


Lymphatic filariasis is infection with any of 3 species of the nematode (worm) Filarioidea. Acute symptoms include fever, lymphadenitis, lymphangitis, epididymitis, and funiculitis (inflammation of the spermatic cord). Chronic symptoms include abscesses, hyperkeratosis, polyarthritis, hydroceles, lymphedema, and elephantiasis. Tropical pulmonary eosinophilia with bronchospasm, fever, and pulmonary infiltrates is another manifestation of infection. Diagnosis is by detection of microfilariae in blood or lymphatic tissue biopsy specimens, ultrasound visualization of adult worms in lymphatics, or serologic testing. Treatment is with diethylcarbamazine.
Bancroftian filariasis is present in tropical and subtropical areas of Africa, Asia, the Pacific, and the Americas, including Haiti. Brugian filariasis is endemic in South and Southeast Asia.
In 2000, the World Health Organization launched its Global Programme to Eliminate Lymphatic Filariasis. As a result, substantial progress has been made in stopping the spread of infection through large-scale, annual treatment of eligible people in areas where infection is present. As of 2018, approximately 51 million people were infected, which is a decline of 74% since the programme started (1). In 2023, 657 million people in 39 countries required annual preventative treatment to stop the spread of infection (1).
Lymphatic filariasis is caused by Wuchereria bancrofti (approximately 90% of cases), Brugia malayi, or B. timori. Transmission is by mosquitoes. Infective larvae from the mosquito migrate to the lymphatics, where they develop into threadlike adult worms within 6 to 12 months. Gravid adult females produce microfilariae that circulate in blood. W. bancrofti females are approximately 80 to 100 mm long; males are approximately 40 mm long.
(See also Approach to Parasitic Infections and Overview of Filarial Nematode Infections.)


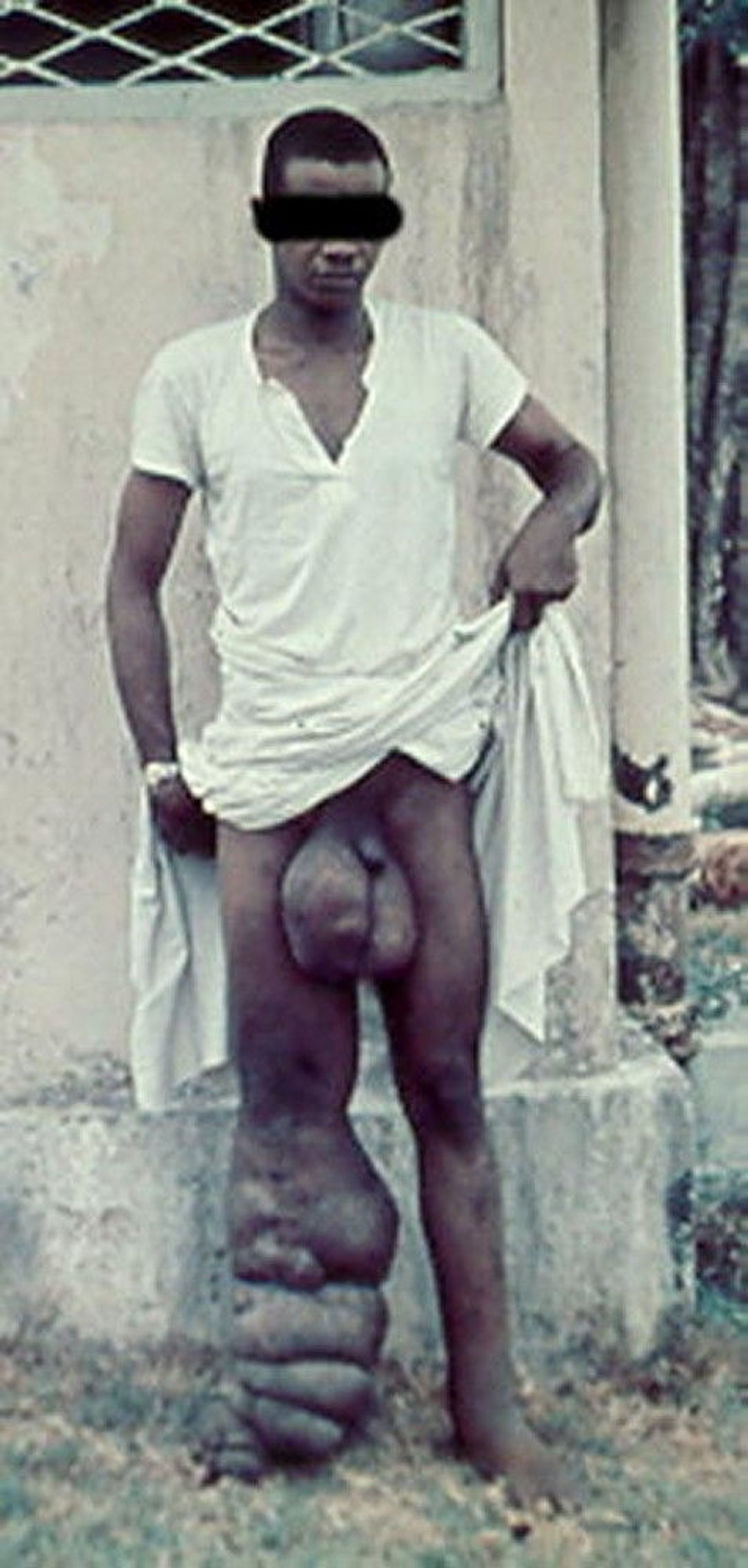
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
General reference
1. World Health Organization (WHO): Lymphatic filariasis. Accessed October 21, 2024.
Symptoms and Signs of Lymphatic Filariasis
Infection can result in microfilaremia without overt clinical manifestations. Symptoms and signs are caused primarily by adult worms. Microfilaremia gradually disappears after people leave the endemic area.
Acute inflammatory filariasis consists of 4- to 7-day episodes (often recurrent) of fever and inflammation of lymph nodes with lymphangitis (termed acute adenolymphangitis) or acute epididymitis and spermatic cord inflammation; secondary bacterial infections are common. Localized involvement of a limb may cause an abscess that drains externally and leaves a scar. Adenolymphangitis episodes usually precede onset of chronic disease by ≥ 2 decades. Acute filariasis is more severe in previously unexposed immigrants to endemic areas than in native residents.
Chronic filarial disease develops insidiously after many years. In most patients, asymptomatic lymphatic dilation occurs, but chronic inflammatory responses to adult worms and secondary bacterial infections may result in chronic lymphedema of the affected body area. Increased local susceptibility to bacterial and fungal infections further contributes to its development. Chronic pitting lymphedema of a lower extremity can progress to elephantiasis (chronic lymphatic obstruction). W. bancrofti can cause hydrocele and scrotal elephantiasis. Other forms of chronic filarial disease are caused by disruption of lymphatic vessels or aberrant drainage of lymph fluid, leading to chyluria and chyloceles.

© Springer Science+Business Media


© Springer Science+Business Media
Extralymphatic signs include chronic microscopic hematuria and proteinuria and mild polyarthritis, all presumed to result from immune complex deposition.
Tropical pulmonary eosinophilia is an uncommon manifestation with recurrent bronchospasm, transitory lung infiltrates, low-grade fever, and marked eosinophilia. It is most likely due to hypersensitivity reactions to microfilariae. Chronic lung involvement can lead to pulmonary fibrosis.
Diagnosis of Lymphatic Filariasis
Microscopic examination of blood samples or lymphatic tissue biopsy
Antigen test for W. bancrofti (available internationally but not in the United States)
Antibody tests
Microscopic detection of microfilariae in blood establishes the diagnosis of lymphatic filariasis. Filtered or centrifuged concentrates of blood are more sensitive than thick blood films. Blood samples must be obtained when microfilaremia peaks—at night in most endemic areas but during the day in many Pacific islands. Viable adult worms can be visualized in dilated lymphatics by ultrasound; their movement has been called the filarial dance.
Several blood tests are available:
Antibody detection: Enzyme immunoassay tests for antifilarial IgG1 and IgG4
Antigen detection: A rapid-format immunochromatographic test for W. bancrofti antigen
Patients with active filarial infection typically have elevated levels of antifilarial IgG4 in the blood. However, there is substantial antigenic cross-reactivity between filariae and other helminths, and a positive serologic test does not distinguish between past and current filarial infection. A rapid diagnostic test for W. bancrofti antigen is used internationally in filariasis elimination programs, but it is not licensed in the United States.
Polymerase chain reaction (PCR) assays for W. bancrofti and B. malayi are available in research laboratories.
Adults of both W. bancrofti and B. malayi species may be identified in biopsy specimens of lymphatic tissue.
Treatment of Lymphatic Filariasis
Diethylcarbamazine
Diethylcarbamazine (DEC) kills microfilariae and a variable proportion of adult worms. In the United States, DEC is available from the Centers for Disease Control and Prevention (CDC) after laboratory confirmation of filariasis.
Pearls & Pitfalls
|
Treatment of acute lymphatic filariasis
DEC 2 mg/kg orally 3 times a day for 12 days has traditionally been used; 6 mg/kg orally once is an alternative. Generally, the 1-day regimen seems to be as effective as the 12-day regimen (1).
Adverse effects of DEC are usually limited and depend on the number of microfilariae in the blood. The most common are dizziness, nausea, fever, headache, and pain in muscles or joints, which are thought to be related to release of filarial antigens.
Before treatment with DEC, patients should be assessed for coinfection with Loa loa (loiasis) or Onchocerca volvulus (onchocerciasis) because DEC can cause serious reactions in patients with these infections. A single dose of albendazole 400 mg orally plus ivermectin 200 mcg/kg orally can be used in areas where onchocerciasis is co-endemic;ivermectin alone does not kill adult worms that cause lymphatic filariasis. DEC should not be used in patients with high circulating Loa loa microfilarial levels due to risk of life-threatening adverse effects including encephalopathy.
Doxycycline 200 mg/day orally for 4 to 6 weeks reduces adult worm burden and lessens pathology in people with mild to moderate disease (2). Doxycycline kills Wolbachia endosymbiont bacteria within filaria, leading to death of adult filarial worms. It can be used alone or in combination with DEC (3) or albendazole (4).
Attacks of acute adenolymphangitis usually resolve spontaneously, but antibiotics may be required to control secondary bacterial infections.
Treatment of chronic lymphedema
Chronic lymphedema requires meticulous skin care, including use of systemic antibiotics to treat secondary bacterial infections; these antibiotics may slow or prevent progression to elephantiasis.
Whether DEC therapy prevents or lessens chronic lymphedema remains controversial. There is some evidence that doxycycline 200 mg/day orally for 4 to 6 weeks can reduce lymphedema, and regular treatment is suggested for patients with advanced disease (5).
Conservative measures, such as elastic bandaging of the affected limb, reduce swelling.
Surgical decompression using nodal-venous shunts to improve lymphatic drainage offers some long-term benefit in extreme cases of elephantiasis. Massive hydroceles can also be managed surgically, but recurrence is common.
Treatment of tropical pulmonary eosinophilia
Tropical pulmonary eosinophilia responds to DEC 2 mg/kg orally 3 times a day for 14 to 21 days, but relapses occur in up to 25% of patients and require additional courses of therapy.
Treatment references
1. Meyrowitsch DW, Simonsen PE, Makunde WH. Mass diethylcarbamazine chemotherapy for control of bancroftian filariasis: comparative efficacy of standard treatment and two semi-annual single-dose treatments. Trans R Soc Trop Med Hyg. 1996;90(1):69-73. doi:10.1016/s0035-9203(96)90484-8
2. Taylor MJ, Makunde WH, McGarry HF, Turner JD, Mand S, Hoerauf A. Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial. Lancet. 2005;365(9477):2116-2121. doi:10.1016/S0140-6736(05)66591-9
3. Mand S, Pfarr K, Sahoo PK, et al. Macrofilaricidal activity and amelioration of lymphatic pathology in bancroftian filariasis after 3 weeks of doxycycline followed by single-dose diethylcarbamazine. Am J Trop Med Hyg. 2009;81(4):702-711. doi:10.4269/ajtmh.2009.09-0155
4. Gayen P, Nayak A, Saini P, et al. A double-blind controlled field trial of doxycycline and albendazole in combination for the treatment of bancroftian filariasis in India. Acta Trop. 2013;125(2):150-156. doi:10.1016/j.actatropica.2012.10.011
5. Mand S, Debrah AY, Klarmann U, et al. Doxycycline improves filarial lymphedema independent of active filarial infection: a randomized controlled trial. Clin Infect Dis. 2012;55(5):621-630. doi:10.1093/cid/cis486
Prevention of Lymphatic Filariasis
Avoiding mosquito bites in endemic areas is the best protection for travelers (eg, by using diethyltoluamide [DEET] on exposed skin, permethrin-impregnated clothing, and bed nets).
The World Health Organization launched the Global Programme to Eliminate Lymphatic Filariasis in 2000 to map endemic areas and treat entire at-risk populations. Several medication regimens are used (1). These regimens decrease microfilaremia and thereby reduce transmission of the parasite by mosquitoes.
Prevention reference
1. World Health Organization: Alternative mass drug administration regimens to eliminate lymphatic filariasis. 2017. Accessed October 28, 2024.
Key Points
Lymphatic filariasis is transmitted by mosquitoes; infective larvae migrate to the lymphatics, where they develop into adult worms.
Adult worms inside the lymphatics can cause inflammation resulting in acute adenolymphangitis or epididymitis or in chronic lymphatic obstruction, which, in some patients, leads to elephantiasis or hydrocele.
Diagnose based on microscopic detection of microfilariae in filtered or centrifuged concentrates of blood that is drawn at the time of day when microfilaremia peaks (varies by species).
Tests for antigen, antibodies, and parasite DNA are alternatives to diagnosis by microscopy.
Treat with diethylcarbamazine (DEC) after excluding coinfection with Loa loa and Onchocerca volvulus.
The WHO global elimination program has reduced transmission in many endemic areas.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.







