



- Overview of Vasculitis
- Behçet Disease
- Cutaneous Vasculitis
- Eosinophilic Granulomatosis with Polyangiitis (EGPA)
- Giant Cell Arteritis
- Granulomatosis with Polyangiitis (GPA)
- Immunoglobulin A–Associated Vasculitis (IgAV)
- Microscopic Polyangiitis (MPA)
- Polyarteritis Nodosa (PAN)
- Polymyalgia Rheumatica
- Takayasu Arteritis
Cutaneous vasculitis refers to vasculitis affecting small- or medium-sized vessels in the skin and subcutaneous tissue but not the internal organs. Cutaneous vasculitis may be limited to the skin, or may be a component of a systemic primary or secondary vasculitic disorder. Purpura, petechiae, or ulcers may develop. Diagnosis requires biopsy. Treatment depends on etiology and extent of disease.

")
")
(See also Overview of Vasculitis.)
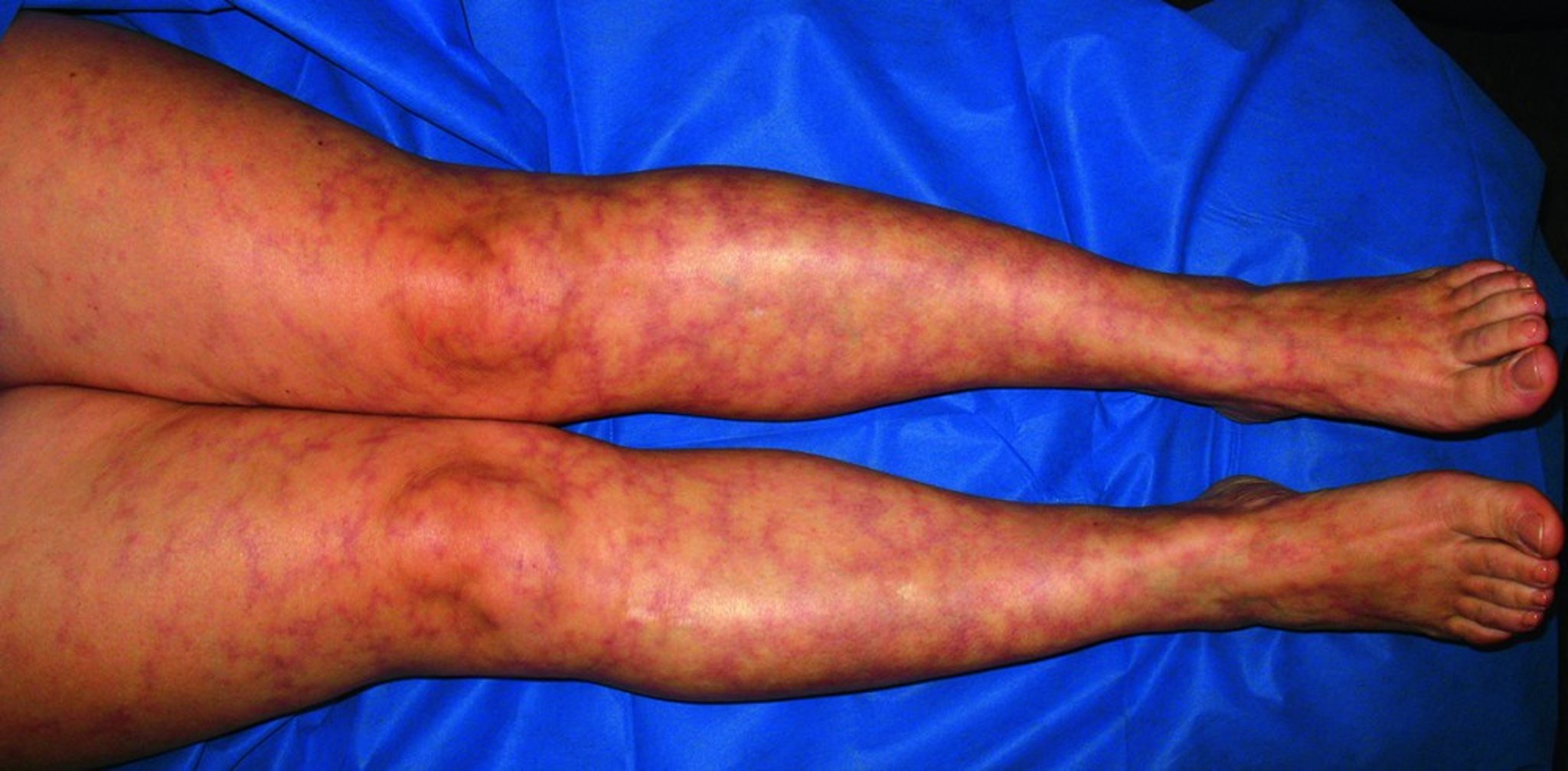
Vasculitis can affect the small- or medium-sized vessels of the skin. Vasculitis affecting the small vessels of the skin (eg, arterioles, capillaries, postcapillary venules) tends to cause lesions such as purpura, petechiae, and possibly shallow ulcers. Livedo reticularis, nodules, and deep ulcers are usually caused by vasculitis of deeper, medium or large vessels. Any primary or secondary vasculitis can affect the skin, including that due to serum sickness, infections (eg, hepatitis C), cancers, rheumatologic or other autoimmune disorders, and hypersensitivity to medications.

© Springer Science+Business Media


Image courtesy of Karen McKoy, MD.


© Springer Science+Business Media
Terms used to describe cutaneous vasculitis can overlap and have been used inconsistently in the literature:
Cutaneous vasculitis: This term describes vasculitis that affects the skin but not the internal organs.
Cutaneous small-vessel vasculitis (CSVV): This term describes vasculitis that affects the small vessels of the skin but not the internal organs. CSVV sometimes refers to small-vessel vasculitis of unknown cause (also called idiopathic cutaneous small-vessel vasculitis).
Leukocytoclastic vasculitis: This is a histopathologic term that describes a vasculitis of the small vessels of the skin, so-called because inflammation consists initially of neutrophils, which after degranulation result in deposition of nuclear debris (leukocytoclasis) in the vessel wall.
Hypersensitivity vasculitis: This term previously used to mean CSVV but is now usually not used because the cause of CSVV is usually not hypersensitivity. However, hypersensitivity vasculitis is sometimes used to refer to CSVV caused by a known medication or infection.
Symptoms and Signs of Cutaneous Vasculitis
Patients may present with skin symptoms such as lesions, including palpable purpura, petechiae, urticaria, ulcers, livedo reticularis, and nodules. If skin involvement is secondary to a systemic vasculitis, symptoms may also include fever, arthralgias, other organ involvement, or a combination.
Diagnosis of Cutaneous Vasculitis
Exclusion of clinically evident causes of systemic vasculitis
Routine tests (eg, complete blood count, serum creatinine, aminotransferases, erythrocyte sedimentation rate and/or C-reactive protein, urinalysis with urinary sediment, chest radiograph)
Biopsy
Tests to identify the type and etiology of systemic vasculitis (eg, cryoglobulins, antineutrophil cytoplasmic antibodies, hepatitis B and C antibodies, C3 and C4 complement levels, rheumatoid factor, blood cultures, protein electrophoresis)
A diagnosis of vasculitis limited to the skin requires a complete history and physical examination. Evaluation is focused at identifying causes, such as new medications or infections, and excluding manifestations of inflammation or vasculitis in other organs, such as
Lungs: Shortness of breath, cough, hemoptysis, and signs of consolidation
Kidneys: New-onset hypertension or edema
Nerves: New-onset asymmetric weakness or paresthesias
Intestine: New-onset abdominal pain, diarrhea, and bloody stools
Urinalysis should exclude blood, protein, and red blood cell casts. A chest radiograph is needed to check for infiltrates (suggesting alveolar hemorrhage). Complete blood count and other blood tests are needed to check for anemia, to determine platelet count and serum creatinine level, and to check for elevated levels of acute-phase reactants (eg, erythrocyte sedimentation rate, C-reactive protein). Leukopenia and thrombocytopenia are not typical of cutaneous vasculitis and should prompt consideration of an alternate diagnosis (eg, leukemia, especially in older patients).
Skin biopsy should be done, optimally within 24 to 48 hours after vasculitic lesions appear. Diagnostic yield depends on the depth and timing of the biopsy. Generally, deep punch biopsy or excision biopsy into the subcutis is preferred; these biopsies can sample small- and medium-sized vessels. Shave biopsy is usually inadequate.
If histologic examination detects the following, cutaneous vasculitis is confirmed:
Infiltration of the vessel wall by inflammatory cells, resulting in disruption and destruction of the vessel wall
Intramural and intraluminal fibrin deposition (fibrinoid necrosis)
Extravasation of red blood cells
Nuclear debris (leukocytoclasis)
Direct immunofluorescence staining is needed to check for IgA, IgM, and IgG and complement deposition in and around the vessel wall, which suggests an immune complex–mediated process, a myeloid or lymphoproliferative disorder, or other neoplastic disorder, especially in adults. IgA deposition has been associated with renal, joint, and gastrointestinal manifestations, but IgG and IgM have not. Direct immunofluorescence staining may be positive for IgM or IgG in cryoglobulinemic vasculitis or rheumatoid arthritis and for IgA in immunoglobulin A–associated vasculitis.
Tests done to identify the cause of vasculitis include cryoglobulins, antineutrophil cytoplasmic antibodies (ANCA), hepatitis B and C antibodies, C3 and C4 levels, rheumatoid factor, blood cultures, and serum and urine protein electrophoresis. Other tests are done as needed to identify clinically suspected causes of vasculitis.
Treatment of Cutaneous Vasculitis
Treatment of the cause when possible
Initial medication options include colchicine, hydroxychloroquine, dapsone, or a short course of low-dose corticosteroids as neededInitial medication options include colchicine, hydroxychloroquine, dapsone, or a short course of low-dose corticosteroids as needed
Treatment of cutaneous vasculitis is first directed at any identified cause when possible (eg, hepatitis C causing cryoglobulinemia). If no cause is identified and vasculitis is limited to the skin, treatment is minimal and conservative. Colchicine, hydroxychloroquine, dapsone, or a short course of low-dose corticosteroids can be tried (Treatment of cutaneous vasculitis is first directed at any identified cause when possible (eg, hepatitis C causing cryoglobulinemia). If no cause is identified and vasculitis is limited to the skin, treatment is minimal and conservative. Colchicine, hydroxychloroquine, dapsone, or a short course of low-dose corticosteroids can be tried (1).
Sometimes, more potent immunosuppressants (eg, azathioprine, methotrexate) are used, particularly if lesions ulcerate or if corticosteroids must be taken indefinitely to control symptoms.Sometimes, more potent immunosuppressants (eg, azathioprine, methotrexate) are used, particularly if lesions ulcerate or if corticosteroids must be taken indefinitely to control symptoms.
Treatment reference
1. Micheletti RG. Treatment of cutaneous vasculitis. Front Med (Lausanne). 2022;9:1059612. doi:10.3389/fmed.2022.1059612
Key Points
Cutaneous vasculitis affects small or medium-sized vessels and can be primary or secondary.
Manifestations can include palpable purpura, petechiae, urticaria, ulcers, livedo reticularis, and nodules.
Exclude other causes of vasculitis.
Do routine laboratory tests and biopsy.
Treat the cause when possible.







