



- Human and Mammal Bites
- Alligator, Crocodile, Iguana, and Venomous Lizard Bites
- Snakebites
- Centipede and Millipede Bites
- Insect Stings
- Puss Moth Caterpillar (Asp) Stings
- Mite Bites
- Scorpion Stings
- Spider Bites
- Tick Bites
- Tick Paralysis
- Other Arthropod Bites
- Overview of Marine Bites and Stings
- Cnidaria (Coelenterates, such as Jellyfish and Sea Anemones) Stings
- Mollusk Stings
- Sea Urchin Stings
- Stingray Stings








There are about 3000 snake species throughout the world, and only approximately 15% worldwide and 20% in the United States are dangerous to humans because of venom or toxic salivary secretions (see table Significant Venomous Snakes by Region). At least one species of venomous snake is native to every state in the United States except Alaska, Maine, and Hawaii. Almost all are pit vipers (named because of pitlike depressions on either side of the head, which are heat-sensing organs):
Rattlesnakes (Crotalus)
Copperheads (Agkistrodon)
Cottonmouths or water moccasins (Agkistrodon)
Approximately 45,000 snakebites are reported each year to poison centers in the United States (of which 7000 to 8000 are venomous and cause approximately 5 deaths) (1). Rattlesnakes account for the majority of snakebites and almost all deaths. Copperheads and, to a lesser extent, cottonmouths account for most other venomous bites.
Coral snakes are elapids, which are a different class of snakes characterized by having a neurotoxic venom and imported species (in zoos, schools, snake farms, and amateur and professional collections) account for < 1% of all venomous bites in the United States.

Most fatal envenomations occur in male patients who have deliberately handled the snake; ethanol was a contributing factor in many of the envenomations (Most fatal envenomations occur in male patients who have deliberately handled the snake; ethanol was a contributing factor in many of the envenomations (2). Most bites occur on the upper extremities. Risk factors for death include age extremes, handling of captive snakes (rather than wild encounters), delay in treatment, and undertreatment.
Outside the United States, fatal snakebites are much more common, accounting for > 100,000 deaths yearly (3).
Nonvenomous snakes in the United states include rat snakes, king snakes, and water snakes. Bites from these snakes only require local wound care.
Significant Venomous Snakes by Region
Geographic Region | Snakes |
|---|---|
Africa | Bird snake Boomslang Burrowing asp Gaboon viper Mamba Mole viper Natal black snake Puff adder |
Asia | Asiatic pit vipers King cobra Krait Malaysian pit viper Red-necked keelback Russell’s viper |
Australia | Death adder King brown snake Red-bellied black snake Taipan Tiger snake |
Central and South America | Bushmaster Cantil pit viper Coral snake Fer-de-lance Palm pit viper Rattlesnake |
Europe | Adder Asp viper Blunt nose viper Nose-horned viper Ottoman viper |
Indo-Pacific | Sea kraits Sea snakes |
Middle East | Burrowing asp Egyptian cobra Horned or desert vipers Mole vipers Natal black snake Palestinian viper Saw-scaled viper Sinai desert snake |
North America | Copperhead Coral snakes Cottonmouth (water moccasin) Rattlesnake (eg, diamondback, sidewinder, timber, prairie, Mojave) |
References
1. U.S. Centers for Disease Control and Prevention (CDC); National Institute for Occupational Safety and Health (NIOSH). Venomous Snakes at Work. Accessed December 17, 2024.
2. Greene SC, Folt J, Wyatt K, Brandehoff NP. Epidemiology of fatal snakebites in the United States 1989-2018. Am J Emerg Med. 2021;45:309-316. doi:10.1016/j.ajem.2020.08.083
3. World Health Organization (WHO). Snakebite Envenoming. Accessed December 12, 2024.
Pathophysiology of Snakebites
Snake venoms are complex substances, chiefly proteins, with enzymatic activity. Although enzymes play an important role, the lethal properties of venom are caused by certain smaller polypeptides. Most venom components appear to bind to multiple physiologic receptors, and attempts to classify venom as toxic to a specific system (eg, neurotoxin, hemotoxin, cardiotoxin, myotoxin) are misleading and can lead to errors in clinical judgment.
Pit vipers
The complex venom of most North American pit vipers has local effects as well as systemic effects such as coagulopathy. Effects may include
Local tissue damage, causing edema and ecchymosis
Vascular endothelial damage
Hemolysis
A disseminated intravascular coagulation (DIC)–like (defibrination) syndrome
Pulmonary, cardiac, renal, and neurologic defects
Venom alters capillary membrane permeability, causing extravasation of electrolytes, albumin, and red blood cells through vessel walls into the envenomated site. This process may occur in the lungs, myocardium, kidneys, peritoneum, and, rarely, the central nervous system. Common clinical syndromes secondary to severe pit viper envenomation include the following:
Edema: Initially, edema, hypoalbuminemia, and hemoconcentration occur.
Hypovolemia: Later, blood and fluids pool in the microcirculation, causing hypotension, lactic acidemia, shock, and, in severe cases, multisystem organ failure. Effective circulating blood volume falls and may contribute to cardiac and renal failure.
Bleeding: Clinically significant thrombocytopenia (platelet count < 20 × 109 cells/L [20,000 cells/mcL]) is common in severe rattlesnake bites and may occur alone or with other coagulopathies. Venom-induced intravascular clotting may trigger a DIC-like syndrome, resulting in bleeding.
Renal failure: Renal failure may result from severe hypotension, hemolysis, rhabdomyolysis, nephrotoxic venom effects, or a DIC-like syndrome. Proteinuria, hemoglobinuria, and myoglobinuria may occur in reaction to severe rattlesnake bites.


Photo courtesy of Thomas Arnold, MD.
The venom of most North American pit vipers causes very minor changes in neuromuscular conduction, except for Mojave and eastern diamondback rattlesnake venom, which may cause serious neurologic deficits (eg, muscle weakness, respiratory depression).
ElapidsC


Photo courtesy of Mike Cardwell (Victorville, CA).
Coral snakes are the most common elapids found in the United States. Other elapids include cobras and mambas. Venom of these snakes contains primarily neurotoxic components, which cause a presynaptic neuromuscular blockade, potentially causing respiratory paralysis. The lack of significant proteolytic enzyme activity accounts for the paucity of symptoms and signs at the bite site.
Symptoms and Signs of Snakebites
A snakebite, whether from a venomous or nonvenomous snake, usually causes terror, often with autonomic manifestations (eg, nausea, vomiting, tachycardia, diarrhea, diaphoresis), which may be difficult to distinguish from systemic manifestations of envenomation.
Nonvenomous snakebites cause only local injury, usually pain and 2 to 4 rows of scratches from the snake’s upper jaw at the bite site.
Symptoms and signs of envenomation may be local, systemic, or a combination, depending on degree of envenomation and species of snake. Anaphylaxis can occur, particularly in snake handlers who have been previously sensitized.
Pit vipers
Approximately 25% of pit viper bites are dry (venom is not deposited), and no systemic symptoms or signs develop.
Local signs include ≥ 1 fang marks and scratches. Oozing from the wound suggests envenomation. If envenomation has occurred, edema and erythema at the bite site and in adjacent tissues occur, usually within 30 to 60 minutes. Edema can progress rapidly and may involve the entire extremity within hours. Lymphangitis and enlarged, tender regional lymph nodes may develop; temperature increases over the bite area. In moderate or severe envenomations, ecchymosis is common and may appear at and around the bite site within 3 to 6 hours. Ecchymosis is most severe after bites by
Eastern and western diamondbacks
Cottonmouths
Prairie, Pacific, and timber rattlesnakes
The skin around the bite may appear tense and discolored. Bullae—serous, hemorrhagic, or both—usually appear at the bite site within 8 hours. Edema resulting from North American rattlesnake envenomations may be severe but is usually limited to dermal and subcutaneous tissues, although severe envenomation rarely causes edema in subfascial tissue, causing compartment syndrome (defined as compartment pressures ≥ 30 mm Hg for > 1 hour, or as < 30 mm Hg below the diastolic pressure). Necrosis around the bite site is common after rattlesnake envenomations. Most venom effects on soft tissues peak within 2 to 4 days.
Ecchymosis is less common after copperhead and Mojave rattlesnake bites.
Systemic manifestations of envenomation can include nausea, vomiting, diarrhea, diaphoresis, anxiety, confusion, spontaneous bleeding, fever, chest pain, difficulty breathing, paresthesias, hypotension, and shock. Some patients with rattlesnake bites experience a rubbery, minty, or metallic taste in their mouth. The venom of most North American pit vipers causes minor neuromuscular conduction changes, including generalized weakness and paresthesias and muscle fasciculations. Some patients have alterations in mental status. Venom of Mojave and eastern diamondback rattlesnakes may cause serious neurologic deficits, including respiratory depression.
Anaphylaxis can cause systemic symptoms immediately.
Rattlesnake envenomations may induce various coagulation abnormalities, including thrombocytopenia, prolongation of prothrombin time (PT, measured by the INR [international normalized ratio]) or activated partial thromboplastin time (PTT), hypofibrinogenemia, elevated fibrin degradation products, or a combination of these findings, causing a disseminated intravascular coagulation (DIC)-like syndrome. Thrombocytopenia is usually the first manifestation and may be asymptomatic or, in the presence of a multicomponent coagulopathy, cause spontaneous bleeding. Patients with coagulopathy typically hemorrhage from the bite site or from venipuncture sites or mucous membranes, with epistaxis, gingival bleeding, hematemesis, hematochezia, hematuria, or a combination. A rise in hematocrit (Hct) is an early finding secondary to edema and hemoconcentration. Later, Hct may fall as a result of fluid replacement and blood loss due to DIC-like syndrome. In severe cases, hemolysis may cause a rapid fall in Hct.
Elapids
Pain and swelling may be minimal or absent and are often transitory. The absence of local symptoms and signs may erroneously suggest a dry bite, producing a false sense of security for both patient and clinician.
Pearls & Pitfalls
|
Weakness of the bitten extremity may become evident within several hours. Systemic neuromuscular manifestations may be delayed for 12 hours and include weakness and lethargy; altered sensorium (eg, euphoria, drowsiness); cranial nerve palsies causing ptosis, diplopia, blurred vision, dysarthria, and dysphagia; increased salivation; muscle flaccidity; and respiratory distress or failure. Once the neurotoxic venom effects manifest, they are difficult to reverse and may last 3 to 6 days. Untreated, respiratory muscle paralysis may be fatal.
Diagnosis of Snakebites
Identification of the snake
Grading severity of envenomation
Definitive diagnosis of a snakebite is aided by positive identification of the snake and clinical manifestations of envenomation. History should include the time of bite, description of the snake, type of field therapy, underlying medical conditions, allergy to horse or sheep products, and history of previous venomous snakebites and therapy. A complete physical examination should be done. A marker should be used to indicate the leading edge of edema on the affected limb or area, and the time the mark was made should be recorded.
Snakebites should be assumed to be venomous until proved otherwise by clear identification of the species or by a period of observation.
Snake identification
Patients often cannot recall details of the snake’s appearance. Pit vipers and nonvenomous snakes can be distinguished by some physical features (see figure Identifying Pit Vipers). Consultation with a zoo, an aquarium, or a poison center (eg, in the Unites States 1-800-222-1222) can help in the identification of snake species.
Identifying Pit Vipers
Pit vipers have the following features, which help differentiate them from nonvenomous snakes:
|

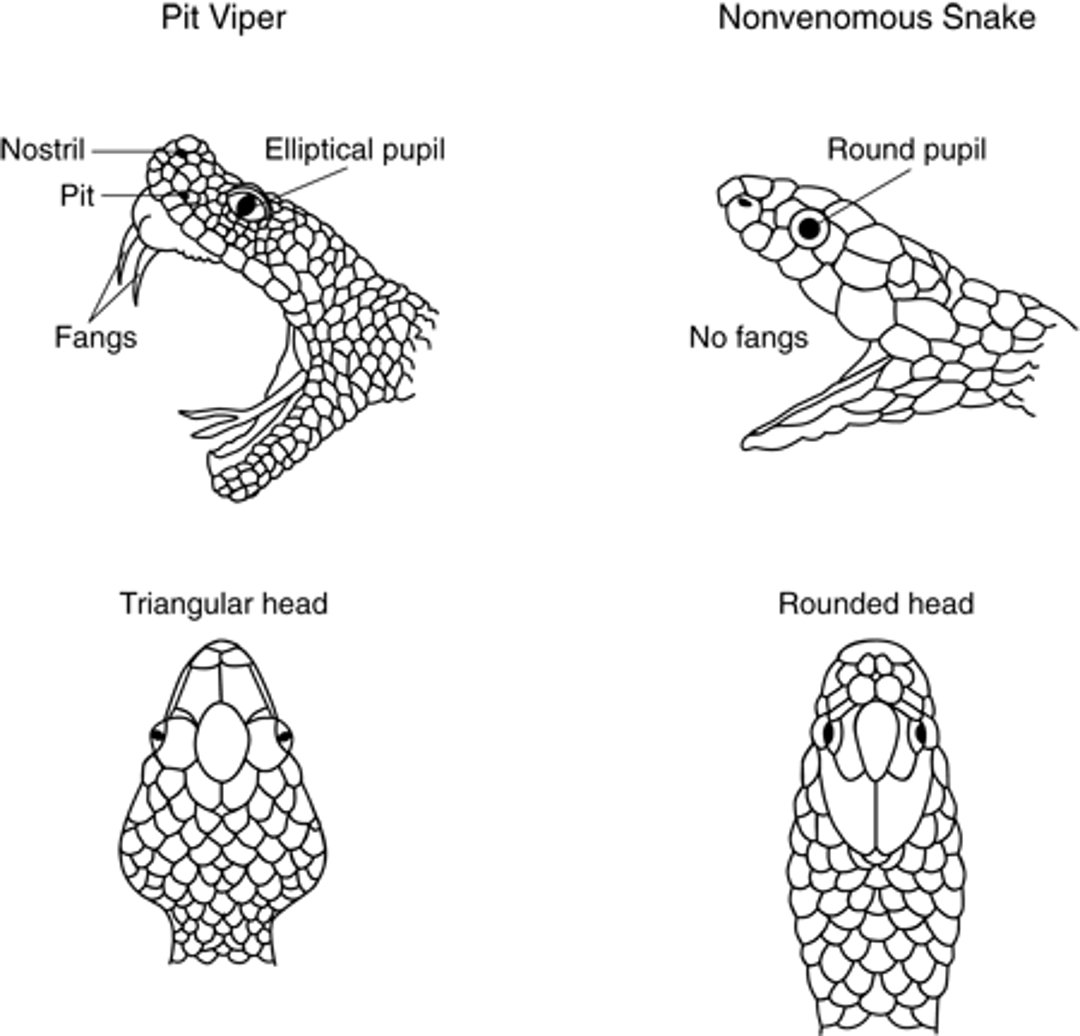

Image courtesy of Edward J. Wozniak, DVM, PhD via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of CDC/James Gathany via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of CDC/James Gathany via the Public Health Image Library of the Centers for Disease Control and Prevention.
Coral snakes in the United States have round pupils and black snouts but lack facial pits. They have blunt or cigar-shaped heads and alternating bands of red, yellow (cream), and black, often causing them to be mistaken for the common nonvenomous scarlet king snake, which has alternating bands of red, black, and yellow. The distinguishing feature in the coral snake is that the red bands are adjacent to only yellow bands, not black bands (“red on yellow, kill a fellow; red on black, venom lack”). Coral snakes have short, fixed fangs and inject venom through successive chewing movements.
Fang marks are suggestive but not conclusive; rattlesnakes may leave single or double fang marks or other teeth marks, whereas bites by nonvenomous snakes usually leave multiple superficial teeth marks. However, the number of teeth marks and bite sites may vary because snakes may strike and bite multiple times.
A dry pit viper bite is diagnosed when no symptoms or signs of envenomation appear within 8 hours after the bite.
Severity of envenomation
Severity of envenomation depends on the following:
Size and species of the snake (rattlesnakes > cottonmouths > copperheads)
Amount of venom injected per bite (cannot be determined by history)
Number of bites
Location and depth of the bite (eg, envenomation in bites to the head and trunk tends to be more severe than in bites to the extremities)
Age, size, and health of the patient
Time elapsed before treatment
Patient’s susceptibility (response) to the venom
Severity of envenomation can be graded as minimal, moderate, or severe based on local findings, systemic symptoms and signs, coagulation parameters, and laboratory results (see table Severity of Pit Viper Envenomation). Grading should be determined by the most severe symptom, sign, or laboratory finding within 8 hours from the time of the bite.
Envenomation may progress rapidly from minimal to severe and must be reassessed continually.
If systemic symptoms begin immediately, anaphylaxis should be assumed.
Severity of Pit Viper Envenomation
Grade | Description |
|---|---|
Minimal | Changes at bite site only No systemic symptoms or signs or abnormal laboratory findings |
Moderate | Changes extending beyond the bite site Non–life-threatening systemic symptoms and signs (eg, nausea, vomiting, paresthesias) Mildly abnormal coagulation or laboratory changes without clinically significant bleeding |
Severe | Changes involving the entire extremity Severe systemic symptoms and signs (eg, hypotension, dyspnea, shock) Markedly abnormal coagulation and laboratory changes with or without clinically significant bleeding |
Data from Lavonas EJ, Ruha AM, Banner W, et al. Unified treatment algorithm for the management of crotaline snakebite in the United States: results of an evidence-informed consensus workshop. BMC Emerg Med. 2011;11:2. Published 2011 Feb 3. doi:10.1186/1471-227X-11-2 | |
Treatment of Snakebites
First aid (clean the wound and stop the bleeding)
Supportive care
Antivenom
Wound care
Bites from nonvenomous snakes require only local wound care. However, if the patient is not certain of the snake type, observation may be required to determine whether envenomation has occurred.
General approach
Treatment of snakebites begins immediately, before patients are moved to a medical facility.
In the field, patients should move or be moved beyond the snake’s striking distance. They should avoid exertion and be reassured, kept warm, and transported rapidly to the nearest medical facility. A bitten extremity should be wrapped loosely and immobilized in a functional position at about heart level, and all rings, watches, and constrictive clothing should be removed. Pressure immobilization to delay systemic absorption of venom (eg, by wrapping tourniquets or other fabric bandages around the limb) may be appropriate for coral snake bites but is not recommended in the United States, where most bites are from pit vipers; pressure immobilization may cause arterial insufficiency and necrosis.
First responders should support airway and breathing, administer oxygen, and establish IV access in an unaffected extremity while transporting patients. All other out-of-hospital interventions (eg, tourniquets, topical preparations, any form of wound suction with or without incision, cryotherapy, electrical shock) are of no proven benefit, may be harmful, and may delay appropriate treatment. However, tourniquets that are already placed, unless causing limb-threatening ischemia, should remain in place until patients are transported to the hospital and envenomation is excluded or definitive treatment is initiated.
Pearls & Pitfalls
|
Serial assessment and testing begin in the emergency department. Outlining the leading margin of local edema with an indelible marker every 15 to 30 minutes can help clinicians assess progression of local envenomation. Extremity circumference should be measured on arrival and at regular intervals until local progression subsides. All but trivial pit viper bites require
A baseline complete blood count (including platelets)
Coagulation profile (eg, prothrombin time, partial thromboplastin time, fibrinogen)
Measurement of fibrin degradation products
Urinalysis
Measurement of serum electrolytes, blood urea nitrogen (BUN), and creatinine (1)
For moderate and severe envenomations, patients require blood typing and cross-matching, ECG, chest radiograph, and creatine kinase tests, as governed by the patient’s status, often as frequently as every 4 hours for the first 12 hours and then daily. In the management of patients with coral snake bites, neurotoxic venom effects necessitate monitoring of oxygen saturation and baseline and serial pulmonary function tests (ie, peak flow, vital capacity).
Duration of close observation for all patients with pit viper bites should be at least 8 hours. Patients without evidence of envenomation after 8 hours may be sent home after adequate wound care. Patients with coral snake bites should be monitored closely for at least 12 hours in case respiratory paralysis develops. Envenomation initially assessed as mild may progress to severe within several hours.
Supportive care may include respiratory support, benzodiazepines for anxiety relief and sedation, opioids for pain, and fluid replacement and vasopressor support for shock. Transfusions (eg, packed red blood cells, fresh frozen plasma, cryoprecipitate, platelets) may be required but should not be given before patients have received adequate quantities of neutralizing antivenom because most coagulopathies respond to sufficient quantities of neutralizing antivenom. Suspected anaphylaxis (eg, with immediate onset of systemic symptoms) is treated with standard measures, including epinephrine. (eg, packed red blood cells, fresh frozen plasma, cryoprecipitate, platelets) may be required but should not be given before patients have received adequate quantities of neutralizing antivenom because most coagulopathies respond to sufficient quantities of neutralizing antivenom. Suspected anaphylaxis (eg, with immediate onset of systemic symptoms) is treated with standard measures, including epinephrine.Tracheostomy may be needed if trismus, laryngeal spasm, or excessive salivation is present.
Antivenom
Along with aggressive supportive care, antivenom is the mainstay of treatment for patients with anything more than the mildest envenomation grade.
For pit viper envenomation, the mainstay of treatment in the United States is an ovine-derived Crotalidae polyvalent immune FAb antivenom (purified FAb fragments of IgG harvested from pit viper venom–immunized sheep) (, the mainstay of treatment in the United States is an ovine-derived Crotalidae polyvalent immune FAb antivenom (purified FAb fragments of IgG harvested from pit viper venom–immunized sheep) (1). The effectiveness of this antivenom is time and dose related; it is most effective in preventing venom-induced tissue damage when given as soon as possible. It is less effective if delayed but can reverse coagulopathies and be effective even when started 24 hours after envenomation. Crotalidae polyvalent immune FAb is very safe, although it can still cause acute (cutaneous or anaphylactic) reactions and delayed hypersensitivity reactions (). The effectiveness of this antivenom is time and dose related; it is most effective in preventing venom-induced tissue damage when given as soon as possible. It is less effective if delayed but can reverse coagulopathies and be effective even when started 24 hours after envenomation. Crotalidae polyvalent immune FAb is very safe, although it can still cause acute (cutaneous or anaphylactic) reactions and delayed hypersensitivity reactions (serum sickness). Serum sickness develops in up to 16% of patients 1 to 3 weeks after administration of the FAb product.
A loading dose of 4 to 12 vials of reconstituted Crotalidae polyvalent immune FAb diluted in 250 mL of normal saline should be infused slowly at 20 to 50 mL/hour for the first 10 minutes; then, if no adverse reactions occur, the remainder is infused over the next hour. The same dose can be repeated 2 times as needed to achieve initial control of symptoms, reverse coagulopathies, and correct physiologic parameters. In children, the dose is not decreased (eg, based on weight or size). Measuring the circumference of the involved extremity at 3 points proximal to the bite and measuring the advancing border of edema every 15 to 30 minutes can guide decisions about the need for additional doses. Once control is achieved, a 2-vial dose in 250 mL saline is given at 6, 12, and 18 hours to prevent recurrence of limb swelling and other venom effects.A loading dose of 4 to 12 vials of reconstituted Crotalidae polyvalent immune FAb diluted in 250 mL of normal saline should be infused slowly at 20 to 50 mL/hour for the first 10 minutes; then, if no adverse reactions occur, the remainder is infused over the next hour. The same dose can be repeated 2 times as needed to achieve initial control of symptoms, reverse coagulopathies, and correct physiologic parameters. In children, the dose is not decreased (eg, based on weight or size). Measuring the circumference of the involved extremity at 3 points proximal to the bite and measuring the advancing border of edema every 15 to 30 minutes can guide decisions about the need for additional doses. Once control is achieved, a 2-vial dose in 250 mL saline is given at 6, 12, and 18 hours to prevent recurrence of limb swelling and other venom effects.
Crotalidae immune F(ab')2 (equine) is a horse-derived antivenom consisting of reconstituted Crotalidae immune Fab2 fragments. It is used to treat North American rattlesnake bites in adults and children. Crotalidae immune F(ab')2 (equine) is a horse-derived antivenom consisting of reconstituted Crotalidae immune Fab2 fragments. It is used to treat North American rattlesnake bites in adults and children.
Pearls & Pitfalls
|
Pit viper species may affect dose. Cottonmouth, copperhead, and pygmy rattlesnake envenomations may require smaller doses of antivenom. However, antivenom should not be withheld based on the species of snake and should be given based on envenomation grading regardless of the species.
For coral snake envenomation, equine-derived polyvalent coral snake antivenom (coral snake antivenin) is given for adults and children., equine-derived polyvalent coral snake antivenom (coral snake antivenin) is given for adults and children.
Antivenom pretreatment precautions should be considered for patients with known hypersensitivity to the specific antivenom being considered or to horse or sheep serum and those with a history of asthma or multiple allergies. In such patients, if the envenomation is considered life or limb threatening, H1 and H2 blockers should be given before antivenom in a critical care setting equipped to treat anaphylaxis. Early anaphylactoid reactions to antivenom have been noted and usually result from too-rapid infusion; treatment is to temporarily stop the infusion and give epinephrine, H1 and H2 blockers, and IV fluid, depending on severity. Usually, antivenom can be resumed after diluting the antivenom further and infusing it at a slower rate. . Early anaphylactoid reactions to antivenom have been noted and usually result from too-rapid infusion; treatment is to temporarily stop the infusion and give epinephrine, H1 and H2 blockers, and IV fluid, depending on severity. Usually, antivenom can be resumed after diluting the antivenom further and infusing it at a slower rate.
Serum sickness may develop, manifesting 7 to 21 days after treatment as fever, rash, malaise, urticaria, arthralgia, and lymphadenopathy. Treatment is H1 blockers and a tapering course of oral corticosteroids.
Adjunctive measures
Patients should receive tetanus prophylaxis (toxoid and sometimes Ig) as indicated by their history (see table Tetanus Prophylaxis in Routine Wound Management). Snakebites rarely become infected, and antibiotics are indicated only for patients with clinical evidence of infection. If necessary, options include a first-generation cephalosporin (eg, oral cephalexin, IV cefazolin) or a broad-spectrum penicillin (eg, oral amoxicillin/clavulanic acid, IV ampicillin/sulbactam). Subsequent antibiotic choices should be based on culture and sensitivity results from wound cultures.). Snakebites rarely become infected, and antibiotics are indicated only for patients with clinical evidence of infection. If necessary, options include a first-generation cephalosporin (eg, oral cephalexin, IV cefazolin) or a broad-spectrum penicillin (eg, oral amoxicillin/clavulanic acid, IV ampicillin/sulbactam). Subsequent antibiotic choices should be based on culture and sensitivity results from wound cultures.
Wound care for bites is similar to that for other puncture wounds. The area is cleaned and dressed. For limb bites, the extremity is splinted in a functional position and elevated. Wounds should be examined and cleaned daily and covered with a sterile dressing. Blebs, bloody vesicles, or superficial necrosis should be surgically debrided between days 3 and 10, in stages if needed. Sterile whirlpool sessions may be indicated for wound debridement and physical therapy. Fasciotomy (ie, for compartment syndrome) is rarely indicated and should be considered only when compartment pressure is ≥ 30 mm Hg for > 1 hour or < 30 mm Hg below the diastolic pressure, causes severe vascular compromise, is unresponsive to limb elevation and mannitol 1 to 2 g/kg IV, and appropriate doses of antivenom have failed. Massive edema alone is 30 mm Hg for > 1 hour or mannitol 1 to 2 g/kg IV, and appropriate doses of antivenom have failed. Massive edema alone isnot an indication for fasciotomy. Joint motion, muscle strength, sensation, and limb girth should be evaluated within 2 days after the bite. Contractures can be prevented by interrupting immobilization with frequent periods of gentle exercise, progressing from passive to active.
Regional poison centers and zoos are excellent resources when dealing with snakebites, including those by nonnative snakes. These facilities maintain a list of physicians trained in snake identification and snakebite care as well as the Antivenom Index, published and periodically updated by the American Zoo and Aquarium Association and the American Association of Poison Control Centers. This index catalogs the location and number of vials of antivenom available for all native venomous snakes and most exotic species. In the United States a national help line is available at 1-800-222-1222.
Treatment reference
1. Lavonas EJ, Ruha AM, Banner W, et al. Unified treatment algorithm for the management of crotaline snakebite in the United States: results of an evidence-informed consensus workshop. BMC Emerg Med. 2011;11:2. Published 2011 Feb 3. doi:10.1186/1471-227X-11-2
Key Points
In the United States, common venomous snakes include rattlesnakes, copperheads, and cottonmouths (all pit vipers), but rattlesnakes account for most bites and almost all deaths.
Pit viper envenomation can cause local effects (eg, pain, progressive swelling, ecchymosis) and systemic effects (eg, vomiting, diaphoresis, confusion, bleeding, fever, chest pain, dyspnea, paresthesias, hypotension).
Features that can help differentiate pit vipers from nonvenomous snakes include an elliptical pupil, a triangular head, retractable fangs, heat-sensing pits between the eyes and nose, and a single row of subcaudal plates extending from the anal plate on the underside of the tail.
In the field, remove the patient out of striking distance from the snake, arrange rapid transport, wrap a bitten limb loosely, immobilize it in a position at about heart level, and remove constricting devices such as rings and watches; do not incise bite wounds or apply tourniquets.
Monitor patients with pit viper bites serially for at least 8 hours, longer if any findings suggest envenomation.
Treat wounds and symptoms, and consult a poison center.
Give antivenom early.







