


Any cancer has the potential to metastasize to bone, but metastases from carcinomas are the most common, particularly those arising in the following solid organs:
Prostate cancer in men and breast cancer in women are the most common types of cancers. Lung cancer is the most common cause of cancer death in both sexes. Breast cancer is the most common cancer to metastasize to bone. Any bone may be involved with metastases. Metastatic disease does not commonly spread to bone below the mid forearm or mid calf, but when it occurs in those sites (acral metastasis), it results most often from lung or renal cancer.
The American Cancer Society projects that the incidence of breast cancer in females (316,950) will be higher than the incidence of lung cancer in males and females combined (124,730) (1). However, the incidence of lung cancer deaths, whether in males (64,190) or females (60,540), will be higher than the incidence of breast cancer deaths in females (42,170) or prostate cancer in males (35,770). Published case series of orthopedic surgical management of metastatic lesions in cancer centers show that breast cancer remains the most common cancer requiring orthopedic intervention (2). Usually medically treated metastatic breast cancer patients survive longer before they succumb to lung, liver, and brain metastasis compared to other solid organ metastatic lesions.
References
1. American Cancer Society. Cancer Facts & Figures 2025. Accessed February 11, 2025.
2. Toma CD, Dominkus M, Nedelcu T, et al. Metastatic bone disease: a 36-year single centre trend-analysis of patients admitted to a tertiary orthopaedic surgical department. J Surg Oncol. 2007;96(5):404-410. doi:10.1002/jso.20787
Symptoms and Signs of Metastatic Bone Tumors
Metastases manifest as bone pain, although they may remain asymptomatic for some time. Bone metastases may cause symptoms before the primary tumor is suspected or may appear in patients with a known diagnosis of cancer.
Diagnosis of Metastatic Bone Tumors of Unknown Origin
History, physical examination, and laboratory testing (complete blood count, metabolic panel, serum/urine protein electrophoresis, prostate-specific antigen in men)
Radiograph of the entire bone
Advanced imaging (CT scan of the chest/abdomen/pelvis)
Whole-body radionuclide technecium-99m bone scanning to identify other sites of metastases
Biopsy to confirm origin of the primary tumor
Metastatic bone tumors are considered in all patients over 40 years old with unexplained bone pain, but particularly in patients who have
A known cancer history
Pain or radiographic abnormalities at more than one site
Findings on imaging studies that suggest metastases to other locations
Prostate cancer is most often blastic, lung cancer is most often lytic, and breast cancer may be blastic or lytic.

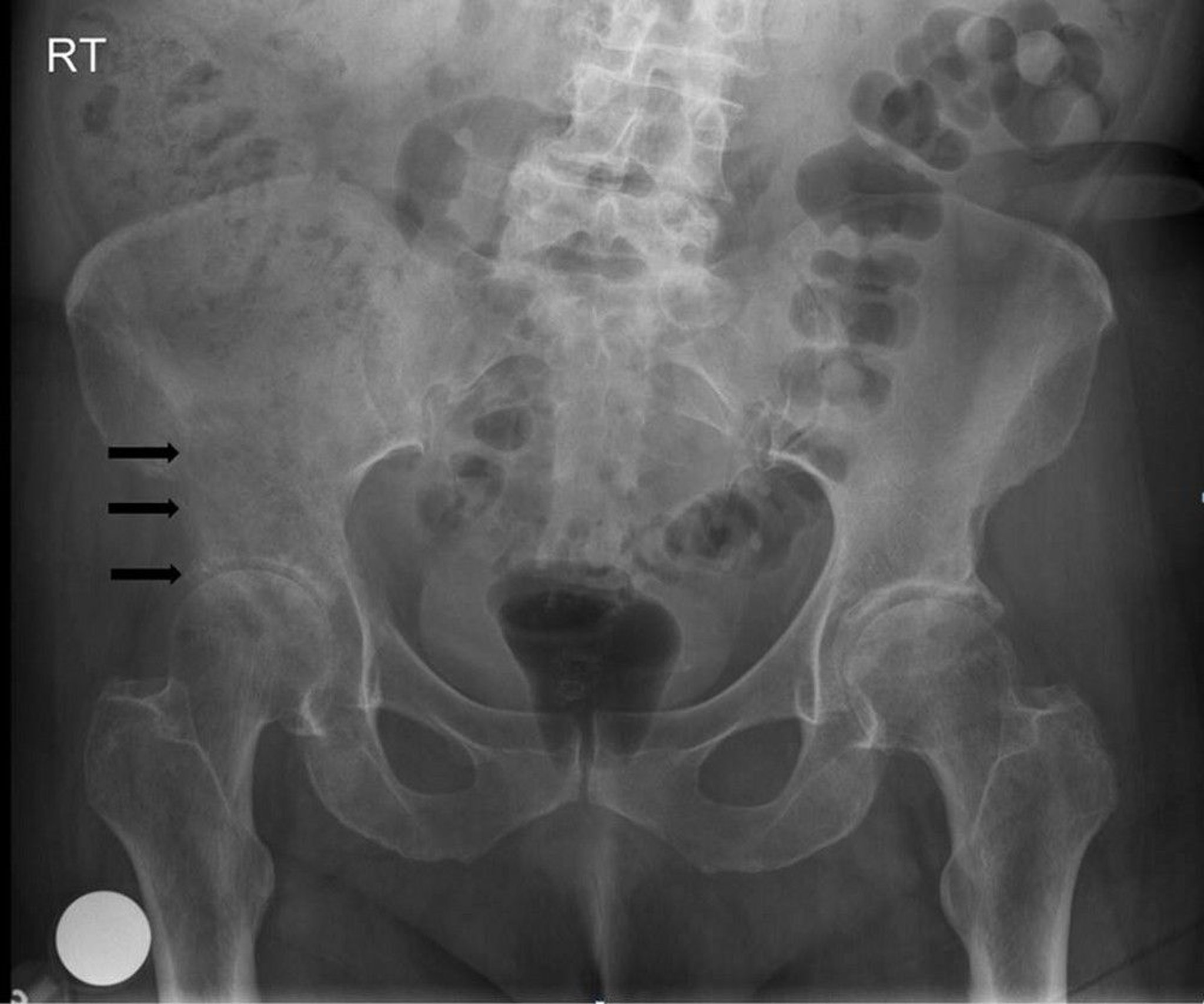
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
If metastases are suspected, a radionuclide whole-body scan or PET/CT is usually done. Bone scan or PET/CT is more sensitive for early and asymptomatic bone metastases than radiographs and can be used to scan the entire body. Lesions on the scan are usually presumed to be metastases if the patient has a known primary cancer.
Metastases should be suspected in patients who have multiple lesions on bone scan or PET scan. Although metastases are suspected in patients with known cancer and a single bone lesion, the lesion may not be a metastasis, particularly if the patient's cancer history was low-grade and/or if there has been a long disease-free interval. Thus, a biopsy of the lesion is recommended in those instances to confirm the diagnosis of a metastasis.
An evaluation to identify an initially unknown primary cancer in a patient with a single or multiple bony lesions includes a comprehensive history and physical examination, CT of the chest/abdomen/pelvis, and laboratory evaluation. Such an approach will identify the primary cancer over 85% of the time (1). The diagnosis suspected on this staging evaluation is confirmed by bone biopsy, typically image-guided core biopsy. Biopsy with use of immunohistologic stains may give clues to the primary tumor type. Sometimes the primary tumor cannot be identified after these tests, in which case additional evaluation, including PET/CT and any indicated endoscopy, is performed.

CAVALLINI JAMES/BSIP/SCIENCE PHOTO LIBRARY
Diagnosis reference
1. Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg Am. 1993;75(9):1276-1281. doi:10.2106/00004623-199309000-00003
Treatment of Metastatic Bone Tumors
Usually radiation therapy for symptomatic or large or progressively enlarging lesions
Surgery to stabilize bone at risk of pathologic fracture or resect highly diseased bone (with joint reconstruction if needed)
Kyphoplasty or vertebraplasty for certain painful vertebral fractures
Treatment of metastatic bone tumors depends on the type of tissue involved (which organ tissue type). Radiation therapy, combined with selected chemotherapeutic or hormonal drugs, is the most common treatment modality. Radiation therapy is used for lesions that are symptomatic and for larger lesions that, if they progress, risk leading to pain, fracture, and/or a more difficult stabilization procedure. Early use of radiation and medications that inhibit osteoclasts (bisphosphonates [eg, zoledronate] or denosumab) slow bone destruction. Some tumors are more likely to heal after radiation therapy (eg, breast, prostate, and myeloma) than others (eg, lung cancer and renal cell carcinoma). For this reason, more aggressive surgical treatment is often pursued with these less radioresponsive histologies.Treatment of metastatic bone tumors depends on the type of tissue involved (which organ tissue type). Radiation therapy, combined with selected chemotherapeutic or hormonal drugs, is the most common treatment modality. Radiation therapy is used for lesions that are symptomatic and for larger lesions that, if they progress, risk leading to pain, fracture, and/or a more difficult stabilization procedure. Early use of radiation and medications that inhibit osteoclasts (bisphosphonates [eg, zoledronate] or denosumab) slow bone destruction. Some tumors are more likely to heal after radiation therapy (eg, breast, prostate, and myeloma) than others (eg, lung cancer and renal cell carcinoma). For this reason, more aggressive surgical treatment is often pursued with these less radioresponsive histologies.
If bone destruction is extensive, resulting in impending or actual pathologic fracture, surgical fixation with trauma implants or resection and endoprosthetic reconstruction may be required to provide stabilization, improve pain, and maintain quality of life and independence. When the primary cancer has been resected and there is only oligometastatic bone disease (especially if the metastatic lesion appears delayed ≥ 1 year after the primary tumor treatment), en bloc excision sometimes combined with radiation therapy, chemotherapy, or both rarely may be curative. Insertion of methyl methacrylate into the spine (kyphoplasty or vertebraplasty) relieves pain and expands and stabilizes compression fractures that do not have epidural soft tissue extension. Similar minimally invasive surgical techniques are rapidly gaining favor in the treatment of metastatic bone disease of the pelvis and extremities.


This image shows bone destruction due to a metastasis secondary to renal cell carcinoma in the proximal femur. The location and extent of bone destruction make the risk of fracture extremely high (impending fracture).
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.


This radiograph shows a large metastatic lytic lesion of the femoral medial condyle with impending pathologic fracture.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
This image shows bone destruction due to a metastasis secondary to renal cell carcinoma in the proximal femur. The location and extent of bone destruction make the risk of fracture extremely high (impending fracture).
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
This radiograph shows a large metastatic lytic lesion of the femoral medial condyle with impending pathologic fracture.
Image courtesy of Michael J. Joyce, MD, and David M. Joyce, MD.
Multiple Myeloma Bone Tumors
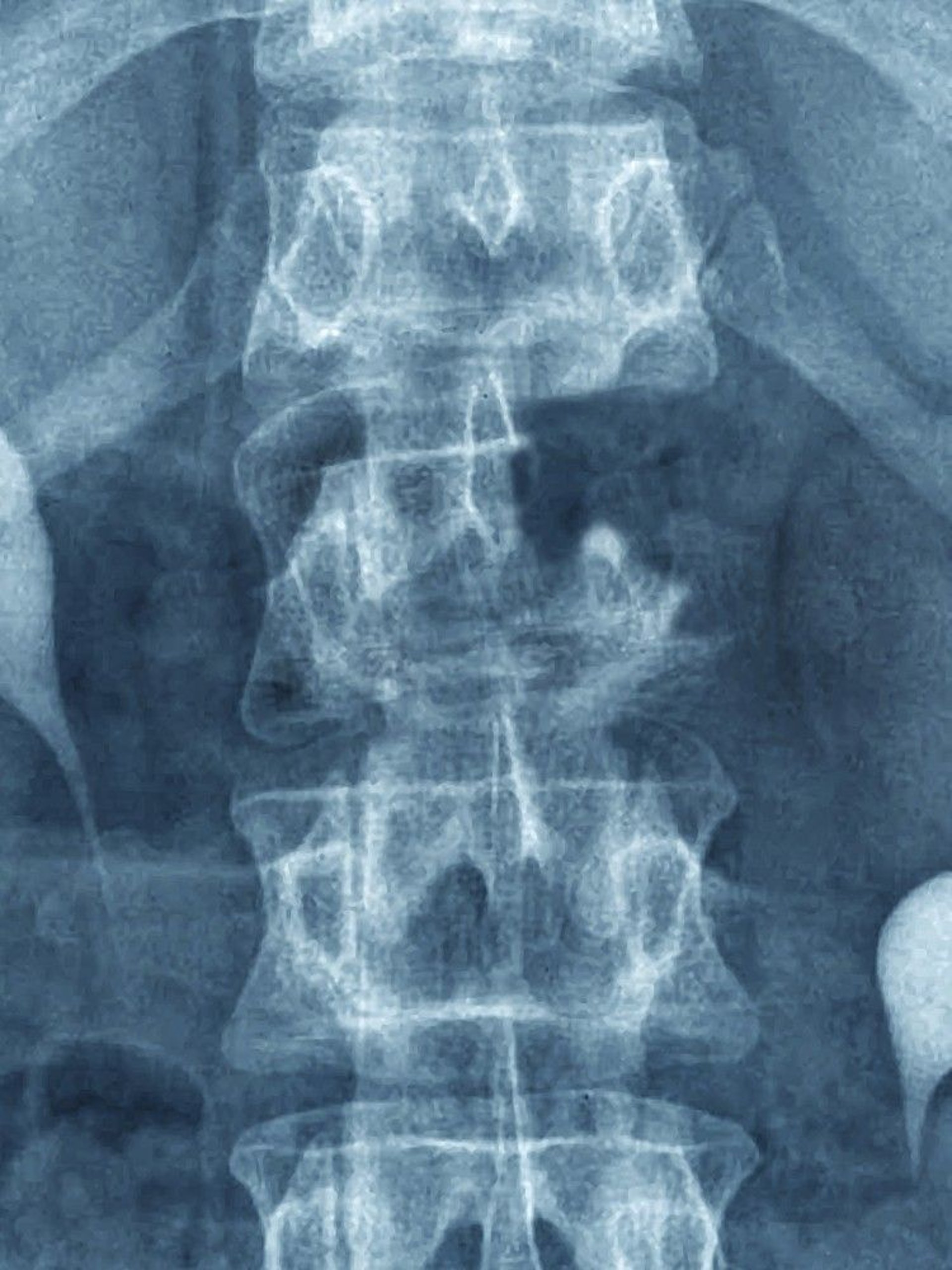
Multiple myeloma, the most common primary malignant bone tumor, occurs mostly in older adults. It is often considered a marrow cell tumor within the bone rather than a primary bone tumor because it is of hematopoietic derivation (see also Multiple Myeloma). Even if multiple myeloma is considered a hematologic tumor, the identified skeletal abnormality must be differentiated from other bone tumors. It is a plasma cell neoplasm characterized by clonal plasma cell growth. Diagnosis can be achieved by serum and urine protein electrophoresis, which will identify a monoclonal spike in the vast majority of patients related to the overproduced immunoglobulin, typically IgG, IgA or IgM. The diagnosis is then confirmed with bone marrow biopsy.
Tumor development and progression is usually multicentric. However, it may also present as an isolated lesion without systemic marrow involvement, which is called a plasmacytoma. Unlike in metastatic disease, a radionuclide bone scan will not reliably show lesions and skeletal surveys (whole body radiographs) should be done. Skeletal surveys typically show sharply circumscribed lytic lesions (punched-out lesions) or diffuse demineralization.


Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Certain bony lesions respond quite well to radiation therapy.
Key Points
Carcinomas of breast, lung, prostate, and kidney are the most common sources of metastatic bone tumors.
Bone metastases should be suspected in patients with known cancer, when pain is at more than one site, and/or when findings on imaging studies suggest metastases.
Patients with known solid organ cancer and a new destructive bone lesion may require a biopsy to confirm metastatic disease and exclude a second primary tumor.
Most often, radiation therapy, bisphosphonates, and receptor activator of nuclear factor kappa-B ligand inhibitors (RANKL) (denosumab) are used to slow bone destruction.Most often, radiation therapy, bisphosphonates, and receptor activator of nuclear factor kappa-B ligand inhibitors (RANKL) (denosumab) are used to slow bone destruction.
Pathologic fractures may require treatment with surgery,to fix the fracture or replace the fracture.







