



Measles is a highly contagious viral infection that is most common among children. It is characterized by fever, cough, coryza, conjunctivitis, an enanthem (Koplik spots) on the oral mucosa, and a maculopapular rash that spreads cephalocaudally. Complications, mainly pneumonia or encephalitis, may be fatal, particularly in medically underserved areas. Diagnosis is usually clinical. Treatment is supportive. Vaccination is effective for prevention.
Topic Resources
")
")
Worldwide, measles infects approximately 10 million people and causes approximately 100,000 to 200,000 deaths each year, primarily in children (1). These numbers can vary dramatically over a short period of time depending on the vaccination status of the population.
Measles is uncommon in the United States because of routine childhood vaccination, and endemic measles was declared eliminated in the United States in 2000. An average of 63 cases/year were reported to the Centers for Disease Control and Prevention (CDC) from 2000 to 2010.
However, in 2019, incidence in the United States rose to 1274 cases, the highest number reported since 1992. That increase primarily was due to the spread among unvaccinated groups (see the CDC's Measles Cases and Outbreaks). Parental refusal of vaccination is becoming more frequent as a cause of the increase in vaccine-preventable diseases in children.
In 2020, only 13 measles cases were reported in the United States amid the COVID-19 global pandemic. In 2022, 121 cases were reported (see the CDC's Measles Cases and Outbreaks).
General reference
1. Patel MK, Goodson JL, Alexander Jr. JP, et al: Progress toward regional measles elimination—worldwide, 2000–2019. MMWR Morb Mortal Wkly Rep 69(45):1700–1705, 2020. doi: 10.15585/mmwr.mm6945a6
Pathophysiology of Measles
Measles is caused by a paramyxovirus and is a human disease with no known animal reservoir or asymptomatic carrier state. It is extremely communicable; the secondary attack rate is > 90% among susceptible people who are exposed.
Measles is spread mainly by secretions from the nose, throat, and mouth during the prodromal or early eruptive stage. Communicability begins several days before and continues until several days after the rash appears. Measles is not communicable once the rash begins to desquamate.
Transmission is typically by large respiratory droplets that are discharged by cough and briefly remain airborne for a short distance. Transmission may also occur by small aerosolized droplets that can remain airborne (and thus can be inhaled) for up to 2 hours in closed areas (eg, in an office examination room). Transmission by fomites seems less likely than airborne transmission because the measles virus is thought to survive only for a short time on dry surfaces.
An infant whose mother has immunity to measles (eg, because of previous illness or vaccination) receives antibodies transplacentally; these antibodies are protective for most of the first 6 to 12 months of life. Lifelong immunity is conferred by infection.
In the United States, almost all measles cases are imported by travelers or immigrants, with subsequent community transmission occurring primarily among unvaccinated people.
Symptoms and Signs of Measles
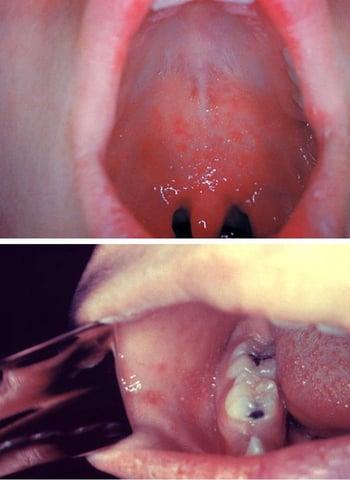
After a 7- to 14-day incubation period, measles begins with a prodrome of fever, coryza, hacking cough, and tarsal conjunctivitis. Koplik spots (which resemble grains of white sand surrounded by red areolae) are pathognomonic. These spots appear during the prodrome before the onset of rash, usually on the oral mucosa opposite the 1st and 2nd upper molars. They may be extensive, producing diffuse mottled erythema of the oral mucosa. Sore throat develops.

The rash appears 3 to 5 days after symptom onset, usually 1 to 2 days after Koplik spots appear. It begins on the face in front of and below the ears and on the side of the neck as irregular macules, soon mixed with papules. Within 24 to 48 hours, lesions spread to the trunk and extremities (including the palms and soles) as they begin to fade on the face. Petechiae or ecchymoses may occur with in severe cases.


During peak disease severity, a patient’s temperature may exceed 40° C, with periorbital edema, conjunctivitis, photophobia, a hacking cough, extensive rash, prostration, and mild itching. Constitutional symptoms and signs parallel the severity of the eruption.
In 3 to 5 days, the fever decreases, the patient feels more comfortable, and the rash fades rapidly, leaving a coppery brown discoloration followed by desquamation.
Patients who are immunocompromised may not have a rash and can develop severe, progressive giant cell pneumonia.
Complications of measles
Complications of measles include
Bacterial superinfection, including pneumonia
Acute thrombocytopenic purpura
Encephalitis
Transient hepatitis
Subacute sclerosing panencephalitis
Bacterial superinfections include pneumonia, laryngotracheobronchitis, and otitis media. Measles transiently suppresses delayed hypersensitivity, which can worsen active tuberculosis and temporarily prevent reaction to tuberculin and histoplasmin antigens in skin tests. Bacterial superinfection is suggested by pertinent focal signs or a relapse of fever, leukocytosis, or prostration.
Pneumonia due to measles virus infection of the lungs occurs in approximately 5% of patients, even during apparently uncomplicated infection. In fatal cases of measles in infants, pneumonia is often the cause of death.
Acute thrombocytopenic purpura may occur after infection resolves and cause a mild, self-limited bleeding tendency; occasionally, bleeding is severe.
Encephalitis occurs in 1/1000 children, usually 2 days to 2 weeks after onset of the rash (1), often beginning with recrudescence of high fever, headache, seizures, and coma. Cerebrospinal fluid usually has a lymphocyte count of 50 to 500/mcL and a mildly elevated protein level but may be normal initially. Encephalitis may resolve in about 1 week or may persist longer, causing morbidity or death.
Transient hepatitis and diarrhea may occur during an acute infection.
Subacute sclerosing panencephalitis (SSPE) is a rare, progressive, ultimately fatal, late complication of measles.
Atypical measles syndrome is a complication that occurred in people vaccinated with the original killed-virus measles vaccines, which were used in the United States from 1963 to 1967 and until the early 1970s in some other countries (2). These older vaccines altered disease expression in some patients who were incompletely protected and subsequently infected with wild-type measles. Measles manifestations developed more suddenly, and significant pulmonary involvement was more common. Confirmed cases have been extremely rare since the 1980s. Atypical measles is of note mainly because patients who received a measles vaccine during that time period may report a history of both measles vaccination and measles infection.
Complications references
1. Centers for Disease Control and Prevention (CDC): Measles: For Healthcare Providers. Accessed March 13, 2023.
2. CDC: Measles prevention. MMWR Suppl 38(9):1–18, 1989.
Diagnosis of Measles
History and physical examination
Serologic testing
Viral detection via culture or reverse transcription–polymerase chain reaction (RT-PCR)
Measles may be suspected in an exposed patient who has coryza, conjunctivitis, photophobia, and cough but is usually suspected only after the rash appears. Diagnosis is usually clinical, by identifying Koplik spots or the rash in an appropriate clinical context. A complete blood count is unnecessary but, if obtained, may show leukopenia with a relative lymphocytosis.
Laboratory confirmation is necessary for public health outbreak control purposes. It is most easily done by demonstration of the presence of measles IgM antibody in an acute serum specimen or by viral culture or RT-PCR of throat swabs, blood, nasopharyngeal swabs, or urine samples. A rise in IgG antibody levels between acute and convalescent sera is highly accurate, but obtaining this information delays diagnosis. All cases of suspected measles should be reported to the local health department even before laboratory confirmation.
Differential diagnosis includes rubella, scarlet fever, drug rash, serum sickness (see table Some Causes of Urticaria), roseola infantum, infectious mononucleosis, erythema infectiosum, and echovirus and coxsackievirus infections (see table Some Respiratory Viruses). Manifestations can also resemble Kawasaki disease. The presenting symptoms and signs may cause diagnostic confusion in areas where measles is very rare.
Some of these conditions can be distinguished from typical measles as follows:
Rubella: A recognizable prodrome is absent, fever and other constitutional symptoms are absent or less severe, postauricular and suboccipital lymph nodes are enlarged (and usually tender), and duration is short.
Drug rash: A rash caused by drug hypersensitivity often resembles the measles rash, but a prodrome is absent, there is no cephalocaudal progression or cough, and there is usually a history of recent drug exposure.
Roseola infantum: The rash resembles that of measles, but it seldom occurs in children > 3 years of age. Initial temperature is usually high, Koplik spots and malaise are absent, and defervescence and rash occur simultaneously.
Treatment of Measles
Supportive care
For children, vitamin AFor children, vitamin A
Treatment of measles is supportive, including for encephalitis.
Patients are most contagious for 4 days after the development of the rash. Patients who are otherwise healthy and can be managed as outpatients should be isolated from others during their illness.
Hospitalized patients with measles should be managed with standard and airborne precautions. Single-patient airborne infection isolation rooms and N-95 respirators or similar personal protective equipment are recommended.
Vitamin A supplementationVitamin A supplementation has been shown to reduce morbidity and mortality due to measles in children in medically underserved areas. Because low serum levels of vitamin A are associated with severe disease due to measles, vitamin A treatment is recommended for all children with measles. The dose is given orally once a day for 2 days and depends on the child’s age:has been shown to reduce morbidity and mortality due to measles in children in medically underserved areas. Because low serum levels of vitamin A are associated with severe disease due to measles, vitamin A treatment is recommended for all children with measles. The dose is given orally once a day for 2 days and depends on the child’s age:
≥ 12 months: 200,000 international units (IU)
6 to 11 months: 100,000 IU
< 6 months: 50,000 IU
In children with clinical signs of vitamin A deficiencyvitamin A deficiency, an additional single, age-specific dose of vitamin A is repeated 2 to 4 weeks later., an additional single, age-specific dose of vitamin A is repeated 2 to 4 weeks later.
Prognosis for Measles
Mortality is approximately 1 to 2/1000 children in the United States, but is much higher in medically underserved countries (1). Undernutrition and vitamin A deficiencyvitamin A deficiency may predispose to mortality.
The CDC estimates that worldwide approximately 134,000 people die each year of measles, typically from complications of pneumonia or encephalitis.
Prognosis reference
1. Centers for Disease Control and Prevention: Global Health: Measles. Accessed 3/13/2023.
Prevention of Measles
A live-attenuated virus vaccine containing measles, mumps, and rubella (MMR) is routinely given to children in most nations that have a robust health care system (see also Childhood Vaccination Schedule).
Two doses are recommended:
The first dose at age 12 to 15 months but can be given as young as age 6 months during a measles outbreak or before international travel
The second dose at age 4 to 6 years
Infants immunized at < 1 year of age still require 2 additional doses given after their first birthday.
MMR vaccination generally provides lasting immunity and has decreased measles incidence in the United States by 99% (1). A large meta-analysis of cohort studies found the effectiveness of the MMR vaccine in preventing measles in children from age 9 months to 15 years was 95% after one dose and 96% after two doses (2).
The vaccine causes mild or inapparent, noncommunicable infection. Fever > 38° C occurs 5 to 12 days after inoculation in 5 to 15% of vaccinees and can be followed by a rash. Central nervous system reactions are exceedingly rare. The MMR vaccine does not cause autism.
MMR is a live vaccine and is contraindicated during pregnancy.
See MMR Vaccine for more information, including indications, contraindications and precautions, dosing and administration, and adverse effects.
Postexposure prophylaxis
Prevention in susceptible contacts is possible by giving the vaccine within 3 days of exposure. If vaccination cannot occur in that timeframe, immune globulin 0.50 mL/kg IM (maximum dose, 15 mL) is given immediately (within 6 days), with vaccination given 5 to 6 months later if medically appropriate.
Exposed patients with severe immunodeficiency, regardless of vaccination status, and pregnant women who are not immune to measles are given immune globulin 400 mg/kg IV.
In an institutional outbreak (eg, schools), susceptible contacts who refuse or cannot receive vaccination and who also have not received immune globulin should be excluded from the affected institution until 21 days after onset of rash in the last case. Exposed, susceptible health care workers should be excluded from duty from 5 days after their first exposure to 21 days after their last exposure, even if they receive postexposure prophylaxis.
Prevention references
1. McLean HQ, Fiebelkorn AP, Temte JL, Wallace GS; Centers for Disease Control and Prevention: Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: Summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 62(RR-04):1–34, 2013.
2. Di Pietrantonj C, Rivetti A, Marchione P, et al: Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst Rev 4(4):CD004407, 2020. doi: 10.1002/14651858.CD004407.pub4
Key Points
Incidence of measles is highly variable depending on the vaccination rate in the population.
Measles is highly transmissible, developing in > 90% of susceptible contacts.
Measles causes approximately 134,000 deaths annually, primarily in children in medically underserved areas; pneumonia is a common cause, whereas encephalitis is less common.
Treatment is mainly supportive, but children should also receive vitamin A supplementation.Treatment is mainly supportive, but children should also receive vitamin A supplementation.
Universal childhood vaccination is imperative unless contraindicated (eg, by active cancer, use of immunosuppressants, or HIV infection with severe immunosuppression).
Give postexposure prophylaxis to susceptible contacts within 3 days of exposure; use vaccine unless contraindicated, in which case give immune globulin.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
CDC: Measles Cases and Outbreaks statistics







