



Gait disorders encompass a number of abnormal walking patterns, including slowing of gait speed and loss of smoothness, symmetry, stride length, and synchrony of body movement; they often indicate one or more underlying conditions.



Gait directly influences mobility, independence, and overall functional capacity. Maintaining a stable, efficient gait ensures that people can perform daily activities, reduce fall risk, and have a higher quality of life in their later years. Gait disorders include slowing of gait speed and loss of smoothness, symmetry, stride length, and synchrony of body movement.
For older adults, walking, standing up from a chair, turning, and leaning are necessary for independent mobility. Gait speed, chair rise time, and the ability to do tandem stance (standing with one foot in front of the other—a measure of balance) are independent predictors of the ability to do instrumental activities of daily living (eg, shopping, traveling, cooking) and of the risk of nursing home admission and death.
Walking without assistance requires synchronization of various neurologic networks that affect attention, strength, sensation, and coordination. Dementia can significantly affect walking by impairing attention, muscle strength, and the motor control needed to coordinate sensory input and muscle contraction for safe and steady ambulation.
Pearls & Pitfalls
|
Normal Age-Related Changes in Gait
Some elements of gait normally change with aging; others do not.
Gait velocity (speed of walking) remains stable until about age 70; it then declines about 15%/decade for usual gait and 20%/decade for fast walking. Gait velocity is a powerful predictor of mortality—as powerful as an older adult's number of chronic medical conditions and hospitalizations. After age 75, slow walkers die ≥ 6 years earlier than normal velocity walkers and ≥ 10 years earlier than fast velocity walkers. Gait velocity slows because older adults take shorter steps at the same rate (cadence). The most likely reason for shortened step length (the distance from one heel strike to the next) is weakness of the calf muscles, which propel the body forward; calf muscle strength is substantially decreased in older adults. However, older adults seem to compensate for decreased lower calf power by using their hip flexor and extensor muscles more than young adults.
Cadence (reported as steps/minute) does not change with aging. Each person has a preferred cadence, which is related to leg length and usually represents the most energy-efficient rhythm. Tall people take longer steps at a slower cadence; short people take shorter steps at a faster cadence.
Double stance time (ie, time with both feet on the ground during ambulation—a more stable position for moving the center of mass forward) increases with age. The percentage of time in double stance goes from 18% in young adults to ≥ 26% in healthy older adults. Increased time in double stance reduces the time the swing leg has to advance and shortens step length. Older adults may increase their double stance time even more when they walk on uneven or slippery surfaces, when they have impaired balance, or when they are afraid of falling. They may appear as if they are walking on slippery ice.
Walking posture changes only slightly with aging. Older adults walk upright, with no forward lean. However, older adults walk with greater anterior (downward) pelvic rotation and increased lumbar lordosis. This posture change is usually due to a combination of weak abdominal muscles, tight hip flexor muscles, and increased abdominal fat. Older adults also walk with their legs rotated laterally (toes out) about 5°, possibly because of a loss of hip internal rotation or in order to increase lateral stability. Foot clearance in swing is unchanged with advancing age.
Joint motion changes slightly with aging. Ankle plantar flexion is reduced during the late stage of stance (just before the back foot lifts off). The overall motion of the knee is unchanged. Hip flexion and extension are unchanged, but the hips have increased adduction. Pelvic motion is reduced in all planes.
Abnormal Changes in Gait
Causes
A number of disorders can contribute to dysfunctional or unsafe gait. They particularly include
Neurologic disorders
Musculoskeletal disorders (eg, spinal stenosis)
Common neurologic disorders that affect gait include dementias, movement and cerebellar disorders, and sensory or motor neuropathies. One study compared the smoothness of gait in older adults with and without cognitive impairments and found that older adults with early cognitive impairment were more likely to have substantially reduced smoothness of gait in addition to the known changes in gait speed and stride length (1). In another study, patients with dementia had lower pace scores and abnormal gait rhythm compared with patients with mild cognitive impairment or older adults without any cognitive impairment. Also, gait rhythm was associated with cerebrospinal fluid tau levels (a biomarker in Alzheimer disease [2]).
Manifestations
There are many manifestations of gait abnormality. Some abnormal gait patterns suggest certain causes. Video demonstrations of selected abnormal gaits are available from the NeuroLogic Exam website.
Loss of symmetry of motion and timing between left and right sides usually indicates a disorder. When healthy, the body moves symmetrically; step length, cadence, torso movement, and ankle, knee, hip, and pelvis motion are equal on the right and left sides. A regular asymmetry occurs in patients with unilateral neurologic or musculoskeletal disorders (eg, a limp caused by a painful hip or ankle).
Loss of synchrony can occur. Normal synchrony of gait depends on regular, rhythmic movement and smooth coordination of upper and lower limbs in a cyclic pattern to move the center of gravity forward. Neurologic or musculoskeletal disorders that affect specific components of gait result in loss of synchrony. Unpredictable or highly variable gait cadence, stride length, or stride width indicates breakdown of motor control of gait due to a cerebellar or frontal lobe syndrome or use of multiple psychoactive medications.
Difficulty initiating or maintaining gait may occur. When patients first start walking, their feet may appear stuck to the floor, typically because patients do not shift their weight to one foot to allow the other foot to move forward. This problem may indicate isolated gait initiation failure, Parkinson disease, or frontal or subcortical disease, including the cognitive abnormalities in normal-pressure hydrocephalus. Once gait is initiated, steps should be continuous, with little variability in the timing of the steps. Freezing, stopping, or almost stopping usually suggests a cautious gait, a fear of falling, or a frontal lobe gait disorder. Scuffing the feet is also abnormal (and is a risk factor for tripping); these abnormalities can occur in patients with parkinsonism or weakness and/or numbness of the feet caused by neuropathy.
Retropulsion is falling backwards when initiating gait or while walking. It may occur in patients with frontal gait disorders, parkinsonism, central nervous system syphilis, or progressive supranuclear palsy.
Foot drop causes toe dragging or a steppage gait (ie, exaggerated lift of the leg to avoid catching the toe). It may be secondary to
Anterior tibialis weakness (eg, caused by trauma to the peroneal nerve at the lateral aspect of the knee, a peroneal mononeuropathy usually associated with diabetes, or a compression injury)
Spasticity of calf muscles (gastrocnemius and soleus)
Lowering of the pelvis due to muscle weakness of the proximal muscles on the stance side (particularly the gluteus medius)
Low foot swing (eg, due to reduced knee flexion) may resemble foot drop.
Short step length is nonspecific and may represent a fear of falling or a neurologic or musculoskeletal problem. The side with short step length is usually the healthy side, and the short step is usually due to a problem during the stance phase of the opposite (affected) leg. For example, a patient with a weak or painful left leg spends less time in single stance on the left leg and develops less power to move the body forward, resulting in shorter swing time for the right leg and a shorter right step. The normal right leg has a normal single stance duration, resulting in a normal swing time for the abnormal left leg and a longer step length for the left leg than for the right leg.
Shortened stride length occurs in patients with parkinsonism, whether it is due to idiopathic Parkinson disease, normal-pressure hydrocephalus, vascular disorders, or drugs.
Wide-based gait (increased step width) is determined by observing the patient’s gait on a floor with 12-inch (30-cm) tiles. The gait is considered wide based if the outside of the patient’s feet do not stay within the width of the tile. As gait speed decreases, step width increases slightly. Wide-based gait can be caused by cerebellar disease or bilateral knee or hip disease. Variable step width (lurching to one side or the other) suggests poor motor control, which may be due to frontal or subcortical gait disorders.
Circumduction (moving the foot in an arc rather than a straight line when stepping forward) occurs in patients with pelvic muscle weakness or difficulty bending the knee. Spasticity of the knee extensor muscles is a common cause.
Forward lean can occur in patients with kyphosis, Parkinson disease, or disorders with parkinsonian features associated with dementia (particularly vascular dementia and Lewy body dementia).
Festination is a progressive quickening of steps (usually with forward lean), whereby patients may break into a run to prevent falling forward. Festination occurs most commonly in patients with Parkinson disease and rarely as an adverse effect of dopamine-blocking medications (typical and atypical antipsychotics).
Sideward trunk lean that is consistent or predictable to the side of the stance leg may be a strategy to reduce joint pain due to hip arthritis or, less commonly, knee arthritis (antalgic gait). In a hemiparetic gait, the trunk may lean to the strong side. In this pattern, the patient leans to lift the pelvis on the opposite side to permit the limb with spasticity (inability to flex the knee) to clear the floor during the swing phase.
Irregular and unpredictable trunk instability can be caused by cerebellar, subcortical, or basal ganglia dysfunction.
Deviations from path are strong indicators of motor control deficits.
Arm swing may be reduced or absent in patients with Parkinson disease or vascular dementias. Arm swing disorders may also be adverse effects of dopamine-blocking medications (typical and atypical antipsychotics).
Abnormal changes in gait references
1. Pau M, Mulas I, Putzu V, et al: Smoothness of gait in healthy and cognitively impaired individuals: a study on Italian elderly using wearable inertial sensor. Sensors 20 (12):3577, 2020. doi: 10.3390/s20123577 PMID: 32599872; PMCID: PMC7348719.
2. Muurling M, Rhodius-Meester HFM, Juha Pärkkä J, et al: Gait disturbances are associated with increased cognitive impairment and cerebrospinal fluid au levels in a memory clinic cohort. J Alzheimers 76 (3):1061–1070, 2020. doi: 10.3233/JAD-200225
Evaluation of Gait Disorders
The goal is to determine as many potential contributing factors to gait disorders as possible. A performance-oriented mobility assessment tool may be helpful (see table Performance-Oriented Assessment of Mobility), as may other clinical tests (eg, a screening cognitive examination for patients with gait problems possibly due to frontal lobe syndromes). Identifying which aspects of gait are affected is important.
Performance-Oriented Assessment of Mobility
Component | Findings | Score* | Clinical Meaning |
|---|---|---|---|
Initiation of gait (immediately after being told to go) | Any hesitancy or multiple attempts to start | 0 | Isolated gait initiation failure (stroke or dementia) Frontal gait disorder |
No hesitancy | 1 | ||
Right step length and height (right swing foot) | Does not pass left stance foot with step or does not clear floor completely with step | 0 | Arthritis Foot problem |
Passes left stance foot | 1 | ||
Completely clears floor | 1 | ||
Left step length and height (left swing foot) | Does not pass right stance foot with step or does not clear floor completely with step | 0 | Arthritis Foot problem |
Passes right stance foot | 1 | ||
Completely clears floor | 1 | ||
Step symmetry | Right and left step length not equal (estimated) | 0 | Unilateral Musculoskeletal or focal neurologic deficit |
Right and left step length equal (estimated) | 1 | ||
Step continuity | Stopping or discontinuity between steps | 0 | Frontal gait disorder Fear of falling, frequent in dementia |
Steps appear continuous | 1 | ||
Path (estimated in relation to floor tiles that are 12 inches [30 cm] wide; observed excursion of one foot over about 10 feet [3 meters] of the course) | Marked deviation | 0 | Frontal gait disorder |
Mild to moderate deviation or use of a walking aid | 1 | ||
Straight without a walking aid | 2 | ||
Trunk | Marked sway or use of a walking aid | 0 | Cerebellar, subcortical, and basal ganglia dysfunction Antalgic gait (hip or knee arthritis) |
No sway but flexion of knees, back pain, or arms spread out while walking | 1 | Fear of falling | |
No sway, no flexion, no use of arms, and no use of a walking aid | 2 | ||
Stride width (step width) | Heels wide apart while walking | 0 | Osteoarthritis (hip, knee, or ankle) Cerebellar disease |
Heels almost touching while walking | 1 | ||
* A perfect score is 12. A score of < 10 is usually associated with limitations in mobility-related function. Adapted from Tinetti M: Performance-oriented assessment of mobility problems in elderly patients. Journal of the American Geriatrics Society 34:119–126, 1986; used with permission. | |||
Evaluation is best approached in 4 parts:
Discussing the patient’s complaints, fears, and goals related to mobility
Observing gait with and without an assistive device (if safe)
Assessing all components of gait (see table Performance-Oriented Assessment of Mobility)
Observing gait again with a knowledge of the patient’s gait components
History
In addition to the standard medical history, older patients should be asked about gait-related issues. First, they are asked open-ended questions regarding any difficulty with walking, balance, or both, including whether they have fallen (or fear they might fall). Then specific capabilities are assessed; they include whether patients can go up and down stairs; get in and out of a chair, shower, or tub; and walk as needed to buy and prepare food and do household chores. If they report any difficulties, details of the onset, duration, and progression are sought. History of neurologic and musculoskeletal symptoms and known disorders is important.
Physical examination
A thorough physical examination is done with emphasis on the musculoskeletal examination and the neurologic examination.
Lower-extremity strength is assessed. Proximal muscle strength is tested by having patients get out of a chair without using their arms. Calf strength is measured by having patients face a wall, put their palms on the wall (to assist balance), and rise onto their toes first using both feet and then using one foot at a time. Strength of hip internal rotation is assessed.
Gait assessment
Routine gait assessment can be done by a primary care practitioner; a specialist (eg, neurologist) may be needed for complex gait disorders. Assessment requires a straight hallway without distractions or obstructions and a stopwatch.
Patients should be prepared for the examination. They should be asked to wear pants or shorts that reveal the knees and be informed that several observations may be needed but that they will be allowed to rest if fatigued.
Assistive devices provide stability but also affect gait. Use of walkers often results in a flexed posture and discontinuous gait, particularly if the walker has no wheels. If safe to do so, the clinician should have the patient walk without an assistive device, while remaining close to or walking with the patient with a gait belt for safety. If patients use a cane, the clinician can walk with them on the cane side or take their arm and walk with them. Patients with a suspected peripheral neuropathy should walk touching the clinician’s forearm. If gait improves with this intervention, proprioception from the arm is being used to supplement the missing proprioception from the leg; such patients usually benefit from using a cane, which transmits information about the type of surface or floor to the cane-holding hand.
Balance is assessed by measuring the time patients can stand on both feet in tandem stance (heel to toe) and on one foot (single stance); normal is ≥ 5 seconds.
Gait velocity is measured using a stopwatch. Patients are timed while walking a fixed distance (preferably 6 or 8 meters) at their preferred speed. The test may need to be repeated with patients walking as quickly as possible. Normal gait speed in healthy older adults ranges from 1.1 to 1.5 meter/second.
Cadence is measured as steps/minute. Cadence varies with leg length—about 90 steps/minute for tall adults (1.83 meters [6 feet]) to about 125 steps/minute for short adults (1.5 meters [5 feet]).
Step length can be determined by measuring the distance covered in 10 steps and dividing that number by 10. Because shorter people take shorter steps and foot size is directly related to height, normal step length is 3 foot lengths, and abnormal step length is < 2 foot lengths. A rule of thumb is that if at least 1 foot length is visible between the patient’s steps, step length is normal.
Step height can be assessed by observing the swing foot; if it touches the floor, particularly in the middle of the swing phase, patients may trip. Some patients with fear of falling or a cautious gait syndrome purposefully slide their feet over the floor surface. This gait pattern may be safe on a smooth surface but is a risky strategy when walking on rugs because patients may trip.
Asymmetry or variability of gait rhythm can be detected when clinicians whisper “dum...dum...dum” to themselves with each of the patient’s steps. Some clinicians have a better ear than an eye for gait rhythm.
Testing
Testing is sometimes required.
CT or MRI of the brain is often done, particularly when gait initiation is poor, cadence is chaotic, or patients appear to have a very stiff gait. Imaging is also helpful if patients have associated signs such as cognitive impairment, abnormal coordination, muscle weakness, or sensory abnormalities. These tests may identify abnormalities such as lacunar infarcts, white matter disease, and focal atrophy and can help determine whether additional testing for normal-pressure hydrocephalus should be considered. Imaging of the lumbosacral spine should be considered if patients have unilateral leg weakness (especially if any sensory deficit is present) or have a spastic gait that suggests a myelopathy that may be secondary to spinal stenosis.
Treatment of Gait Disorders
Strength training
Balance training
Assistive devices
Although determining why gait is abnormal is important, interventions to alter gait are not always indicated. A slowed, aesthetically abnormal gait may enable older adults to walk safely and without assistance. However, some treatment interventions can lead to improvement; they include exercise, balance training, and assistive devices (see table Treatment of Gait Disorders).
Treatment of Gait Disorders
Common Problem | Treatment | Comments |
|---|---|---|
Bone structure | ||
Kyphotic posture due to compression fractures of the thoracic spine or poor posture | Thoracic extension, shoulder rotation, chin tuck exercises Osteoporosis treatment to prevent new fractures | Compression fracture can be diagnosed by x-ray, and osteoporosis can be identified by bone mineral density testing. |
Leg length differences | Heel lift | Usually, heel lift correction is not 100%. |
Severe genu varus or valgus | Orthotics, bracing, strengthening of quadriceps | Knee replacement criteria should be reviewed. |
Foot abnormality or pain Hallux valgus (bunion) Loss of longitudinal arch | Orthotics, podiatry care, custom shoes | Testing for plantar neuropathy with monofilament nylon is always done to detect risk of plantar ulceration. |
Joint range of motion | ||
Decreased hip internal rotation | Stretching of adductors, strengthening of abductors | Attempting to increase internal rotation by stretching is not usually effective but may prevent further loss of range of motion. |
Decreased hip extension | Stretching of hip flexors, strengthening of hip extensors | Lying prone, arching back, and extending hip is often recommended. |
Decreased ankle dorsiflexion | Stretching of calf muscles | Height of high-heel shoes is reduced. |
Hallux rigidus (loss of dorsiflexion of the great toe) | Podiatry or orthopedic referral | An orthotic should be considered. |
Muscle power | ||
Weak hip extension | Chair rise exercises | Chair rise test may be helpful in diagnosis. |
Weak knee extension | Chair rise exercises, knee extension with ankle sandbags, squats | Chair rise test may be helpful in diagnosis. |
Weak ankle plantar flexion | Heel raises (using body weight) | To increase resistance during heel raises, patients can wear a weighted vest, backpack, or waist belt; they may need to stabilize themselves against a wall. |
Weak ankle dorsiflexion | Muscle strengthening (eg, toe rises), ankle foot orthotic for footdrop | Patients place sandbag weights over their metatarsals. With their back to the wall for safety, patients rise on their heels (ie, lift toes off the floor). |
Weak hip abduction | Hip abduction with ankle weights, side-lying position on the floor | — |
Sensory systems | ||
Decreased or impaired position sense or balance when eyes are closed during a Romberg test | Appropriate footwear | Vitamin B12 level should be checked. |
Decreased or impaired plantar touch sensation as measured by Semmes-Weinstein monofilaments | Appropriate footwear | Assess for diabetes and alcohol abuse and, if none, consider nerve conduction studies. |
Dizziness or vertigo | — | |
Motor control/balance | ||
Tandem stance or single-leg stance < 5 seconds or turning 360° (both to right and left) requires > 10 steps or patient is unsteady during turning | Balance training involving static and dynamic balance, tai chi, or the equivalent | Vitamin D supplementation 25 mcg (1000 units) once a day reduces risk of falls and fractures for patients in nursing home settings.Vitamin D supplementation 25 mcg (1000 units) once a day reduces risk of falls and fractures for patients in nursing home settings. |
Forward lean Bradykinesia Leg hypertonia Parkinsonian signs | Physical therapy training to maintain or improve motor control/balance | Assess for Parkinson disease. CT or MRI can detect lacunar infarcts, cerebellar changes, and white matter disease. |
Physical and cardiovascular fitness | ||
Dizziness due to postural hypotension | Review of medications for possible cause, compression stockings | |
Fatigue, shortness of breath, inability to walk > 300 m at usual pace | Regular walking program | Patients should be assessed for angina, heart failure, pulmonary disease, and claudication. A 6-minute walking distance is measured. |
Strength training
Frail older adults with mobility problems achieve modest improvements with exercise programs. In older adults with arthritis, walking or resistance training reduces knee pain, and gait may improve.
Resistance exercises can improve strength and gait velocity, especially in frail patients with slowed gait. Two or three training sessions a week are usually needed; resistance exercises consist of 3 sets of 8 to 14 repetitions during each session. The load is increased every week or two until a plateau of strength is reached. Using good form during each exercise is important to reduce soreness or injury.
Leg press machines train all the large muscle groups of the leg and provide back and pelvic support during lifting. However, these machines are not always accessible to older patients. Chair rises with weight vests or weights attached to the waist (waist belts) are an alternative. Instructions are required to reduce the risk of back injury due to excess lumbar lordosis. Step-ups and stair climbing with the same weights are also useful. Ankle plantar flexion can be done with the same weights.
Knee extension machines are effective to strengthen quadriceps. Attaching weights to the ankle strengthens the quadriceps in very frail older adults. The usual starting weight for frail people is 3 kg (7 lb). Resistance for all exercises should be increased every week or after the patient can complete 10 or 12 repetitions until the patient reaches a plateau of strength. Then, exercise is continued at the maximum tolerable weight for maintenance.
Balance training
Many patients with balance deficits benefit from balance training. Good standing posture and static balance are taught first. Patients are then taught to be aware of the location of pressure on their feet and how the location of pressure moves with slow leaning or turning the torso to look to the left or right. Leaning forward (using a wall or counter for support), backward (with a wall directly behind), and to each side is then practiced. The goal is for the patient to be able stand on one leg for 10 seconds.
Dynamic balance training can involve slow movements in single stance, simple tai chi movements, tandem walking, turns while walking, walking backwards, walking over a virtual object (eg, a 15-cm stripe on the floor), slow forward lunges, and slow dance movements. Multicomponent balance training is probably most effective in improving balance.
Nordic walking
Nordic walking is a full-body walking exercise that incorporates adjustable length walking poles. The walking motion incorporates shoulder girdle muscles (pectorals, latissimus dorsi) and triceps muscles and requires greater pelvic rotation as compared with traditional walking, which results in a slightly longer step length and greater velocity. A systematic review of 12 trials of Nordic walking found statistically significant improvements including increased heart rate during walking, increased oxygen consumption, and improvements in 6-minute walk distance, walking speed, upper body muscular endurance, and energy expenditure over the training period (1). Frail walkers need supervision and training to use the walking sticks safely.
Assistive devices
Assistive devices can help maintain mobility and quality of life. New motor strategies must be learned. Physical therapists should be involved in choice of and training with assistive devices.
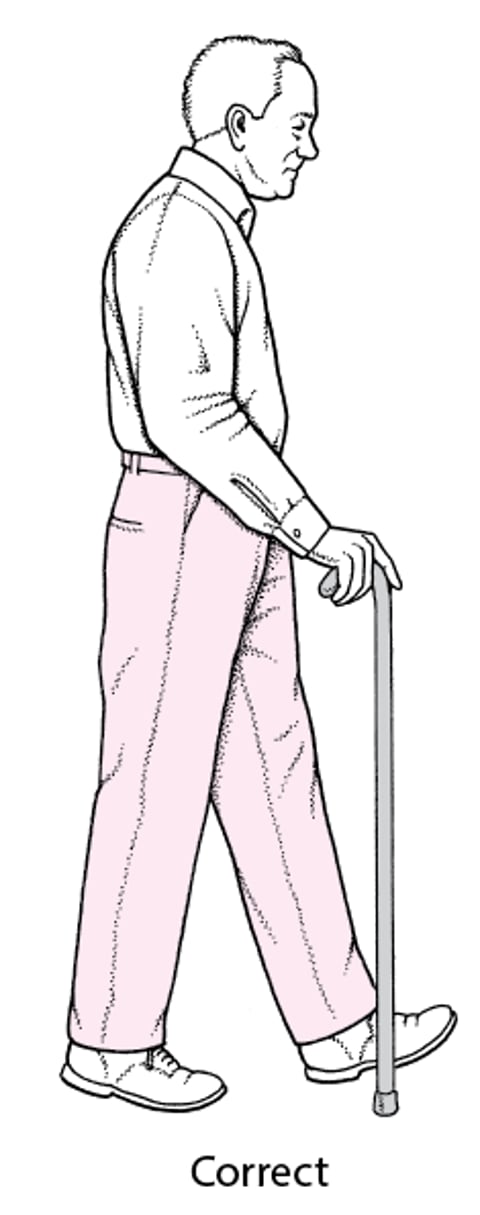
Canes are particularly helpful for patients with pain caused by knee or hip arthritis or with peripheral neuropathy of the feet because a cane transmits information about the type of surface or floor to the cane-holding hand. A quad cane can stabilize the patient but usually slows gait. Canes are usually used on the side opposite the painful or weak leg. Many store-bought canes are too long but can be adjusted to the correct height (see figure Correct Cane Height) by cutting (a wooden cane) or moving the pin settings (an adjustable cane). For maximal support, cane length should be such that patients have their elbow flexed 20 to 30° when holding the cane.
Correct Cane Height
The hand/height of the cane should be at the level of the ipsilateral greater trochanter, which results in about 20 to 30° of elbow flexion. The cane should be held in the hand contralateral to affected hip. The cane can be held on either side for knee pain, based on safety and patient preference. |

Walkers can reduce the force and pain at arthritic joints more than a cane, assuming adequate arm and shoulder strength. Walkers provide good lateral stability and moderate protection from forward falls but do little or nothing to help prevent backward falls for patients with balance problems. When prescribing a walker, the physical therapist should consider the sometimes competing needs of providing stability and maximizing efficiency (energy efficiency) of walking. Four-wheeled walkers with larger wheels and brakes maximize gait efficiency but provide less lateral stability. These walkers have the added advantage of a small seat to sit on if patients become fatigued.
Treatment reference
1. Kocur P, Wiernicka M, Wilski M, et al: Does Nordic walking improves the postural control and gait parameters of women between the age 65 and 74: a randomized trial. J Phys Ther Sci, 27 (12):3733–3737, 2015. doi:10.1589/jpts.27.3733
Prevention of Gait Disorders
Primary prevention: High levels of physical activity have been shown to help maintain mobility, even in patients with disease.
Secondary prevention: Exercise has improved gait and measures of mobility in short- and long-term trials.
The World Health Organization, the American College of Sports Medicine, and the American Heart Association all strongly recommend regular multimodality activity for older adults to maintain health and mobility (1, 2). Regular walking or maintaining a physically active lifestyle is the most important recommendation. The adverse effects of deconditioning and of inactivity cannot be overstated. A regular walking program of 30 minutes/day is the best single activity for maintaining mobility; however, walking on a level surface does not increase strength in a person who is weak. A safe walking course should be recommended, but including an incline (eg, hills) can help maintain leg strength. The use of walking sticks that are adjustable or canes can provide confidence and safety for older adults.
Prevention also includes resistance and balance training. The effects of an active lifestyle on mood and confidence are probably as important as their effect on physiology.
Prevention references
1. Nelson ME, Rejeski WJ, Blair SN, et al: Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 116:1094–1105, 2007. doi: 10.1249/mss.0b013e3180616aa2
2. World Health Organization: Global action plan on physical activity 2018–2030: More active people for a healthier world. Geneva:World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.




