



- How To Cleanse, Irrigate, Debride, and Dress Wounds
- How To Repair a Laceration With Simple Interrupted Sutures
- How To Do Plastic Surgical Repair With Buried Deep Dermal Sutures
- How To Repair a Laceration With Glue
- How To Repair a Laceration With Horizontal Mattress Sutures
- How To Repair a Laceration With Stapling
- How To Repair a Laceration With a Subcuticular Running Suture
- How To Repair a Laceration With Vertical Mattress Sutures
Uncomplicated epidermal closure is most often done using simple interrupted sutures. Each suture consists of a single, roughly circular (ie, simple) loop of suture material, individually tied. This technique permits individual tensioning of each suture, and if one suture should later fail, the others remain unaffected.



The objective of all suture closures is to appose the wound edges (especially the dermis) without gaps or tension. (See figure Simple Cutaneous Suture.)
(See also Lacerations and How To Cleanse, Irrigate, Debride, and Dress Wounds).
Indications for Simple Interrupted Sutures
Wounds sufficiently deep that they would heal with excess scarring if not closed
Wounds having edges that can be satisfactorily approximated using these sutures
Wounds that are relatively recent and uncontaminated
Contraindications for Simple Interrupted Sutures
Absolute contraindications
None
Relative contraindications
Simple interrupted sutures should not be the sole method for closing wounds under high tension; for these wounds, other measures, such as buried deep dermal sutures or undermining, may be necessary prior to epidermal closure.
Sutures of any type may be contraindicated for wounds that are contaminated, relatively old, or that would be at higher risk of infection if closed by sutures, such as small bites to hands or feet, puncture wounds, or high-velocity missile wounds.
Wounds involving deep structures (eg, nerves, blood vessels, ducts, joints, tendons, bones) and those covering large areas or involving the face or hands may require specific repair techniques or referral to a surgical specialist.
Complications of Simple Interrupted Sutures
Infection
Cutting or scarring of skin due to pressure on the skin from the sutures
Ischemia and necrosis due to excessively tight sutures
Equipment for Simple Interrupted Sutures
Wound hygiene and closure techniques need not be sterile procedures. Although instruments that touch the wound (eg, forceps, needles, suture) must be sterile, clean nonsterile gloves as well as clean but not sterile water may be used in immunocompetent patients. Some operators prefer the better fit and better barrier protection of sterile gloves.
Clean procedure, barrier protection
Face mask and safety glasses (or a face shield), head caps, gowns, gloves
Sterile drapes, towels (for wound debridement and suturing)
Antiseptic solution (eg, chlorhexidine, povidone-iodine)Antiseptic solution (eg, chlorhexidine, povidone-iodine)
Sterile gauze squares (eg, 10 cm × 10 cm [4 inch × 4 inch])
Needle driver, toothed forceps or tissue hook, scissors, and suture material (typically, a nonabsorbable monofilament suture). For detailed discussion of the various types and sizes of suture material, refer to Lacerations.
Sometimes splints or other materials (for aftercare) to restrict motion or skin tension that may pull on the sutures
Materials used to dress the wound
Additional Considerations for Simple Interrupted Sutures
Wound tissue is vulnerable to further injury during any aspect of cleansing and closure. Never grasp the wound edges with a hemostat because doing so can crush the tissue; instead, use a tissue forceps or tissue hook when lifting and everting the wound edges.
Use only a needle driver (not a hemostat or forceps) for placing sutures because a driver holds a needle most securely without damaging it.
Excessive tension on the repaired laceration increases the degree of wound scarring.
Positioning for Simple Interrupted Sutures
Position the patient comfortably reclined or supine.
Adjust the stretcher height so that you will be comfortable sitting or standing at the bedside.
With lengthy lacerations, position yourself so that the laceration is roughly parallel to the front of your body.
The laceration should be well lit, preferably with an overhead procedure light.
Step-by-Step Description of Interrupted Sutures
(See How To Cleanse, Irrigate, Debride, and Dress Wounds for step-by-step descriptions of wound preparation, anesthesia, and dressing.)
Cleanse, anesthetize, irrigate, and debride the wound as necessary.
Place a sterile fenestrated drape over the wound. Place additional drapes nearby as needed to provide a large enough sterile work area.

Handling the instruments
Hold the needle driver in your dominant hand, with your index finger extended along the side. This grip gives the most control. Some experts recommend not putting your fingers in the finger holes of the needle driver while placing sutures; doing so can make it harder to insert the needle perpendicular to the skin. However, you may place your fingers in the holes when releasing the needle from the driver and also when you tie knots using the instrument (instrument tie).
Hold the tissue forceps in your nondominant hand, as you would a pencil. Do not close the tips of the forceps tightly on the skin, because this can damage tissues. Use only toothed forceps or a tissue hook when handling tissue to help prevent crushing the tissue.
Hold suture scissors with your index finger extended toward the tip for better control.
Inserting the sutures
In general, place the first suture in the middle of the wound.
Load the needle driver: Grasp the needle at a 90-degree angle with the very tip of the driver. Grasp the needle at the junction of the proximal and middle third of the needle.
Use the tip of the forceps as a hook (or use a tissue hook) to gently lift the tissue and evert the wound edges as needed while the sutures are being placed. Proper wound edge eversion during this step is essential to optimal approximation of the dermis, which ultimately helps maximize the strength and minimize scarring of the healed wound.
Place sutures by gently supinating your wrist so that the needle follows its curvature through the skin.
The needle should enter and exit the skin at a 90-degree angle (see figure Simple Cutaneous Suture). Match the bite depth and the bite width on both sides of the laceration. The bite depth should be greater than the bite width.
Push the needle through both wound edges if this can be done with little resistance. If resistance is significant—or if you are placing a suture across a relatively wide space (as may occur with the first few sutures of an interrupted suture closure)—pull out the needle through the center of the laceration after it passes through the first wound edge and then reattach it to the needle driver. Continue the suture with a second bite passing it into the opposite side of the wound.
Gently pull the suture through the path of the needle and leave some (eg, 2 to 3 cm) of the free end of the suture material exposed.
Release the needle from the driver, and allow the needle to rest on the sterile drape.
Tie the suture using an instrument tie as described below.
Repeating these steps, place all subsequent sutures in the middle of each open section, until there are no remaining gaps in the wound. Spacing between sutures is typically equal to the distance from needle entry to wound margin (see figure Suture Spacing).
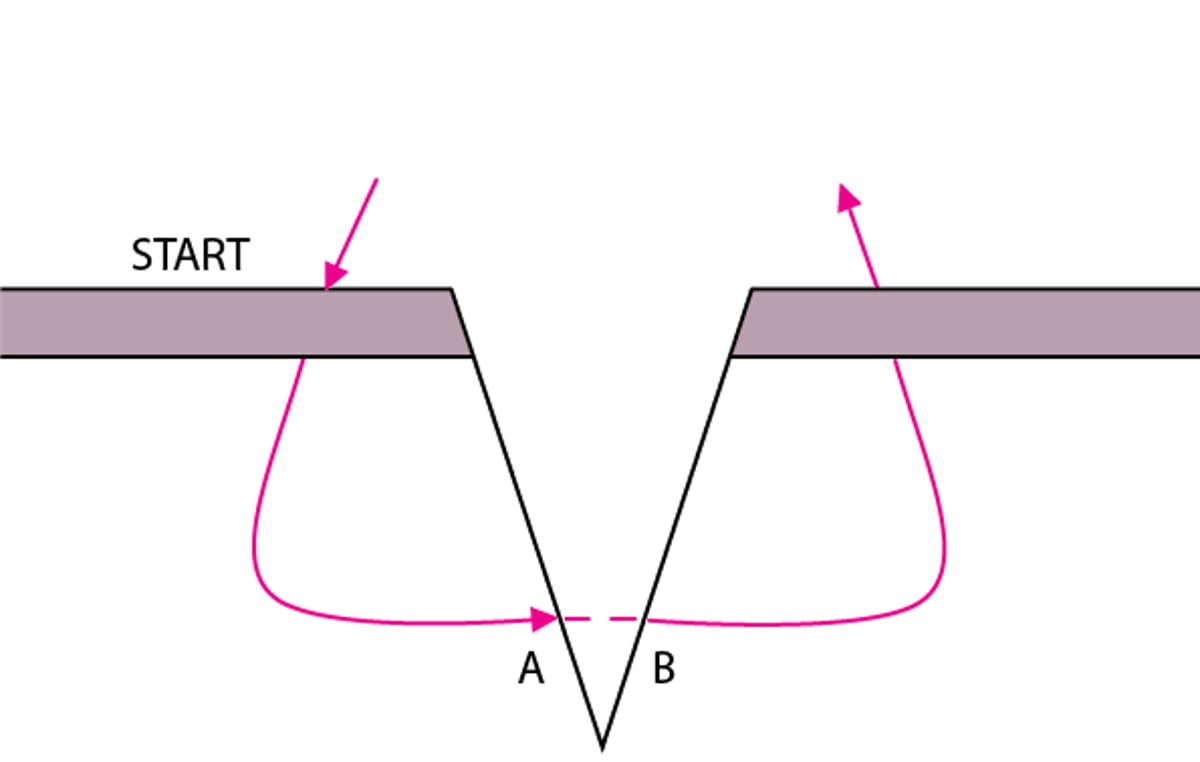
Simple Cutaneous Suture
The suture begins and ends equidistant from the wound margins. Points A and B are at the same depth. The suture is farther from the wound edge when the wound is deep. The skin edges should be everted by making the width of the bite greater at the deepest part of the wound than at the surface. |

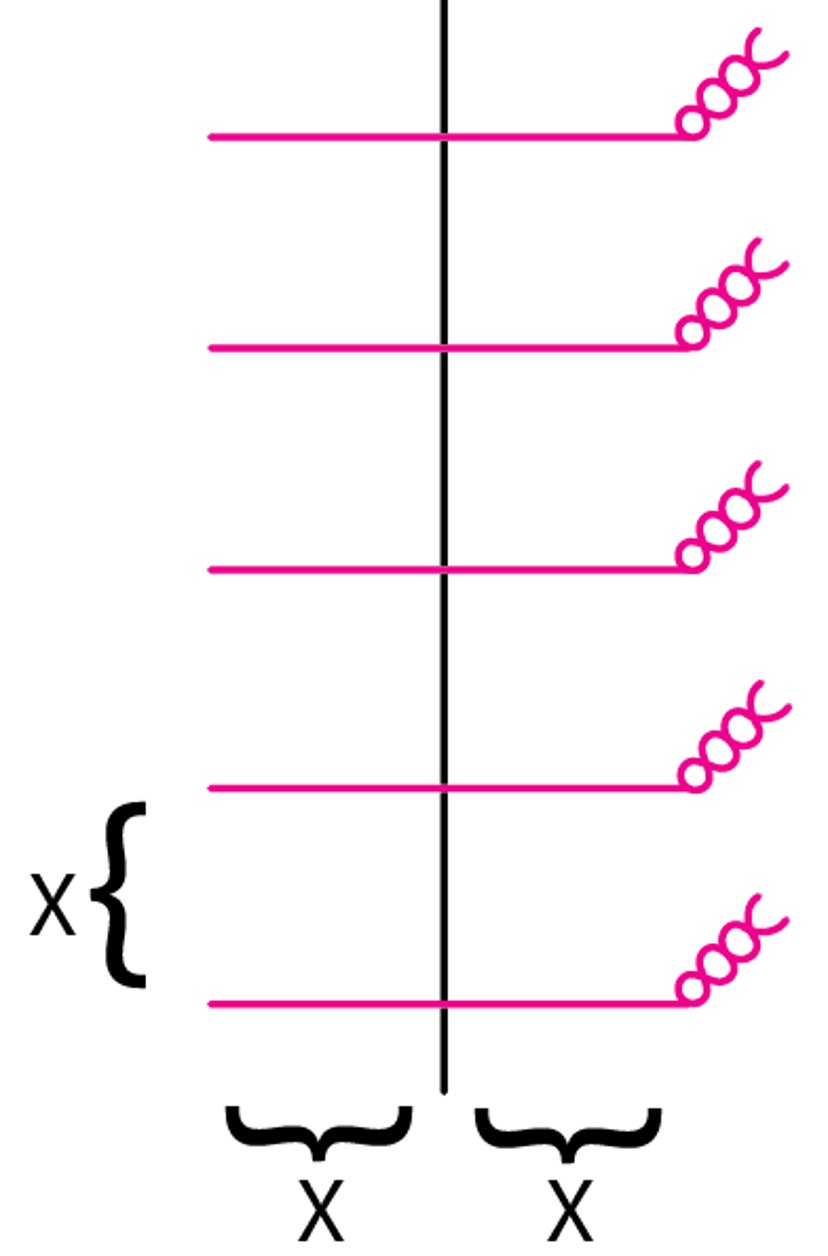
Suture Spacing
Spacing between sutures is typically equal to the distance from needle entry to wound margin. Sutures should enter and exit at an equal distance from the wound margin. |

The instrument tie
Hold the tip of the needle driver above and between the entry and exit sites of the suture. Use your nondominant hand to manually hold the long end of the suture (the needle-end). Be mindful of where the needle is lying and be careful to not allow the needle to stick your hand.
To lay down the first throw of the knot, wrap the needle-end (long end) of the suture OVER the end of the needle driver twice. Wrapping twice forms the base of the surgeon’s knot, which prevents the first throw from loosening. Next, rotate the driver 90 degrees and with it grasp the free (short) end of the suture. Pull your hands in opposite directions to lay down the first throw securely but not tightly; tight sutures risk cutting into the skin and causing ischemia as wound edema develops over the next several hours.
On the second and subsequent throws of the knot, wrap the needle-end of the suture OVER the needle driver only once. Grasp the free end of the suture with the driver and pull in opposite directions to tighten the knot. These subsequent throws may be pulled tightly.
Note that the suture is always drawn OVER the needle driver, and that your hands move in alternating directions across the laceration with each throw. Adhering to this method assures that all knots are square knots.
Place a total of about 4 throws. After the final throw, cut the suture with a scissors, leaving tails about 1 cm long.
Aftercare for Interrupted Sutures
Dress the wound (see Lacerations and How To Cleanse, Irrigate, Debride, and Dress Wounds).
Splint joints whose movement will cause wound tension (eg, an elbow splint for a dorsal elbow laceration).
Instruct the patient to keep the dressing dry and in place and to return in 2 days for a wound check.
Instruct the patient to return if signs of infection develop (eg, increased pain, swelling, redness, fever, proximally spreading red streaks [infectious lymphangiitis]).
Instruct the patient when to return for suture removal, which is generally based on the wound site: 3 to 5 days for the face, 6 to 10 days for the scalp and trunk, 10 to 14 days for the arms and legs, and 14 days for wounds overlying joints. Early suture removal risks wound dehiscence; however, to decrease scarring and cross-hatching of facial sutures, half of the suture line (ie, every other suture) may be removed on day 3 and the remainder are removed on day 5. An alternative is to remove all sutures on day 3 and support the closure by then applying wound tape.
Warnings and Common Errors for Interrupted Sutures
During pre-procedure preparation of the wound, diligently inspect the wound to avoid the frequent error of failing to note associated injuries of nearby tissues, foreign bodies, or body cavity penetrations.
Avoid overly tight sutures and use cautery sparingly because both can cause tissue ischemia.







