








Lumbar puncture is used to do the following:
Evaluate intracranial pressure and cerebrospinal fluid (CSF) composition (see table Cerebrospinal Fluid Abnormalities in Various Disorders)
Therapeutically reduce intracranial pressure (eg, idiopathic intracranial hypertension)
Administer intrathecal drugs or a radiopaque contrast agent for myelography


Cerebrospinal Fluid Abnormalities in Various Disorders
Condition | Pressure* | WBCs/microL* | Predominant Cell Type | Glucose | Protein* |
|---|---|---|---|---|---|
Normal | 100–200 mm H2O | 0–3 | L | 50–100 mg/dL (2.78–5.55 mmol/L) | 20–45 mg/dL |
↑ | 100–10,000 | PMN | ↓ | > 100 mg/dL† | |
Subacute and chronic meningitis (eg, due to TB, Cryptococcus infection, sarcoidosis, leukemia, or carcinoma) | N or ↑ | 100–700 | L | ↓ | ↑ |
Acute syphilitic meningitis | N or ↑ | 25–2000 | L | N | ↑ |
Paretic neurosyphilis | N or ↑ | 15–2000 | L | N | ↑ |
Autoimmune encephalitis | N | N or ↑ | L | N | N or ↑ |
Lyme disease of CNS | N or ↑ | 0–500 | L | N | N or ↑ |
N or ↑ | 0–1000 | L | N | ↑ | |
Viral infections | N or ↑ | 100–2000 | L | N | N or ↑ |
↑ | N | L | N | N or ↓ | |
↑ | Bloody | RBC | N | ↑ | |
Cerebral thrombosis | N or ↑ | 0–100 | L | N | N or ↑ |
N | 0–50 | L | N | N or ↑ | |
N | 0–50 | L | N | N or ↑ | |
N | 0–100 | L | N | > 100 mg/dL | |
Lead encephalopathy | ↑ | ↑ | L | N | ↑ |
* Figures given for pressure, cell count, and protein are approximations; exceptions are common. Similarly, PMNs may predominate in disorders usually characterized by lymphocyte response, especially early in the course of viral infections or tuberculous meningitis. Alterations in glucose are less variable and more reliable. | |||||
† Up to 14% of patients may have a CSF protein level < 100 mg/dL in the initial lumbar puncture sample. | |||||
CNS = central nervous system; L = lymphocyte; N = normal; PMN = polymorphonuclear leukocyte; ↑= increased; ↓= decreased. | |||||
Relative contraindications include
Infection at the puncture site
Bleeding diathesis
Increased intracranial pressure due to an intracranial mass lesion, obstructed CSF outflow (eg, due to aqueductal stenosis or Chiari I malformation), or spinal cord CSF blockage (eg, due to tumor cord compression)
If papilledema or focal neurologic deficits are present, CT or MRI should be done before lumbar puncture to rule out the presence of a mass that could precipitate transtentorial or cerebellar herniation.
Lumbar puncture procedure
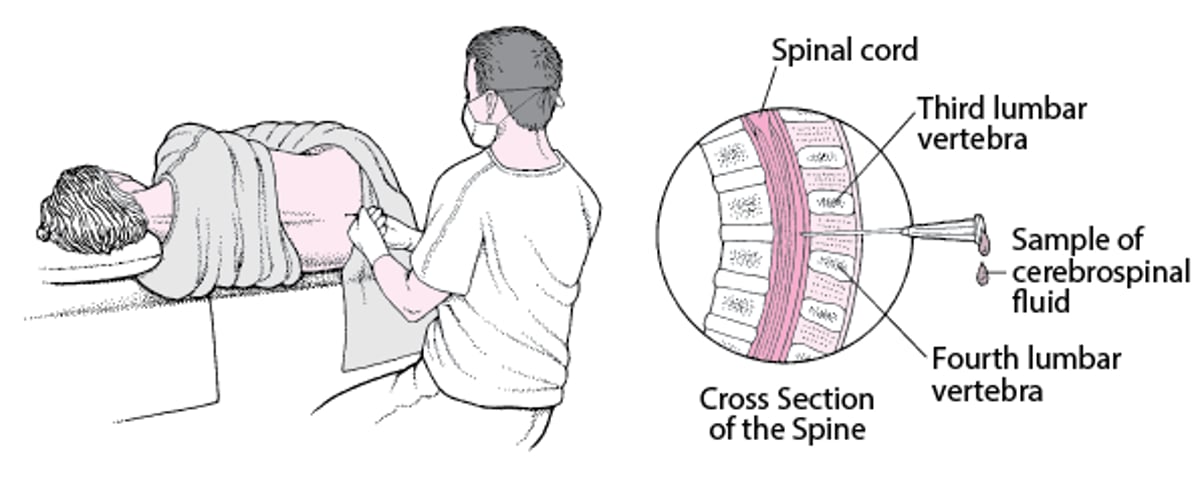
For the procedure, the patient is typically in the left lateral decubitus position. A cooperative patient is asked to hug the knees and curl up as tightly as possible. Assistants may have to hold patients who cannot maintain this position, or the spine may be flexed better by having patients, particularly obese patients, sit on the side of the bed and lean over a bedside tray table.
An area 20 cm in diameter is washed with iodine, then wiped with alcohol to remove the iodine and prevent its introduction into the subarachnoid space. A lumbar puncture needle with stylet is inserted into the L3-to-L4 or L4-to-L5 interspace (the L4 spinous process is typically on a line between the posterior-superior iliac crests); the needle is aimed rostrally toward the patient’s umbilicus and, if the patient is supine, always kept parallel to the floor. Entrance into the subarachnoid space is often accompanied by a discernible pop; the stylet is withdrawn to allow CSF to flow out.
Opening pressure is measured with a manometer; 4 tubes are each filled with about 2 to 10 mL of CSF for testing. The puncture site is then covered with a sterile adhesive strip.
A post–lumbar puncture headache occurs in about 10% of patients.
Lumbar Puncture
This lumbar puncture is done with the patient in the lateral decubitus position and the lumbar puncture needle inserted at the L3-L4 interspace. |

CSF color
Normal CSF is clear and colorless; ≥ 300 cells/microL produces cloudiness or turbidity.
Bloody fluid may indicate a traumatic puncture (pushing the needle in too far, into the venous plexus along the anterior spinal canal) or subarachnoid hemorrhage. A traumatic puncture is distinguished by
Gradual clearing of the CSF between the 1st and 4th tubes (confirmed by decreasing the red blood cell [RBC] count)
Absence of xanthochromia (yellowish CSF due to lysed RBCs) in a centrifuged sample
Fresh, uncrenated RBCs
With intrinsic subarachnoid hemorrhage, the CSF remains uniformly bloody throughout collection; xanthochromia is often present if several hours have passed after ictus; and RBCs are usually older and crenated. Faintly yellow fluid may also be due to senile chromogens, severe jaundice, or increased protein (> 100 mg/dL).
CSF cell count and glucose and protein levels
Cell count and differential and glucose and protein levels aid in the diagnosis of many neurologic disorders (see table Cerebrospinal Fluid Abnormalities in Various Disorders).
Normally, CSF:blood glucose ratio is about 0.6, and except in severe hypoglycemia, CSF glucose is typically > 50 mg/dL (> 2.78 mmol/L).
Increased CSF protein (> 50 mg/dL) is a sensitive but nonspecific index of disease; protein increases to > 500 mg/dL in purulent meningitis, advanced TB meningitis, complete block by a spinal cord tumor, or a bloody puncture. Special examinations for globulin (normally < 15%) and oligoclonal banding aid in diagnosing a demyelinating disorder such as multiple sclerosis. Immunoglobulins in the CSF, usually IgG, can be identified by immunoblotting or immunofixation, in which they are separated by electrophoresis and then stained with antibodies. Alternatively, nephelometry can be used to quantitate protein and immunoglobulins in CSF and serum and thus enable calculation of ratios useful in diagnosing autoimmune disorders that affect the central nervous system (CNS), such as multiple sclerosis. In nephelometry, protein levels are determined by measuring the intensity of light passing through CSF or serum.

CSF staining, testing, and culture
If infection is suspected, the centrifuged CSF sediment is stained for the following:
Bacteria (Gram stain)
Tuberculosis (acid-fast stain or immunofluorescence)
Cryptococcus species (India ink)
Larger amounts of fluid (10 mL) improve the chances of detecting the pathogen, particularly acid-fast bacilli and certain fungi, in stains and cultures. In early meningococcal meningitis or severe leukopenia, CSF protein may be too low for bacterial adherence to the glass slide during Gram staining, producing a false-negative result. Mixing a drop of aseptic serum with CSF sediment prevents this problem. When hemorrhagic meningoencephalitis is suspected, a wet mount is used to search for amebas.
Latex particle agglutination and coagglutination tests may allow rapid bacterial identification, especially when stains and cultures are negative (eg, in partially treated meningitis). CSF should be cultured aerobically and anaerobically and for acid-fast bacilli and fungi.
Except for enteroviruses, viruses are seldom isolated from the CSF. Viral antibody panels are available.
Venereal Disease Research Laboratories (VDRL) testing and cryptococcal antigen testing are often routinely done. Polymerase chain reaction (PCR) tests for herpes simplex virus and other CNS pathogens are increasingly available.
Specialized CSF tests can be done; they include tests for specific antibodies in various disorders, such as autoimmune encephalitis (see also The Diagnosis and Treatment of Autoimmune Encephalitis). The autoimmune encephalitides are antibody-mediated brain disorders that target specific neuronal antigens.







