



Lacerations are tears in soft body tissue.
Topic Resources
















Care of lacerations
Enables prompt healing
Minimizes risk of infection
Optimizes cosmetic results
Physiology of Lacerations
Healing of lacerations begins immediately after injury with coagulation and introduction of white blood cells; neutrophils and macrophages remove debris (including devitalized tissue) and bacteria. Macrophages also encourage fibroblast replication and neovascularization. Fibroblasts deposit collagen, typically beginning within 48 hours and reaching a maximum in about 7 days. Collagen deposition is essentially complete in 1 month, but collagen fiber strength builds more slowly as fibers undergo crosslinking. Wound tensile strength is only about 20% of ultimate by 3 weeks, 60% by 4 months, and maximum at 1 year; strength never becomes equivalent to the undamaged state.
Epithelial cells from the wound edge migrate across the wound shortly after injury. In a surgically repaired wound (healing by primary intention), they form an effective protective barrier to water and bacteria in 12 to 24 hours and resemble normal epidermis within 5 days. In a wound that is not repaired (ie, heals by secondary intention), epithelialization is prolonged proportionally to the defect size.
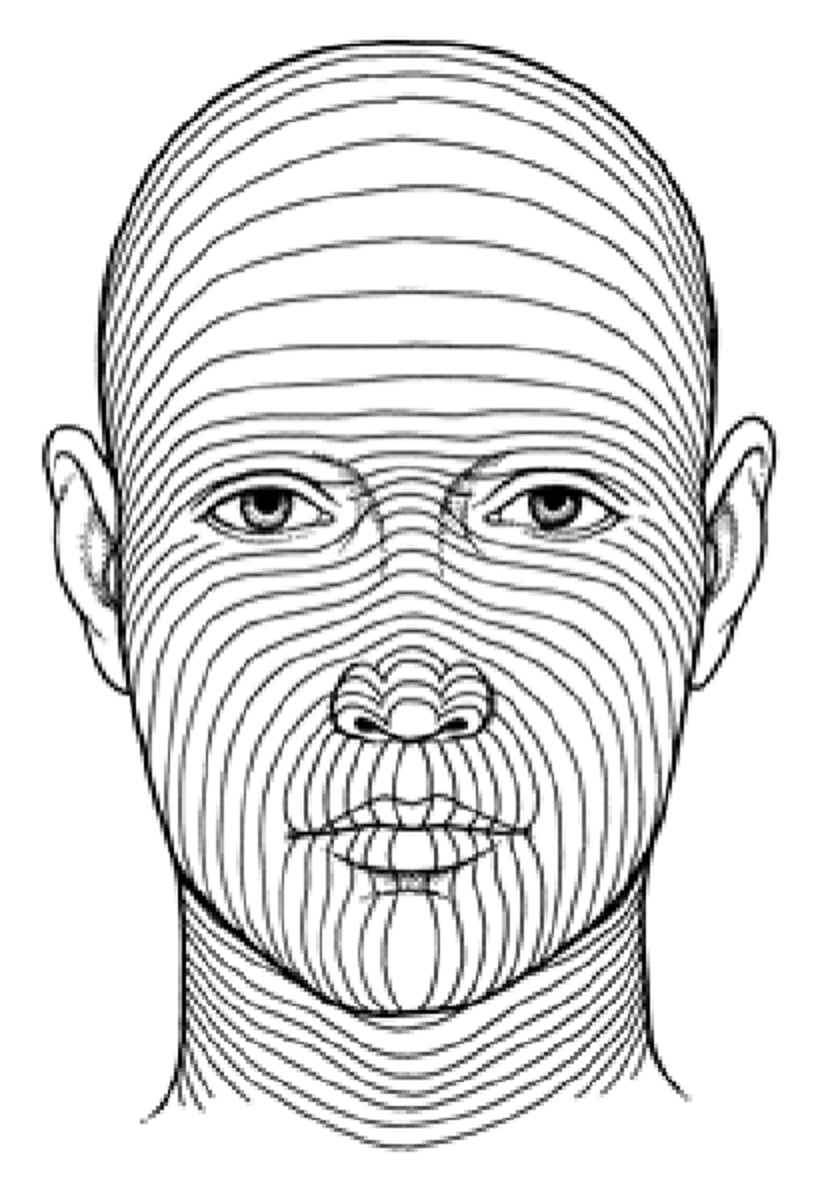
There are static forces on the skin because of its natural elasticity and the underlying muscles (see figure Representative minimal skin tension lines). Because scar tissue is not as strong as adjacent undamaged skin, these forces tend to widen scars, sometimes resulting in a cosmetically unacceptable appearance after apparently adequate wound closure. Scar widening is particularly likely when the forces are perpendicular to the wound edge. This tendency (and resultant wound stress) is readily observed in the fresh wound; gaping edges indicate perpendicular tension, and relatively well approximated edges indicate parallel forces.
Representative Minimal Skin Tension Lines
Direction of force is along each line. Cuts perpendicular to these lines are thus under greatest tension and most likely to widen. |

Scars tend to be red and prominent for about 8 weeks. As collagen remodeling occurs, the scar becomes thinner and loses its erythema. In some patients, however, the scar hypertrophies, becoming unsightly and raised. Keloids are exuberant scars that extend beyond the limits of the original wound and are more likely in patients with darker skin.
The most common factors that interfere with wound healing involve tissue ischemia, infection, or both (see table Factors That Interfere With Wound Healing); tissue ischemia predisposes to infection.
Lower extremities are usually at greatest risk of infection and poor healing due to impaired circulation. The scalp and face are at lowest risk. Certain drugs and disorders can also interfere with wound healing.
Bite wounds are usually heavily contaminated.
Factors That Interfere With Wound Healing
Factor | Examples |
|---|---|
Tissue ischemia (due to features of the wound or locally poor circulation) | Disorders affecting peripheral vasculature (eg, diabetes, arterial insufficiency) Type of injury (eg, a crush-type injury, which damages the microvasculature) Repair techniques (eg, overly tight sutures) Use of cautery |
Bacterial proliferation | Wound hematoma Foreign material (including deep dermal suture material) Delayed treatment (eg, > 6 hours for lower-extremity injuries; > 12 to 24 hours for face and scalp injuries) Significant wound contamination (as typically occurs in bite wounds) |
Drugs | Antiplatelet drugs and anticoagulants Drugs that suppress inflammation (eg, corticosteroids, immunosuppressants) |
Certain disorders | Disorders that suppress the immune system or impair healing (eg, chronic kidney disease) Undernutrition (eg, protein-calorie undernutrition, deficiencies of specific nutrients such as vitamin C) Disorders of collagen synthesis (eg, Marfan syndrome, Ehlers-Danlos syndrome) |
Evaluation of Lacerations
Sequential steps in evaluating lacerations include the following:
Finding and treating serious associated injuries
Obtaining hemostasis
Looking for damage to underlying structures
Clinicians must find and treat serious injuries before focusing on skin lacerations, however dramatic.
Actively bleeding wounds require hemostasis before evaluation. Hemostasis is best obtained by direct pressure and, when possible, elevation; clamping bleeding vessels with instruments is generally avoided because of the possibility of damaging adjacent nerves. Use of topical anesthetics containing epinephrine may also help reduce bleeding. Careful and temporary placement of a proximal tourniquet may enhance visualization of hand and finger wounds.require hemostasis before evaluation. Hemostasis is best obtained by direct pressure and, when possible, elevation; clamping bleeding vessels with instruments is generally avoided because of the possibility of damaging adjacent nerves. Use of topical anesthetics containing epinephrine may also help reduce bleeding. Careful and temporary placement of a proximal tourniquet may enhance visualization of hand and finger wounds.
Wound evaluation also requires good lighting. Magnification (eg, with magnifying glasses) can help, particularly for examiners with imperfect near-vision. Full wound evaluation may require probing or manipulation, and thus local anesthesia, but sensory examination should precede administration of a local anesthetic.
Associated injuries
The wound is evaluated for damage to underlying structures, including nerves, tendons, vessels, joints, and bones, as well as the presence of foreign bodies or body cavity penetration (eg, peritoneum, thorax). Failure to recognize these complications is one of the most significant errors in wound management.
Nerve injury is suggested by sensory or motor abnormality distal to the wound; suspicion is increased for lacerations near the course of significant nerves. Examination should test light touch and motor function. Two-point discrimination is useful for hand and finger injuries; the clinician touches the skin with 2 ends of a bent paper clip simultaneously to determine the minimum separation that allows perception of 2 points (usually 2 to 3 mm). Normal varies among patients and by location on the hand; the identical site on the uninjured side is the best control.
Tendon injury is suspected in any laceration over the course of a tendon. Complete tendon laceration usually causes a resting deformity (eg, foot drop due to Achilles tendon laceration, loss of normal resting finger flexion due to digital flexor laceration) because forces from antagonist muscles are unopposed. Resting deformity does not occur with partial tendon laceration, which may manifest with only pain or relative weakness on strength testing or be discovered only on exploration of the wound. The injured area should be examined through the full range of motion; the injured tendon may sometimes retract and not be visible on inspection or wound exploration when the injured area is in the resting position. Point-of-care ultrasound may also help identify tendon injuries.
Vascular injury is suggested by signs of ischemia, such as pallor, decreased pulses, or perhaps delayed capillary refill distal to the laceration (all compared with the uninjured side). Vascular injury is occasionally suspected in the absence of ischemia when a laceration traverses the territory of a major artery and is deep or complex or results from penetrating trauma. Other signs of vascular injury can include a rapidly expanding or pulsatile mass or a bruit.
Bone injury is possible, particularly after blunt trauma or when injury occurs over a bony prominence. If the mechanism or location of injury is concerning, plain x-rays are taken to rule out fracture.
Foreign bodies are sometimes present in wounds, depending on the mechanism. Wounds involving glass are likely to have foreign bodies, lacerations due to sharp metal rarely do, and wounds involving other substances are of intermediate risk. Although not very sensitive, a patient’s complaint of feeling a foreign body is fairly specific and should not be ignored. Localized pain or tenderness in a high-risk wound also is suggestive, particularly if pain worsens with active or passive motion. Wound examination and exploration are not sensitive for small foreign bodies unless the wound is superficial and its full depth is visible.
Pearls & Pitfalls
|
Joint penetration should be suspected when wounds near a joint are deep or involve penetrating trauma. A CT scan of the joint is highly sensitive for small volumes of intra-articular air, which indicate joint penetration (1). When in doubt, the joint may be injected with normal saline under sterile conditions. Visualization of injected fluid within an adjacent wound confirms joint penetration and such wounds should be irrigated expediently by a specialist in the operating room.
Penetration of the abdominal or thoracic cavity should be considered in any wound over those locations in which the bottom of the laceration is not clearly visible. Wounds should not be blindly probed; blind probing is unreliable and may cause further injury. Patients with suspected thoracic lacerations require a chest x-ray or other imaging study initially, with a repeat film after 4 to 6 hours of observation; any slowly developing pneumothorax should be visible by that time. In patients with abdominal lacerations, local anesthesia facilitates exploration (lacerations can be extended horizontally if necessary). Patients with wounds penetrating the fascia should be observed in the hospital; sometimes abdominal CT is used to identify hemoperitoneum. Bedside ultrasonography may also help identify injuries such as a pneumothorax, hemothorax, or hemoperitoneum, especially in unstable patients who cannot be transported to CT.
Imaging of lacerations
Imaging studies are recommended for all wounds involving glass and for other wounds if a foreign body is suspected because of the mechanism, the symptoms, or an inability to examine the wound’s full depth. If glass or inorganic material (eg, stones, metal fragments) is involved, plain x-rays are taken; glass bits as small as 1 mm are usually visible. Organic materials (eg, wood splinters, plastic) are rarely detected with plain x-rays (although the outline of larger objects may be visible because of their displacement of normal tissue); various other modalities have been used, including ultrasonography, CT, and MRI. None of these is 100% sensitive, but CT may offer the best balance between accuracy and practicality. A high index of suspicion and careful exploration of all wounds are always appropriate.
Evaluation reference
1. Konda SR, Davidovitch RI, Egol KA: Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J Orthop Trauma 27(9):498-504, 2013. doi: 10.1097/BOT.0b013e31828219bc
Treatment of Lacerations
Treating lacerations involves
Cleansing and local anesthesia (sequence can vary)
Exploration
Debridement
Closure
Tissue should be handled as gently as possible.
Cleansing lacerations
Both the wound and the surrounding skin are cleansed. Subepidermal tissue in the wound is relatively delicate and should not be exposed to harsh substances (eg, full-strength povidone iodine, chlorhexidine, hydrogen peroxide) and vigorous scrubbing.Both the wound and the surrounding skin are cleansed. Subepidermal tissue in the wound is relatively delicate and should not be exposed to harsh substances (eg, full-strength povidone iodine, chlorhexidine, hydrogen peroxide) and vigorous scrubbing.
Removing hair from laceration edges is not necessary for wound hygiene but can make markedly hairy areas (eg, scalp) easier to work on. If necessary, hair is removed with electric clippers or scissors, not shaving; razors create microtrauma, allowing skin pathogens to enter and increasing risk of infection. Hair is clipped before wound irrigation so that any clipped hair entering the wound is removed. Eyebrows are not trimmed because the hair-skin border is needed for proper alignment of wound edges. Traditional teaching is that the eyebrow may never grow back or grow back abnormally. However, evidence to support or refute this is lacking.
Although wound cleansing is not particularly painful, local anesthesia is usually administered first, except for heavily contaminated wounds; these wounds are best initially cleansed with running tap water and mild soap before a local anesthetic is administered. Tap water is clean and free of typical wound pathogens, and, used in this manner, does not seem to increase risk of infection. Wounds are then cleansed by a high-velocity stream of liquid and sometimes scrubbed with a fine-pore sponge; brushes and rough materials are avoided. An appropriate irrigation stream can be created using a 20-, 35-, or 50-mL syringe with a 20-gauge needle or IV catheter; commercially available devices incorporating a splash guard help limit splatter. Sterile 0.9% saline is an effective irrigant; specialized surfactant irrigants are costly and of doubtful additional benefit. If bacterial contamination is of particular concern (eg, bites, old wounds, organic debris), povidone iodine solution diluted 1:10 in 0.9% saline may be beneficial and is not harmful to tissues at this concentration. The volume necessary varies. Irrigation continues until visible contamination is removed and at least 100 to 300 mL has been applied (more for large wounds).
Painting the skin with a mixture of chlorhexidine and alcohol before suturing may reduce skin flora, but the substance should not be introduced into the wound.Painting the skin with a mixture of chlorhexidine and alcohol before suturing may reduce skin flora, but the substance should not be introduced into the wound.

Local anesthesia for laceration treatment
Generally, injectable local anesthetics are used. Topical anesthetics are beneficial in certain cases, especially for wounds of the face and scalp and when topical skin adhesives are used to close wounds.
Common injectable agents are lidocaine 0.5%, 1%, and 2%, and bupivacaine 0.25% and 0.5%, both from the amide group of local anesthetics; the ester group includes procaine, tetracaine, and benzocaine. Lidocaine is most commonly used. Bupivacaine has a slightly slower onset (several minutes vs almost immediate) and a significantly longer duration (2 to 4 hours vs 30 to 60 minutes). Duration of action of both can be prolonged by adding epinephrine 1:100,000, a vasoconstrictor. Because vasoconstriction may impair wound vascularity (and thus defenses), epinephrine is mostly used for wounds in highly vascular areas (eg, face, scalp). Although traditional teaching has been to avoid using epinephrine in distal parts (eg, nose, ears, fingers, penis) to prevent tissue ischemia, complications from use on distal parts are rare, and such use is now considered safe. Epinephrine can be particularly helpful in achieving hemostasis in wounds that are bleeding heavily.Common injectable agents are lidocaine 0.5%, 1%, and 2%, and bupivacaine 0.25% and 0.5%, both from the amide group of local anesthetics; the ester group includes procaine, tetracaine, and benzocaine. Lidocaine is most commonly used. Bupivacaine has a slightly slower onset (several minutes vs almost immediate) and a significantly longer duration (2 to 4 hours vs 30 to 60 minutes). Duration of action of both can be prolonged by adding epinephrine 1:100,000, a vasoconstrictor. Because vasoconstriction may impair wound vascularity (and thus defenses), epinephrine is mostly used for wounds in highly vascular areas (eg, face, scalp). Although traditional teaching has been to avoid using epinephrine in distal parts (eg, nose, ears, fingers, penis) to prevent tissue ischemia, complications from use on distal parts are rare, and such use is now considered safe. Epinephrine can be particularly helpful in achieving hemostasis in wounds that are bleeding heavily.
The maximum dose of lidocaine is 3 to 5 mg/kg (1% solution The maximum dose of lidocaine is 3 to 5 mg/kg (1% solution= 1 g/100 mL = 10 mg/mL), and that of bupivacaine is 2.5 mg/kg. Addition of epinephrine increases the allowable dose of lidocaine to 7 mg/kg, and of bupivacaine to 3.5 mg/kg.10 mg/mL), and that of bupivacaine is 2.5 mg/kg. Addition of epinephrine increases the allowable dose of lidocaine to 7 mg/kg, and of bupivacaine to 3.5 mg/kg.
Adverse reactions to local anesthetics include allergic reactions (urticaria and, occasionally, anaphylaxis) and sympathomimetic effects from epinephrine (eg, palpitations, tachycardia). True allergic reaction is rare, particularly to amide anesthetics; many patient-reported events represent anxiety or vagal reactions. Furthermore, allergic reactions are often due to methylparaben, the preservative used in multidose vials of anesthetic. If the offending agent can be identified, a drug from another class (eg, ester instead of amide) can be used. Otherwise, a test dose of 0.1 mL preservative-free (single-dose vial) lidocaine can be given intradermally; if there is no reaction within 30 minutes, that anesthetic can be used.) and sympathomimetic effects from epinephrine (eg, palpitations, tachycardia). True allergic reaction is rare, particularly to amide anesthetics; many patient-reported events represent anxiety or vagal reactions. Furthermore, allergic reactions are often due to methylparaben, the preservative used in multidose vials of anesthetic. If the offending agent can be identified, a drug from another class (eg, ester instead of amide) can be used. Otherwise, a test dose of 0.1 mL preservative-free (single-dose vial) lidocaine can be given intradermally; if there is no reaction within 30 minutes, that anesthetic can be used.
Techniques recommended to minimize the pain of injection include the following:
Using a small needle (a 27-gauge needle is best, and a 25-gauge is acceptable; a 30-gauge may be too flimsy)
Giving the injection slowly
Giving the injection into the subcutaneous plane instead of intradermally
Buffering lidocaine with 8.4% sodium bicarbonate, raising the pH from 4.2 to 7.4 (for example, at ratios of lidocaine to sodium bicarbonate that can range from 3:1 to 9:1) (NOTE: Buffering decreases the shelf life of multidose lidocaine vials, and buffering is less effective for bupivacaine.)Buffering lidocaine with 8.4% sodium bicarbonate, raising the pH from 4.2 to 7.4 (for example, at ratios of lidocaine to sodium bicarbonate that can range from 3:1 to 9:1) (NOTE: Buffering decreases the shelf life of multidose lidocaine vials, and buffering is less effective for bupivacaine.)
Warming the anesthetic solution to body temperature
Pretreating the wound with topical anesthetic
Brief cooling of wound edges with ice
Regional nerve blocks are sometimes preferred to wound injection. Nerve blocks cause less distortion of wound edges by injected anesthetic; this decreased distortion is important when alignment of wound edges must be particularly precise (eg, infraorbital nerve block for lacerations through the vermilion border of the lip) or when wound injection would be difficult because the space for injection is small (eg, digital nerve block for finger lacerations). Also, large areas can be anesthetized without using toxic doses of anesthetic. Slight disadvantages of nerve blocks are slower onset of anesthesia and sometimes < 100% effectiveness with the first injection.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.


© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

Procedure demonstrated by Scott Solow, DDS, Pediatric Dentistry and Orthodontics. Filmed on location at Pediatric Dentistry and Orthodontics Medical Arts Building, Philadelphia, PA.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.

© Elsevier Inc. All Rights Reserved. This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
Use of topical anesthesia makes injection unnecessary and is completely painless—factors particularly desirable in children and fearful adults. The most common solution is LET, which consists of lidocaine 2 to 4%, epinephrine 1:1000 or 1:2000, and tetracaine 0.5 to 2%. A cotton dental pledget (or cotton ball) the length of the wound soaked in several milliliters of the solution and placed within the wound for 30 minutes usually provides adequate anesthesia. If anesthesia is incomplete after application of a topical anesthetic, supplementary local anesthetic can be injected through the partially anesthetized wound edges, usually with minimal pain.makes injection unnecessary and is completely painless—factors particularly desirable in children and fearful adults. The most common solution is LET, which consists of lidocaine 2 to 4%, epinephrine 1:1000 or 1:2000, and tetracaine 0.5 to 2%. A cotton dental pledget (or cotton ball) the length of the wound soaked in several milliliters of the solution and placed within the wound for 30 minutes usually provides adequate anesthesia. If anesthesia is incomplete after application of a topical anesthetic, supplementary local anesthetic can be injected through the partially anesthetized wound edges, usually with minimal pain.
Exploration of lacerations
The full extent of the wound is explored to look for foreign material and possible tendon injury. Foreign material may also often be discerned by palpating gently with the tip of a blunt forceps, feeling for a discrete object and listening for a click characteristic of glass or metal foreign bodies. Occasionally, contaminated puncture wounds (eg, human bite wounds near the metacarpophalangeal joint) must be extended so that they can be adequately explored and cleansed. Deep wounds near a major artery should be explored in the operating room by a surgeon.
Debridement of lacerations
Laceration debridement uses a scalpel, scissors, or both to remove dead tissue, devitalized tissue (eg, tissue with a narrow base and no viable blood supply), and sometimes firmly adherent wound contaminants (eg, grease, paint). Macerated or ragged wound edges are excised; usually 1 to 2 mm is sufficient. Otherwise, debridement is not used to convert irregular wounds into straight lines. Sharply beveled wound edges are sometimes trimmed so that they are perpendicular.
Closure of lacerations
Decision to close a wound depends on the wound’s location, age, cause, and degree of contamination and on patient risk factors.
Most wounds can be closed immediately (primary closure). Primary closure is usually appropriate for uninfected and relatively uncontaminated wounds < 6 to 8 hours old (< 12 to 24 hours for face and scalp wounds).
Many other wounds can be closed after several days (delayed primary closure). Delayed primary closure is appropriate for wounds too old for primary closure, particularly if signs of infection have begun to appear, and for wounds of any age with significant contamination, particularly if organic debris is involved. The threshold for using delayed primary closure is lowered for patients with risk factors for poor healing.
At initial presentation, anesthesia, exploration, and debridement are done at least as thoroughly as for other wounds, but the wound is loosely packed with moist saline-soaked gauze. The dressing is changed at least daily and evaluated for closure after 3 to 5 days. If there are no signs of infection, the laceration is closed by standard techniques. Loosely closing such wounds initially may be ineffective and inappropriate because the wound edges nonetheless typically seal shut within 12 to 24 hours.
Some wounds should not be closed. These wounds include the following:
Small bites to hands or feet
Puncture wounds
High-velocity missile wounds
Materials and methods for laceration repair
Traditionally, sutures have been used for laceration repair, but metal staples, adhesive strips, and liquid topical skin adhesives are now used for certain wounds, mainly linear lacerations subject to only small amounts of tension. Whatever the material used, preliminary wound care is the same; a common error is to do cursory exploration and no debridement because a noninvasive closure not requiring local anesthesia is planned.
Staples are quick and easy to apply and, because there is minimal foreign material in the skin, are less likely to cause infection than sutures. However, they are suited mainly for straight, smooth cuts with perpendicular edges in areas of low skin tension. Improper wound edge apposition (sometimes causing wound edges to overlap) is the most common error.
Topical skin adhesives usually contain octyl cyanoacrylate, butyl cyanoacrylate, or both. They harden within a minute; are strong, nontoxic, and waterproof; form a microbial barrier; and have some antibacterial properties. However, adhesive should not be allowed into the wound. Infections are very unlikely, and cosmetic results are generally good.
Adhesive is best for simple, regular lacerations; it should not be used for wounds under tension unless tension is relieved with deep dermal sutures, immobilization, or both. In wounds requiring debridement, deep dermal suturing, or exploration under local anesthesia, the advantages of decreased pain and time are minimized. However, patients do not require follow-up for suture or staple removal. With long lacerations, skin edges can be held together by a 2nd person or with skin tapes while the adhesive is applied. Generally, only one layer is applied as recommended by the manufacturer. The adhesive sloughs spontaneously in about a week. Excess or inadvertently applied adhesive can be removed with any petrolatum-based ointment or, in areas away from the eyes or open wounds, acetone.
Adhesive strips are probably the quickest repair method and have a very low infection rate. They are useful for wounds not subject to tension. Use on lax tissue (eg, dorsum of hand) is difficult because wound edges tend to invert. Adhesive strips cannot be used on hairy areas. Adhesive strips are particularly advantageous for lacerations in an extremity that is to be casted (thus blocking appropriate suture removal). Adhesive strips can also be used to reinforce wounds after suture or staple removal. Skin must be dry before application. Many clinicians apply tincture of benzoin to boost adhesion. Improper application may result in blister formation. Adhesive strips may be removed by the patient or eventually will fall off on their own.
Sutures are the best choice for
Irregular, heavily bleeding, or complex lacerations
Areas of loose skin
Areas under tension
Wounds requiring deep dermal closure
Because sutures can serve as an entry site for bacteria and there is a significant amount of foreign material under the skin, they have the highest rate of infection among materials used to close lacerations. Suture materials can be monofilament or braided and absorbable or nonabsorbable. Characteristics and uses vary (see table Suture Materials); generally, absorbable material is used for deep dermal sutures, and nonabsorbable material is used for percutaneous ones. Outcomes using rapidly absorbing absorbable sutures are comparable to those using nonabsorbable sutures. Rapidly absorbing absorbable sutures should be considered when suture removal is undesirable, such as in children and nonadherent patients. Braided material generally has higher tissue reactivity and thus poses a slightly higher risk of infection than does monofilament but is soft and easy to handle and has good knot security. Absorbable sutures containing antiseptic agents such as triclosan are available and may help reduce infection.
Suture Materials
Category | Material | Comments |
|---|---|---|
Nonabsorbable (preferred for cutaneous repair) | ||
Monofilament | Nylon | Strong Stiff Moderately hard to work with |
Polypropylene | Poorest knot security Soft, more pliable Most difficult to work with | |
Polybutester | Somewhat elastic, so lengthens with wound edema and contracts as edema resolves | |
Braided | Polyester | Low reactivity Not preferred to monofilament for cutaneous use |
Silk | Soft, easy to work with Good knot security High tissue reactivity Typically limited to use on the mouth, lips, eyelids, and intraorally, where patient comfort is significantly better (because removal of intraoral sutures can be difficult, most clinicians use absorbable sutures in that area) | |
Absorbable (preferred for deep dermal sutures) | ||
Monofilament | Poliglecaprone 25 | Handles like nonabsorbable sutures Easily passes through tissues Low tissue reactivity Rapid absorption (1–2 weeks) |
Polydioxanone | Very strong and long lasting (absorption, 180 days) Stiffer, more difficult to handle than other absorbable sutures Lowest tissue reactivity among absorbable sutures May extrude over time | |
Natural | Gut, chromic gut | From sheep intima Weak, rapidly absorbed (1 week) Poor knot security High tissue reactivity Not preferred |
Braided | Polyglycolic acid | Easy handling Good knot security Mild reactivity Most strength gone in 1 week First absorbable suture |
Polyglactic acid | Easy handling Good knot security Mild reactivity Most strength gone in 3 weeks | |
Suture technique for laceration repair
General goals include the following:
Closely approximating skin margins
Everting wound edges
Eliminating dead space
Minimizing tension on the wound and of individual sutures
Minimizing the amount of foreign material
The relative importance of minimizing wound tension and minimizing the amount of material buried under the skin (eg, deep dermal sutures) vary by wound location. For example, in facial wounds, cosmetic result is very important and, because of the excellent vascular supply, infection risk is low. Thus, for gaping wounds, deep dermal sutures, which decrease wound tension and improve cosmetic result, are desired; infection risk is low even if they are used. In areas where vascular supply is poor or cosmetic result is less important, deep dermal sutures are less desirable.
Sutures may be placed and tied individually (interrupted sutures) or be continuous (running suture). They may be completely buried under the skin (subcuticular or deep dermal sutures) or enter and exit the skin to be tied externally (percutaneous sutures).
Simple deep dermal suture
The suture begins and ends at the bottom of the wound so that the knot is deeply buried. |

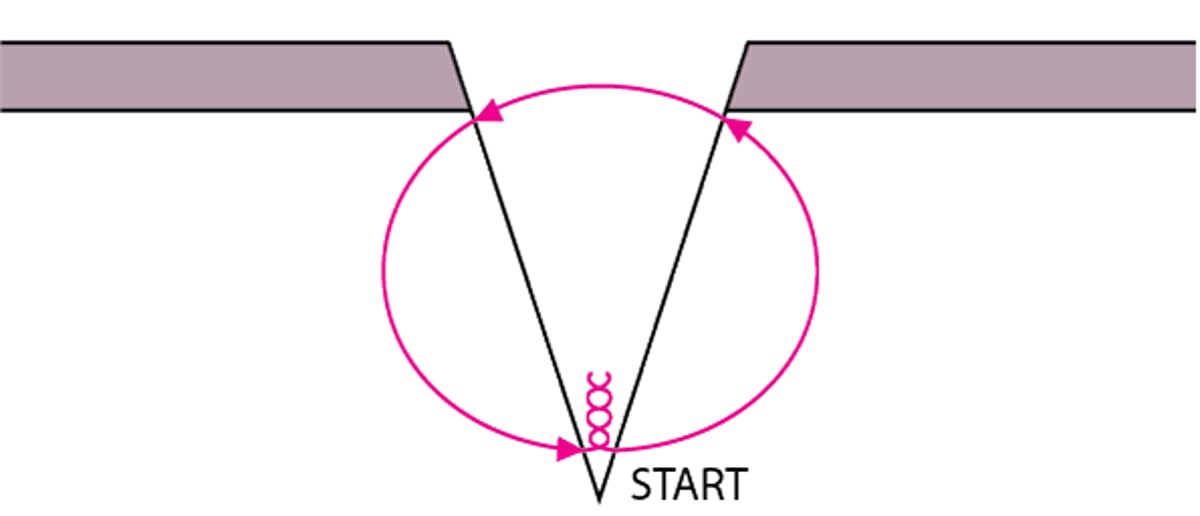
If the wound is gaping, deep dermal suturing tends to be used initially (see figure Simple deep dermal suture); the resultant narrow epidermal gap is then closed by percutaneous sutures. For wounds on the face, any gaping > 5 to 10 mm may benefit from deep dermal suturing (not used on nose and eyelids); in other body areas, a wider gap is acceptable. Interrupted sutures using size 4-0 or 5-0 (smaller numbers indicate thicker material with greater tensile strength) absorbable material (eg, polyglactic acid, poliglecaprone 25) are most common. They are placed with the knot at the bottom of the wound to avoid a palpable lump and must not be too tight. A running subcuticular suture is sometimes used, especially for cosmetic repairs.
Simple Cutaneous Suture
The suture begins and ends equidistant from the wound margins. Points A and B are at the same depth. The suture is farther from the wound edge when the wound is deep. The skin edges should be everted by making the width of the bite greater at the deepest part of the wound than at the surface. |

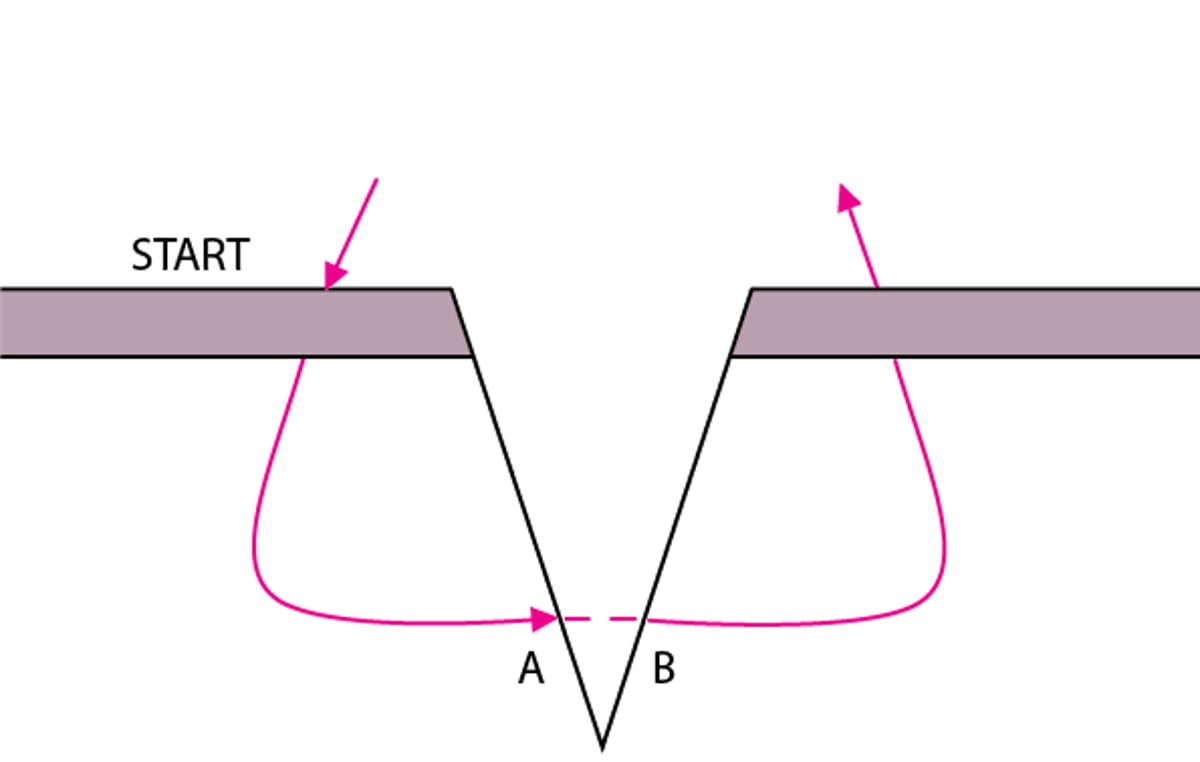
Epidermal closure is typically with simple, interrupted sutures (see figure Simple cutaneous suture) of nonabsorbable monofilament (eg, nylon, polypropylene). Suture size depends on where the wound is located.
In areas over large joints and the scalp, size 3-0 or 4-0 sutures are used.
For facial wounds, size 5-0 or 6-0 sutures are used.
For wounds in the hand, size 5-0 sutures are used.
In most other areas, size 4-0 or 5-0 sutures are used.
Suture size can vary slightly depending on how much static and dynamic tension is predicted (eg, for facial lacerations subject to frequent movement or high tension, size 5-0 sutures may be used).
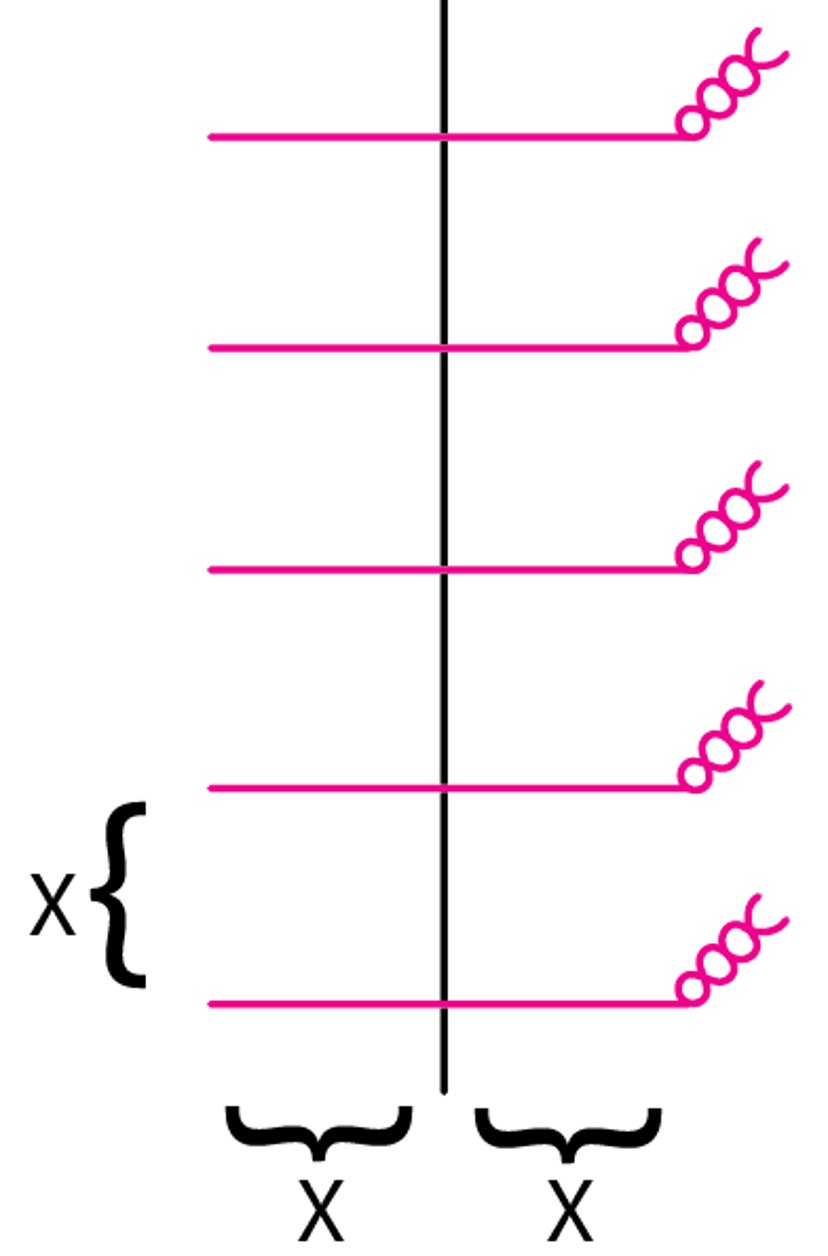
Sutures are placed about as deep as they are wide and are spaced as far apart as the distance from the needle entry point to wound edge (see figure Suture spacing). Small bites (suture typically inserted 1 to 3 mm from the wound edge) are used for repairs in areas where cosmetic results are of particular concern and when tissues are thin. For other repairs, wider bites are used, varying with the tissue thickness. Wound edges can be everted by making the width of the bite greater at the deepest part of the wound than at the surface. Eversion is more easily obtained when the hand is fully pronated and the skin is entered with the needle at a 90° angle and angled slightly away from the skin edge.
Suture Spacing
Spacing between sutures is typically equal to the distance from needle entry to wound margin. Sutures should enter and exit at an equal distance from the wound margin. |

A vertical mattress suture (see figure Vertical mattress suture) is sometimes used instead of a layered closure, provided skin tension is not marked; it also helps ensure proper edge eversion in loose tissue. A running suture (see figure Running suture) is quicker to place than interrupted sutures and can be used when wound edges are well aligned.
Vertical Mattress Suture
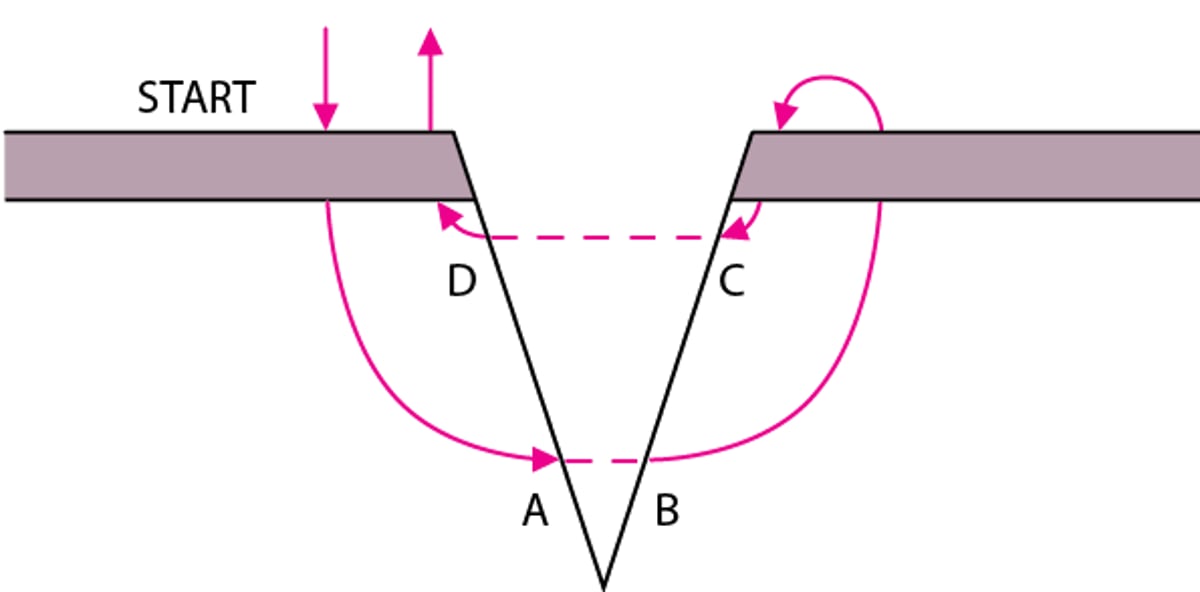
The first pass of the needle is the same as a large simple suture, but instead of tying off, another smaller bite is taken back across the wound to end on the starting side. Both ends are pulled up to closely align (approximate) the wound edges. Points A and B must be at the same depth, as must points C and D; this placement results in correct vertical alignment. |

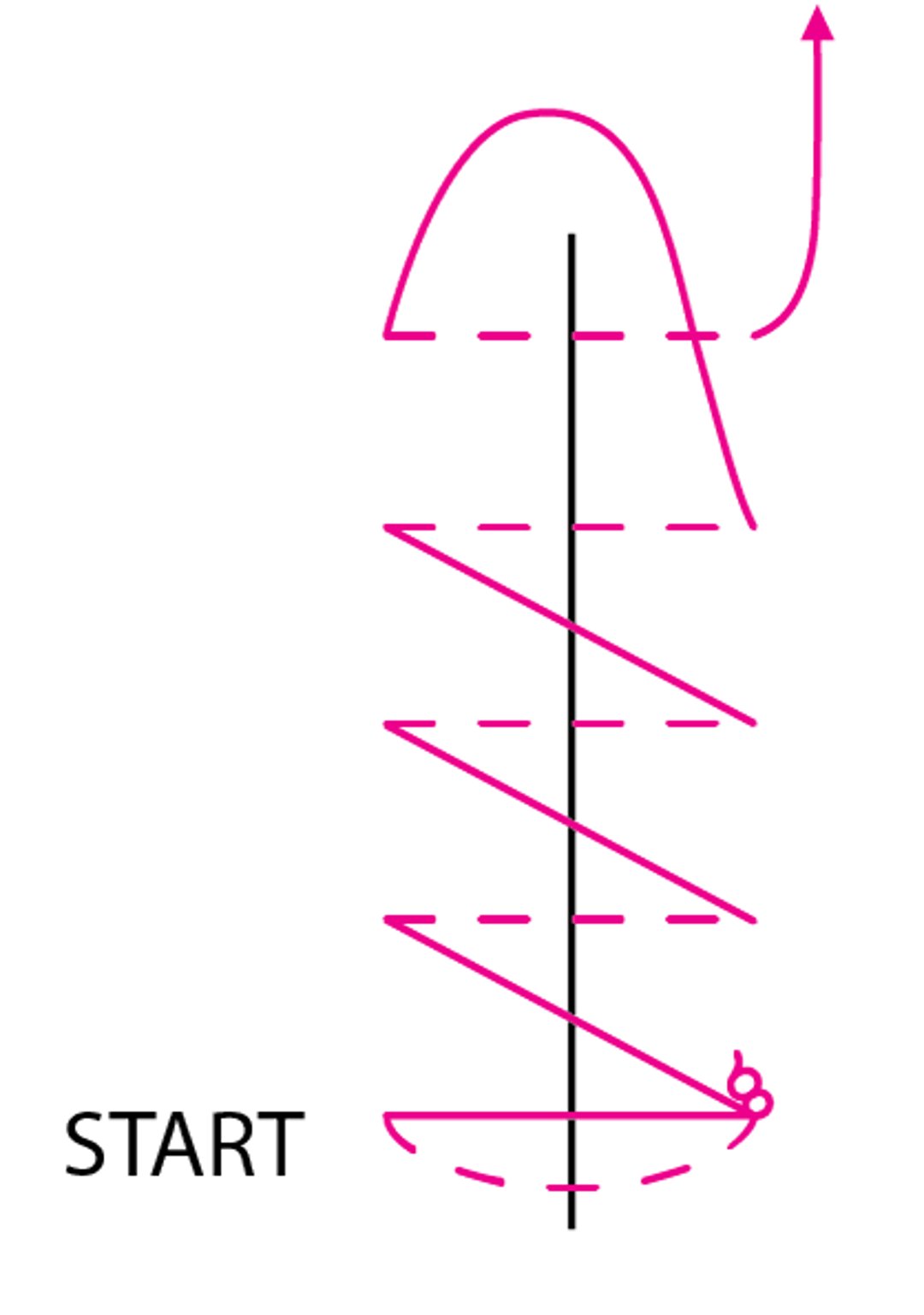
Running suture
This suture begins with a simple suture at one end of the wound. The non-needle end is cut, and then suturing continues; the bite under the skin is perpendicular to the wound, and the crossover is at about a 65° angle. Sutures should be evenly spaced and are snugged up as they are done, except for the last one, which is left as a loop; this loop is tied to the needle end. |

In all cases, epidermal closure must precisely realign edges horizontally using natural skin landmarks (eg, folds, creases, lip margins) when available. Vertical alignment is equally important to avoid a step-off deformity. Excess tension after closure is evidenced by indenting of the skin or a sausage link appearance. Such a repair should be redone, adding deep dermal sutures, additional percutaneous sutures, or both as needed. Adjustments to suture technique are needed to achieve optimal alignment when wound edges are beveled. For example, edges may be debrided or suture bite size may differ from one side of the wound to the other.
Aftercare
Tetanus immunization is given if necessary (see table Tetanus Prophylaxis in Routine Wound Management).
Topical antibiotic ointment (eg, bacitracin, bacitracin/neomycin/polymyxin) is applied daily; it can reduce risk of infection and help maintain a moist wound environment that optimizes healing. However, ointment is not used over tissue adhesives or adhesive strips.(eg, bacitracin, bacitracin/neomycin/polymyxin) is applied daily; it can reduce risk of infection and help maintain a moist wound environment that optimizes healing. However, ointment is not used over tissue adhesives or adhesive strips.
Prophylactic systemic antibiotics are not indicated except for the following cases:
Bite wounds on the extremities
Wounds involving tendons, bones, or joints
Possibly intraoral lacerations
Some heavily contaminated wounds
If deemed necessary, antibiotics are given as early as possible; the first dose may be given parenterally.
Wounds are immobilized because excess movement of the affected area may interfere with healing. Wounds near joints should be immobilized with splints. Bulky dressings are used to immobilize fingers and hands. Wounds should be elevated, above heart level when feasible, for the first 48 hours after suturing. A sling may help maintain some degree of elevation of an upper extremity wound. Patients with distal lower extremity lacerations (other than minor) should probably stay off their feet for several days (eg, by using crutches); elevation of the foot and restrictions on walking probably result in better healing.
Wound care is meticulous. The wound is kept clean and dry; dressings that are nonadherent and impermeable to bacteria are usually applied. Antibiotic ointment is applied daily until the wound closure device is removed. A reliable patient may inspect minor, clean lacerations, but early physician examination is preferable for higher risk wounds and wounds in unreliable patients. After 12 hours, well-healing wounds can be cleansed gently of residual secretions with water, half-strength hydrogen peroxide, or soap and water. Brief wetting in the shower is safe, but prolonged soaking should be avoided.is meticulous. The wound is kept clean and dry; dressings that are nonadherent and impermeable to bacteria are usually applied. Antibiotic ointment is applied daily until the wound closure device is removed. A reliable patient may inspect minor, clean lacerations, but early physician examination is preferable for higher risk wounds and wounds in unreliable patients. After 12 hours, well-healing wounds can be cleansed gently of residual secretions with water, half-strength hydrogen peroxide, or soap and water. Brief wetting in the shower is safe, but prolonged soaking should be avoided.
Wound infection occurs in 2 to 5% of lacerations; steadily increasing pain ≥ 12 hours after closure is often the earliest manifestation, and initial signs are redness more than about 0.5 cm from the wound edge, swelling, tenderness, and warmth. Later signs may include fever, purulent drainage, and ascending lymphangitis. Systemic antibiotics effective against skin flora are begun; a 1st-generation cephalosporin (eg, cephalexin 500 mg orally 4 times a day) or, for intraoral infection, penicillin 500 mg po qid, is typically used. Infection beginning . Systemic antibiotics effective against skin flora are begun; a 1st-generation cephalosporin (eg, cephalexin 500 mg orally 4 times a day) or, for intraoral infection, penicillin 500 mg po qid, is typically used. Infection beginning> 5 to 7 days after injury suggests a retained foreign body.
Closure material (except for tissue adhesive) is removed after various intervals depending on location. For facial lacerations, sutures are removed in 3 to 5 days to prevent cross-hatching and visible needle entrance marks; some clinicians apply adhesive strips to bolster the wound for a few more days. Sutures and staples on the torso and upper extremities are removed in 7 to 10 days. Sutures and staples on hands and fingers, the extensor surface of the elbow, knee, and anywhere below the knee should remain for 10 to 12 days.







