



Blunt facial trauma can fracture the jaw and other bones of the midface. Symptoms depend on the location of the fracture. A dental x-ray or CT is diagnostic. Treatment may include surgery and/or external fixation.


Fractures of the lower jaw (mandible) are suspected in patients with post-traumatic malocclusion or focal swelling and tenderness over a segment of the mandible. Other clues include defects (stepoff) of the dental occlusal surface, alveolar ridge disruptions, and anesthesia in the distribution of the inferior alveolar or mental nerve. Some fractures result in palpable instability. Fractures of the mandibular condyle usually cause preauricular pain, swelling, and limited opening of the mouth (trismus). With a unilateral condylar fracture, the jaw deviates to the affected side when the mouth is opened.
Fractures of the midface, which includes the area from the superior orbital rim to the maxillary teeth, can cause irregularity in the smooth contour of the cheeks, malar eminences, zygomatic arch, or orbital rims. The Le Fort classification (see figure Le Fort Classification of Midface Fractures) can be used to describe midface fractures. Traumatic malocclusion and upper alveolar ridge fractures may suggest a maxillary fracture that involves the occlusal surface.
Orbital floor fracture is suggested by infraorbital nerve anesthesia, enophthalmos, or diplopia. An injury near the orbit requires an eye examination that includes at minimum an assessment of visual acuity, pupils, and extraocular movements (see also Blowout Fracture).
Zygomatic arch fracture is suggested by trismus and a defect on palpation of the zygomatic arch. A depression on the ipsilateral cheek may or may not be visible initially due to swelling.
Brain injury and fractured cervical vertebrae are possible when trauma has been severe enough to fracture facial bones. In major impact injuries, hemorrhage and edema due to a facial fracture may compromise the airway.
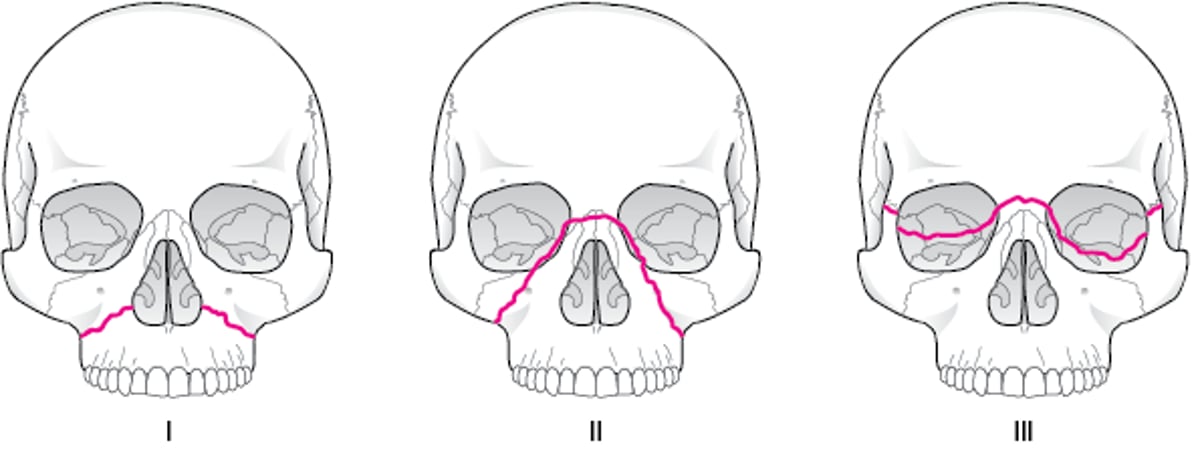
Le Fort Classification of Midface Fractures
I: Only the lower maxilla; II: The infraorbital rim; III: Complete detachment of the midface from the skull (craniofacial dissociation). |

Diagnosis of Mandibular and Midface Fractures
X-ray and/or CT

SCIENCE PHOTO LIBRARY


DU CANE MEDICAL IMAGING LTD/SCIENCE PHOTO LIBRARY
A panoramic dental x-ray is preferred for an isolated mandibular fracture. Fine-cut CT (1-mm slices) is done in axial and coronal planes to diagnose facial fractures.
Treatment of Mandibular and Midface Fractures
Fracture management
Sometimes endotracheal intubation, antibiotics
An oral endotracheal airway may be required to maintain airway patency in patients with hemorrhage, edema, or significant tissue disruption. Definitive facial fracture management is complex and may include internal fixation.
Tooth socket fractures
Fractures through a tooth socket are open fractures. They require antibiotic prophylaxis (typically with a broad-spectrum antibiotic that is particularly effective against anaerobes, such as penicillin) given orally as a liquid or parenterally.
Mandible fractures
For a fractured mandible, treatment ranges from soft diet alone to maxillomandibular fixation (wiring the jaw shut), rigid open fixation, or both. If fixation is available within the first few hours after injury, closure of any lip or oral lacerations should be delayed until the fracture has been reduced. For maxillomandibular fixation, metal bars (arch bars) are attached to the buccal surface of the upper and lower teeth and then wired to each other after correct occlusion has been established. Patients with maxillomandibular fixation should always carry wire cutters in case of vomiting. Early mobilization is usually preferred, although fixation may need to last several weeks. Eating is restricted to liquids, pureed foods, and supplements.
Because only part of the teeth surfaces can be brushed, control of plaque formation, infection, and halitosis is accomplished using a 60-second rinse with 30 mL of chlorhexidine 0.12% every morning and evening. Jaw-opening exercises usually help restore function after fixation is discontinued.Because only part of the teeth surfaces can be brushed, control of plaque formation, infection, and halitosis is accomplished using a 60-second rinse with 30 mL of chlorhexidine 0.12% every morning and evening. Jaw-opening exercises usually help restore function after fixation is discontinued.
Pearls & Pitfalls
|
Condylar fractures may require only 2 to 3 weeks of maxillomandibular fixation, followed by a soft diet. However, severely displaced, bilaterally fractured condyles may require open reduction and fixation. Condylar fractures in children should not be rigidly immobilized because ankylosis and abnormal facial development may result. Flexible (elastic) fixation for 5 to 10 days is usually sufficient.
Midface fractures
Fractures of the midface are treated surgically if they cause malocclusion, enophthalmos, diplopia, infraorbital nerve anesthesia, or unacceptable cosmetic deformity. Surgical treatment usually consists of internal stabilization using fine screws and plates. Surgery can often be delayed until swelling subsides, particularly if the indication for surgery is not clear. However, if surgery is required, it is best done within 14 days of injury because after this time, bone callus can make reduction difficult.







