



- Overview of Fractures
- Pediatric Physeal (Growth Plate) Fractures
- Clavicle Fractures
- Proximal Humeral Fractures
- Distal Humeral Fractures
- Radial Head Fractures
- Ulnar and Radial Shaft Fractures
- Distal Radius Fractures
- Isolated Olecranon Fractures
- Scaphoid (Navicular) Fractures
- Metacarpal Neck Fractures
- Fingertip Fractures
- Vertebral Compression Fractures
- Pelvic Fractures
- Hip Fractures
- Femoral Shaft Fractures
- Ankle Fractures
- Calcaneal Fractures
- Fracture-Dislocation of the Midfoot (Lisfranc Injury)
- Fractures of the 5th Metatarsal Bone
- Toe Fractures
- Compartment Syndrome
Distal humeral fractures usually result from a fall on an outstretched arm or direct force; they may be associated with neurovascular injury.


(See also Overview of Fractures.)
Distal humeral fractures are common among children aged 3 to 11 years. The usual injury mechanism is a fall on an outstretched arm with the elbow extended or direct force, often causing posterior displacement or angulation.
The brachial artery or median or radial nerve may be damaged, particularly when the fracture is posteriorly displaced or angulated. Neurovascular injury sometimes leads to compartment syndrome of the forearm, which can cause Volkmann ischemic contracture (a flexion contracture at the wrist resulting in a clawlike hand deformity because of ischemia to the forearm). Fractures are usually intra-articular, causing hemarthrosis.
Symptoms and Signs of Distal Humeral Fractures
The elbow area is painful and swollen, and the elbow's range of motion is limited.
Ecchymoses over the anterior medial forearm suggest brachial artery injury.
Diagnosis of Distal Humeral Fractures
Anteroposterior and lateral radiographs
A fracture line may not be visible, but other radiograph findings may suggest fracture. They include
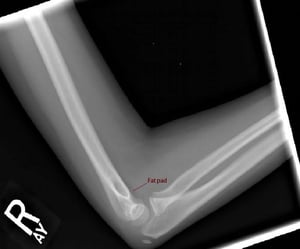
Posterior fat pad
Anterior fat pad (sail sign)
Abnormal anterior humeral line
Abnormal radiocapitellar line
A posterior fat pad on a true lateral radiograph of the elbow is always abnormal; this finding is specific for joint effusion but not highly sensitive.
A displaced anterior fat pad may indicate joint effusion but is not specific.
However, if a posterior fat pad is seen or if a large anterior fat pad (sail sign) is present, an occult fracture should be assumed and should be treated as such.
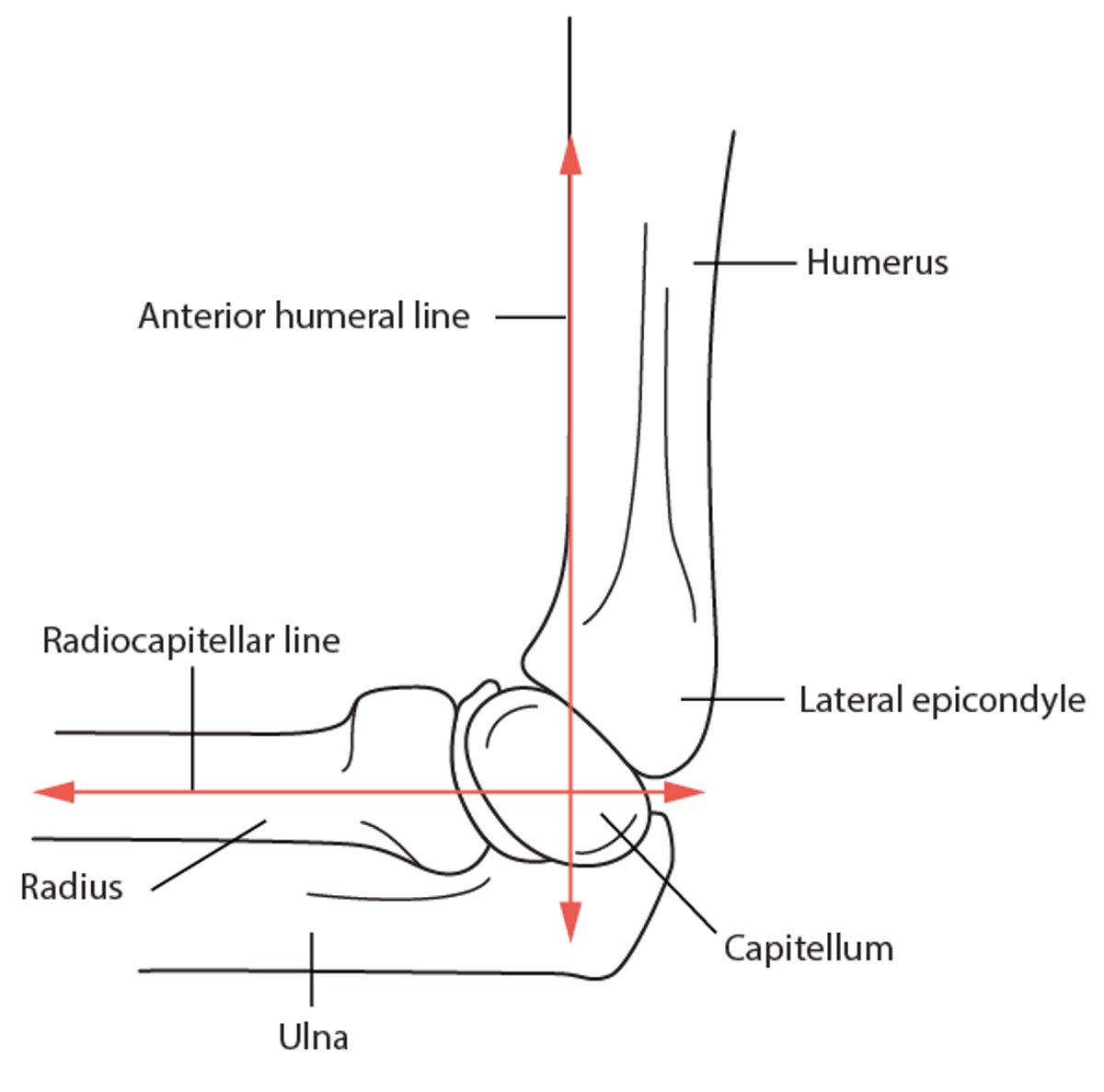
The anterior humeral line is a line drawn along the anterior border of the humerus on a true lateral radiograph. Normally, this line transects the middle of the capitellum. If the line transects none or only the anterior part of the capitellum, a posteriorly displaced distal humeral fracture is possible; then oblique views are taken, and other imaging may be done.
The radiocapitellar line is a line drawn through the midshaft of the radius on a true lateral radiograph of the elbow; normally, it bisects the capitellum. If it does not, an occult fracture should be suspected.
Pearls & Pitfalls
|
If findings in children are compatible with a distal humeral fracture, radiographs should be reviewed closely for evidence of occult fracture (eg, a posterior fat pad, abnormalities in the anterior humeral or radiocapitellar line).
A complete neurovascular examination is done if a fracture is suspected. Particular attention should be paid to the median, radial, and ulnar nerves. Distal pulses should be compared with those of the opposite limb, particularly if ecchymoses or enlarging swelling (which suggest brachial artery injury) are present on the anterior medial forearm.
Anterior Humeral Line and Radiocapitellar Line
Normally, the anterior humeral line, which is drawn along the anterior border of the humerus on a lateral radiograph, transects the middle of the capitellum. If the line transects none or only the anterior part of the capitellum, a distal humeral fracture with posterior displacement may be present. The radiocapitellar line, which is drawn through the midshaft of the radius, normally bisects the capitellum. If it does not, an occult fracture should be suspected. |


The anterior humeral line and radiocapitellar line are normal. However, an anterior fat pad is present, suggesting a joint effusion.
Image courtesy of Danielle Campagne, MD.

A posterior fat pad is always abnormal. Also on this radiograph, the anterior humeral line does not transect the middle of the capitellum.
Image courtesy of Danielle Campagne, MD.
The anterior humeral line and radiocapitellar line are normal. However, an anterior fat pad is present, suggesting a joint effusion.
Image courtesy of Danielle Campagne, MD.
A posterior fat pad is always abnormal. Also on this radiograph, the anterior humeral line does not transect the middle of the capitellum.
Image courtesy of Danielle Campagne, MD.
Treatment of Distal Humeral Fractures
Early orthopedic consultation
For nondisplaced fractures or occult fractures, splinting
For displaced fractures, often open reduction with internal fixation (ORIF)
For clinically suspected fractures, splinting and close follow-up
Displaced supracondylar fractures should be splinted in the position that they are in; they should not be reduced because of the risk of reduction-related median nerve and radial artery injury.
Most fractures are managed by an orthopedic surgeon because long-term complications are a risk. Most patients are admitted for neurovascular observation, although some clinicians splint and discharge patients who have nondisplaced fractures if patients can be trusted to return for follow-up the next day.
Posteriorly displaced or angulated distal humeral fractures, in particular, should be reduced by an orthopedic surgeon because nerves and/or the radial artery can be injured during reduction. Casting with closed reduction may be tried but is typically not recommended because ORIF is usually necessary.
If a fracture is suspected clinically (eg, children cannot move their elbow in a normal range of motion) and radiographs appear normal, the joint should be splinted and close follow-up should be arranged.
Pearls & Pitfalls
|
Key Points
Distal humeral fractures are more common among children.
These fractures can injure the radial artery or median nerve.
Check radiographs for posterior and anterior fat pads, and use the anterior humeral line and radiocapitellar line to determine whether an occult fracture is likely.
For treatment, consult an orthopedic surgeon.







