxemia |
Diagnosis of Acid-Base Disorders
Arterial blood gases (ABG)
Serum electrolytes
Anion gap calculated
If metabolic acidosis is present, delta gap calculated and Winters formula applied
Search for compensatory changes
Evaluation is with ABG and serum electrolytes. The ABG directly measures arterial pH and Pco2. HCO3− level reported on the arterial blood gas panel is calculated using the Henderson-Hasselbalch equation. The HCO3− level on the serum chemistry panel is directly measured. Directly measured HCO3− levels are considered more accurate in cases of discrepancy.
Acid-base balance is most accurately assessed with measurement of pH and Pco2 in an arterial blood sample. In cases of circulatory failure or during cardiopulmonary resuscitation, measurements from a sample of venous blood may more accurately reflect conditions at the tissue level and may be a more useful guide to bicarbonate administration and adequacy of ventilation.
The pH establishes the primary process (acidosis or alkalosis), although pH moves toward the normal range with compensation. Changes in Pco2 reflect the respiratory component, and changes in HCO3− reflect the metabolic component.
Complex or mixed acid-base disturbances involve more than one primary process. In these mixed disorders, values may be deceptively normal. Thus, when evaluating acid-base disorders, it is important to determine whether changes in Pco2 and HCO3− show the expected compensation (see table Primary Changes and Compensation in Simple Acid-Base Disorders). If not, then a second primary process should be suspected of causing the abnormal compensation. Interpretation must also consider clinical conditions (eg, chronic lung disease, renal failure, drug overdose).
The anion gap should always be calculated; elevation almost always indicates a metabolic acidosis. A normal anion gap with a low HCO3− level (eg, < 24 mEq/L [< 24 mmol/L]) and high serum chloride (Cl−) level indicates a non-anion gap (hyperchloremic) metabolic acidosis. If metabolic acidosis is present, a delta gap is calculated to identify concomitant metabolic alkalosis, and Winters formula is applied to determine whether respiratory compensation is appropriate or reflects a second acid-base disorder (predicted Pco2 = 1.5 [HCO3−] + 8 ± 2; if Pco2 is higher, there is also a primary respiratory acidosis—if lower, respiratory alkalosis).
Respiratory acidosis is suggested by Pco2> 40 mm Hg; HCO3− should compensate by increasing 3 to 4 mEq/L ( 3 to 4 mmol/L) for each 10-mm Hg rise in Pco2 sustained for 4 to 12 hours (there may be no increase or only an increase of 1 to 2 mEq/L [1 to 2 mmol/L], which slowly increases to 3 to 4 mEq/L [3 to 4 mmol/L] over days). Greater increase in HCO3− implies a primary metabolic alkalosis; lesser increase suggests no time for compensation or coexisting primary metabolic acidosis.
Metabolic alkalosis is suggested by HCO3−> 28 mEq/L (> 28 mmol/L). The Pco2 should compensate by increasing about 0.6 to 0.75 mm Hg for each 1 mEq/L (1 mmol/L) increase in HCO3− (up to about 55 mm Hg). Greater increase implies concomitant respiratory acidosis; lesser increase, respiratory alkalosis.
Respiratory alkalosis is suggested by Pco2< 38 mm Hg. The HCO3− should compensate over 4 to 12 hours by decreasing 4 to 5 mEq/L (4 to 5 mmol/L) for every 10 mm Hg decrease in Pco2. Lesser decrease means there has been no time for compensation or a primary metabolic alkalosis coexists. Greater decrease implies a primary metabolic acidosis.
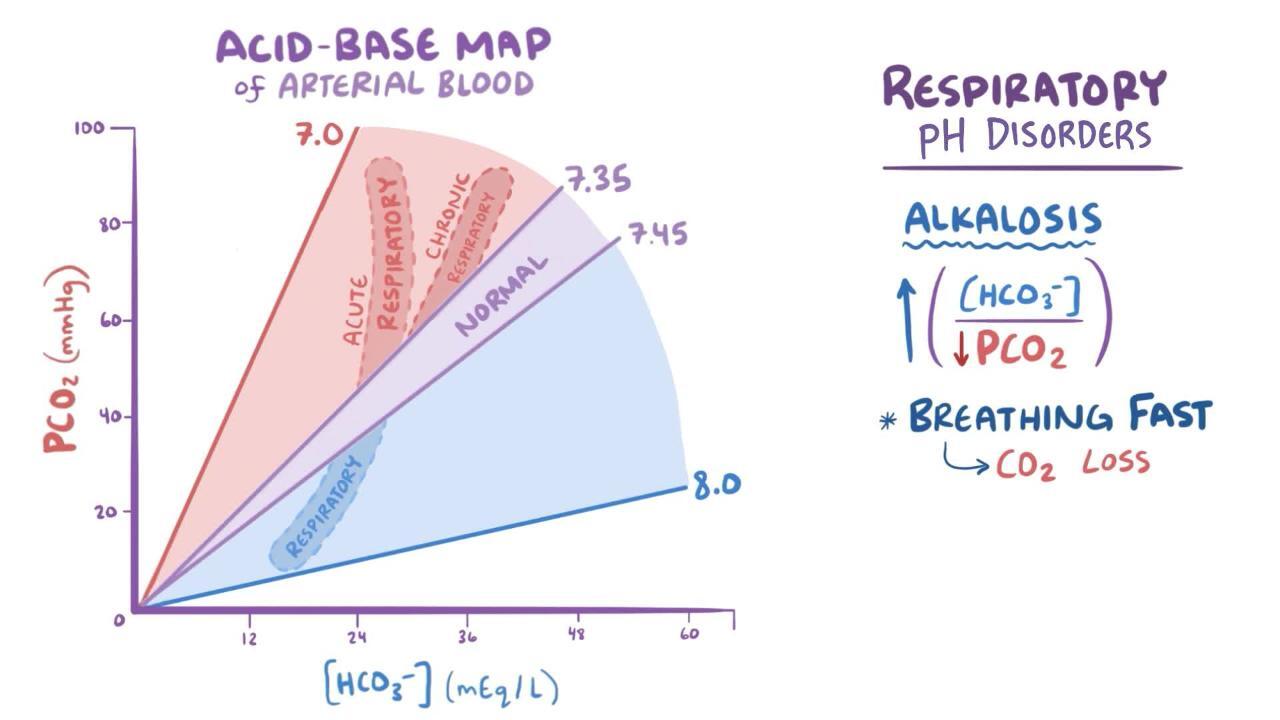
Nomograms (acid-base maps) are an alternative way to diagnose mixed disorders, allowing for simultaneous plotting of pH, HCO3−, and Pco2.

Calculation of the anion gap
The anion gap is defined as serum sodium (Na) concentration minus the sum of serum chloride (Cl−) and serum bicarbonate (HCO3−) concentrations.
Na+− (Cl−+ HCO3−)
The term “gap” is misleading, because the law of electroneutrality requires the same number of positive and negative charges in an open system; the gap appears on laboratory testing because certain cations (+) and anions (−) are not measured on routine laboratory chemistry panels. Thus,
Na++ unmeasured cations (UC) = Cl− + HCO3−+ unmeasured anions (UA)
and the anion gap,
Na+ − (Cl−+ HCO3−) = UA − UC
The predominant "unmeasured" anions are phosphate (PO43−), sulfate (SO4−), various negatively charged proteins, and some organic acids, accounting for 20 to 24 mEq/L (20 to 24 mmol/L).
The predominant "unmeasured" extracellular cations are potassium (K+), calcium (Ca++), and magnesium (Mg++) and account for about 11 mEq/L (5.5 mmol/L).
Thus, the typical anion gap is 23 − 11 = 12 mEq/L (12 mmol/L). The anion gap can be affected by increases or decreases in the UC or UA.
Increased anion gap is most commonly caused by metabolic acidosis in which negatively charged acids—mostly ketones, lactate, sulfates, or metabolites of methanol, ethylene glycol,or salicylate—consume (are buffered by) HCO3−. Other causes of increased anion gap include hyperalbuminemia or uremia (increased anions) and hypocalcemia or hypomagnesemia (decreased cations).
Decreased anion gap is unrelated to metabolic acidosis but is caused by hypoalbuminemia (decreased anions); hypercalcemia, hypermagnesemia, lithium intoxication, and hypergammaglobulinemia as occurs in myeloma (increased cations); or hyperviscosity or halide (bromide or iodide) intoxication. The effect of low albumin can be accounted for by adjusting the normal range for the anion gap 2.5 mEq/L (2.5 mmol/L) downward for every 1g/dL (10 g/L) fall in albumin.
Negative anion gap occurs rarely as a laboratory artifact in severe cases of hypernatremia, hyperlipidemia, and bromide intoxication.
The delta gap: The difference between the patient’s anion gap and the normal anion gap is termed the delta gap. This amount is considered an HCO3− equivalent, because for every unit rise in the anion gap, the HCO3− should lower by 1 (by buffering). Thus, if the delta gap is added to the measured HCO3−, the result should be in the normal range for HCO3−; elevation indicates the additional presence of a metabolic alkalosis.
Example: A vomiting, ill-appearing patient with alcohol use disorder has laboratory results showing
Na: 137
K: 3.8
Cl: 90
HCO3−: 22
pH: 7.40
Pco2: 41
Po2: 85
At first glance, the results appear unremarkable. However, calculations show elevation of the anion gap:
Na - (Cl + HCO3-) = 137 − (90 + 22) = 25 (normal, 10 to 12)
indicating a metabolic acidosis. Respiratory compensation is evaluated by Winters formula:
Predicted Pco2= 1.5[HCO3-] + 8 ± 2 = 1.5 (22) + 8 ± 2 = 41 ± 2
Predicted = measured, so respiratory compensation is appropriate.
Because there is metabolic acidosis, the delta gap is calculated, and the result is added to measured HCO3−:
Delta gap = calculated anion gap − normal anion gap = 25 − 10 = 15
Corrected HCO3- = delta gap + HCO3- = 15 + 22 = 37
The resulting corrected HCO3− (37) is above the normal range for HCO3−(22 to 29), indicating a primary metabolic alkalosis is also present. Thus, the patient has a mixed acid-base disorder.
Using clinical information, one could theorize a metabolic acidosis arising from alcoholic ketoacidosis combined with a metabolic alkalosis from recurrent vomiting with loss of acid (primarily HCl) and volume. The management of this patient should include treatments to address each primary acid-base disorder.
Key Points
Acidosis and alkalosis refer to physiologic processes that cause accumulation or loss of acid and/or alkali; blood pH may or may not be abnormal.
Acidemia and alkalemia refer to an abnormally acidic (pH < 7.35) or alkalotic (pH > 7.45) serum pH.
Acid-base disorders are classified as metabolic if the change in pH is primarily due to an alteration in serum bicarbonate (HCO3−) and respiratory if the change is primarily due to a change in Pco2 (increase or decrease in ventilation).
The pH establishes the primary process (acidosis or alkalosis), changes in Pco2 reflect the respiratory component, and changes in HCO3− reflect the metabolic component.
All acid-base disturbances result in compensation that tends to normalize the pH. Metabolic acid-base disorders result in respiratory compensation (change in Pco2); respiratory acid-base disorders result in metabolic compensation (change in HCO3− ).
More than one primary acid-base disorder may be present simultaneously. It is important to identify and address each primary acid-base disorder.
Initial laboratory evaluation of acid-base disorders includes measurement of arterial blood gases and serum electrolytes and calculation of the anion gap.
Use one of several formulas, rules-of-thumb, or an acid-base nomogram to determine if laboratory values are consistent with a single acid-base disorder (and compensation) or if a second primary acid-base disorder is also present.
Treat each primary acid-base disorder.






