




")
")

The number of undernourished people in the world has been increasing since 2014. In The State of Food Security and Nutrition in the World 2023, the United Nations Food and Agriculture Organization (FAO) reported that almost 735 million people, or 9.2% of the global population, were undernourished in 2023, which is 122 million more people than in 2019, before the pandemic. Most live in countries with high rates of food insecurity. The prevalence of undernutrition in Africa rose from 19.4% in 2021 to 19.7% in 2022. In contrast, in Asia, the prevalence of undernutrition decreased from 8.8% in 2021 to 8.5% in 2022, a decrease of more than 12 million people. However, these numbers are 58 million above prepandemic levels. Nearly 600 million people are predicted to be chronically undernourished in 2030. This estimate is 23 million more than it would have been if the war in Ukraine had not occurred and is 119 million more than it would be if neither the pandemic nor the war in Ukraine had occurred.
Risk Factors for Undernutrition
Undernutrition is caused by social, cultural, and political factors. Poverty remains the leading cause of undernutrition in low, middle-, and high-income nations. War, civil unrest, overpopulation, unsafe housing conditions, infectious diseases, pandemics, and urbanization can all contribute to undernutrition.
Undernutrition is of special concern at certain times (ie, during infancy, early childhood, adolescence, pregnancy, breastfeeding, and old age) because these conditions involve rapid growth and/or increase the need for nutrients.
Infancy and childhood
Infants and children are particularly susceptible to undernutrition because of their high demand for energy and essential nutrients. According to the World Health Organization (WHO), in 2020, 149 million children > 5 years were estimated to be stunted (too short for age) and 45 million were estimated to be wasted (too thin for height [1]). The mortality rate for children < 5 years is the probability that a neonate will die before reaching 5 years of age and is expressed as deaths per 1000 live births. Worldwide, this rate decreased by 59%: from 93/1000 deaths per live births in 1990 to 38% in 2021 (2). Despite this progress, lowering the mortality rate for children < 5 years remains a major public health concern.
Because vitamin K does not readily cross the placenta, neonates may be deficient, so they are given a single injection of vitamin K within 1 hour of birth to prevent hemorrhagic disease of the newborn, a life-threatening disorder. Infants fed only breast milk, which is typically low in vitamin D, are given supplemental vitamin D; they can develop , are given supplemental vitamin D; they can developvitamin B12 deficiency if the mother is vegan.
Inadequately fed infants and children are at risk of protein-energy undernutrition (PEU—previously called protein-energy malnutrition) and deficiencies of iron, folate (folic acid), (folic acid),vitamins A and C, copper, and zinc.
During adolescence, nutritional requirements increase because the growth rate accelerates. Anorexia nervosa may affect adolescent girls in particular.
Pregnancy and breastfeeding
Requirements for nutrients increase during pregnancy (to support the metabolic demands of pregnancy and fetal growth) and breastfeeding. Aberrations of diet, including pica (consumption of nonnutritive substances, such as clay and charcoal), may occur during pregnancy. Anemia due to iron deficiency is common, as is anemia due to folate deficiency, especially among women who have taken oral contraceptives. Vitamin D deficiency is common during late pregnancy, predisposing the child to decreased bone mass. For women who are pregnant or breastfeeding, clinicians may need to recommend diet plans or dietary supplements, especially if nutritional status is compromised.
Old age
Older adults are at high risk of undernutrition because their nutritional needs increase but energy requirements decrease. This disparity requires consumption of nutrient-dense foods.
Aging—even when disease or dietary deficiency is absent—leads to sarcopenia (progressive loss of lean body mass), starting after age 40 and eventually amounting to a muscle loss of about 10 kg (22 lb) in men and 5 kg (11 lb) in women. Undernutrition contributes to sarcopenia, and sarcopenia accounts for many of the complications of undernutrition (eg, decreased nitrogen balance, increased susceptibility to infections).
Causes of sarcopenia include the following:
Decreased physical activity
Decreased food intake
Increased levels of cytokines (particularly interleukin-6)
Decreased levels of growth hormone and mechano growth factor (insulin-like growth factor-3)
In men, decreasing androgen levels
Aging decreases basal metabolic rate (due mainly to decreased fat-free mass), total body weight, height, and skeletal mass; from about age 40 to age 65, mean body fat (as a percentage of body weight) increases to about 30% (from 20%) in men and to 40% (from 27%) in women.
From age 20 to 80, food intake decreases, especially in men.
Anorexia due to aging itself has many causes, including
Reduced receptive relaxation of the stomach’s fundus
Increased release and activity of cholecystokinin (which produces satiation)
Increased leptin (an anorectic hormone produced by fat cells)
Diminished taste and smell, which can decrease eating pleasure but usually decrease food intake only slightly
Depression (a common cause)
Loneliness
Inability to shop or prepare meals
Some chronic disorders
Use of certain medications
Occasionally, anorexia nervosa (sometimes called anorexia tardive in older patients), paranoia, or mania interferes with eating. Dental problems limit the ability to chew and subsequently to digest foods. Swallowing difficulties (eg, due to stroke, other neurologic disorders, esophageal candidiasis, or xerostomia) are common. Poverty or functional impairment limits access to nutrients.
Institutionalized older patients are at particular risk of protein-energy undernutrition. They are often confused and may be unable to express hunger or preferences for foods. They may be physically unable to feed themselves. Chewing or swallowing may be very slow, making it tedious for another person to feed them enough food.
In older patients, particularly those who are institutionalized, inadequate intake and often decreased absorption or synthesis of vitamin D, increased demand for vitamin D, and inadequate exposure to sunshine contribute to vitamin D deficiency and osteomalacia.
Disorders and medical procedures
Diabetes, some chronic disorders that affect the gastrointestinal tract, intestinal resection, and certain other gastrointestinal surgical procedures tend to impair absorption of fat-soluble vitamins, vitamin B12, calcium, and iron. Gluten enteropathy, pancreatic insufficiency, or other disorders can result in malabsorption. Decreased absorption possibly contributes to iron deficiency and osteoporosis.
Liver disorders impair storage of vitamins A and B12 and interfere with metabolism of protein and energy sources. Renal insufficiency predisposes to protein, iron, and vitamin D deficiencies.
Anorexia causes some patients with cancer or depression and many with AIDS to consume inadequate amounts of food.
Infections, trauma, hyperthyroidism, extensive burns, and prolonged fever increase metabolic demands. Any condition that increases cytokines may be accompanied by muscle loss, lipolysis, low albumin levels, and anorexia.
Vegetarian and vegan diets
Iron deficiency can occur in people who follow an ovo-lacto diet (although such a diet can be compatible with good health). People who follow a vegan diet may develop vitamin B12 deficiency unless they consume yeast extracts or Asian-style fermented foods. Their intake of calcium, iron, and zinc also tends to be low.
Fad diets
Some fad diets result in vitamin, mineral, and protein deficiencies; cardiac, renal, and metabolic disorders; and sometimes death. Very low calorie diets (< 400 kcal/day) cannot sustain health for long.
A fruit-only diet is not recommended because it is deficient in protein, sodium, and many micronutrients.
Medications and nutritional supplements
Many medications (eg, appetite suppressants, digoxin, glucagon-like peptide-1 [GLP-1] receptor agonists) decrease appetite; others impair nutrient absorption or metabolism. Some medications and other substances (eg, stimulants) have catabolic effects. Certain medications can impair absorption of many nutrients; eg, antiseizure medications can impair absorption of vitamins.Many medications (eg, appetite suppressants, digoxin, glucagon-like peptide-1 [GLP-1] receptor agonists) decrease appetite; others impair nutrient absorption or metabolism. Some medications and other substances (eg, stimulants) have catabolic effects. Certain medications can impair absorption of many nutrients; eg, antiseizure medications can impair absorption of vitamins.
Alcohol or substance dependency
Patients with alcohol or substance dependency may neglect their nutritional needs. Absorption and metabolism of nutrients may also be impaired. People with IV drug use disorders typically become undernourished, as do people with alcohol use disorder who consume ≥ 1 quart of hard liquor/day. Alcohol use disorder can cause deficiencies of magnesium, zinc, and certain vitamins, including thiamine.1 quart of hard liquor/day. Alcohol use disorder can cause deficiencies of magnesium, zinc, and certain vitamins, including thiamine.
Risk factor references
1. World Health Organization (WHO): Infant and young child feeding, 2021. Accessed September 20, 2023.
2. Unicef: Under-Five Mortality, 2023. Accessed September 20, 2023.
Symptoms and Signs of Undernutrition
Symptoms vary depending on the cause and type of undernutrition (eg, protein-energy undernutrition, vitamin deficiency).
Evaluation of Undernutrition
Diagnosis of undernutrition is based on results of medical and diet histories, physical examination, body composition analysis, and selected laboratory tests. Explicit consensus criteria have been proposed but are not yet universally adopted (1).
History
History should include questions about
Dietary intake: See Mini Nutritional Assessment (MNA), a nutrition screening and assessment tool that can identify patients age ≥ 65 who are undernourished or at risk of undernutrition (2)
Chronic disease: See the Global Diet Quality Score (GDQS), a quick way to assess the risk of undernutrition in people with chronic disorders (3)
Recent changes in weight
Risk factors for undernutrition, including drug and alcohol use
Unintentional loss of ≥ 10% of usual body weight during a 3-month period indicates a high probability of undernutrition. Social history should include questions about food security and the patient's ability to shop and cook.
Review of systems should focus on symptoms of nutritional deficiencies (see table Symptoms and Signs of Nutritional Deficiency). For example, impaired night vision may indicate vitamin A deficiency.
Symptoms and Signs of Nutritional Deficiency
Area/System | Symptom or Sign | Deficiency |
|---|---|---|
General appearance | Wasting | Energy |
Skin | Rash | Many vitamins, zinc, essential fatty acids |
Rash in sun-exposed areas | Niacin (pellagra) | |
Easy bruising | ||
Hair and nails | Thinning or loss of hair | |
Premature whitening of hair | ||
Spooning (upcurling) of nails | ||
Eyes | Impaired night vision | |
Corneal keratomalacia (corneal drying and clouding) | Vitamin AVitamin A | |
Mouth | Cheilosis and glossitis | Riboflavin, niacin, pyridoxine, iron |
Bleeding gums | Vitamin C, riboflavin | |
Extremities | Edema | Protein |
Neurologic | Paresthesias or numbness in a stocking-glove distribution | Thiamin (beriberi) |
Tetany | ||
Cognitive and sensory deficits | Thiamin, niacin, pyridoxine, , pyridoxine,vitamin B12 | |
Dementia | Thiamin, niacin, vitamin B12 | |
Musculoskeletal | Wasting of muscle | Protein |
Bone deformities (eg, bowlegs, knocked knees, curved spine) | Vitamin D, calcium | |
Bone tenderness | Vitamin D | |
Joint pain or swelling | Vitamin C | |
Gastrointestinal | Diarrhea | Protein, niacin, folate, vitamin B12 |
Diarrhea and dysgeusia | Zinc | |
Dysphagia or odynophagia (due to Plummer-Vinson syndrome) | Iron | |
Endocrine | Thyromegaly |
Physical examination
Physical examination should include
Measurement of height and weight
Inspection of body fat distribution
Anthropometric measurements of lean body mass
Body mass index (BMI = weight[kg]/height[m]2) adjusts weight for height. If weight is < 80% of what is predicted for the patient’s height or if BMI is ≤ 18, undernutrition should be suspected. Although these findings are useful in diagnosing undernutrition and are acceptably sensitive, they lack specificity.

The mid upper arm muscle area estimates lean body mass. This area is derived from the triceps skinfold thickness (TSF) and mid upper arm circumference. Both are measured at the same site, with the patient’s right arm in a relaxed position. The average mid upper arm circumference is about 34.1 cm for men and 31.9 cm for women (4). The formula for calculating the mid upper arm muscle area in cm2 is as follows:


This formula corrects the upper arm area for fat and bone. Average values for the mid upper arm muscle area are 54 ± 11 cm2 for men and 30 ± 7 cm2 for women. A value < 75% of this standard (depending on age) indicates depletion of lean body mass (see table Mid Upper Arm Muscle Area in Adults). This measurement may be affected by physical activity, genetic factors, and age-related muscle loss.
Mid Upper Arm Muscle Area in Adults
Percentage of Standard (%) | Men (cm2) | Women (cm2) | Muscle Mass |
|---|---|---|---|
100 ± 20* | 54 ± 11 | 30 ± 7 | Adequate |
75 | 40 | 22 | Marginal |
60 | 32 | 18 | Depleted |
50 | 27 | 15 | Wasted |
* Mean mid upper arm muscle mass ± 1 standard deviation. | |||
From the National Health and Nutrition Examination Surveys I and II. | |||
Physical examination should focus on signs of specific nutritional deficiencies. Signs of protein-energy undernutrition (eg, edema, muscle wasting, skin changes) should be sought. Examination should also focus on signs of conditions that could predispose to nutritional deficiencies, such as dental problems. Mental status should be assessed because depression and cognitive impairment can lead to weight loss.
The following assessment tools may be useful:
The widely used Subjective Global Assessment (SGA) uses information from the patient history (eg, weight loss, change in intake, gastrointestinal symptoms), physical examination findings (eg, loss of muscle and subcutaneous fat, edema, ascites), and the clinician’s judgment of the patient’s nutritional status.
The Mini Nutritional Assessment (MNA®) has been validated and is widely used, especially in older patients. The MNA consists of 18 scored questions that are divided into four sections: anthropometric measurements, comprehensive assessment, dietary history, and metabolic stress. The possible total score is 30; scores of ≥ 24 indicate normal nutritional status, scores between 17 and 23.5 indicate risk of undernutrition, and scores of < 17 points indicate undernutrition (5, 6, 7). The MNA Short Form (MNA-SF) only includes six elements and thus is faster and easier to use. A score of ≤ 11 points (out of a total of 14) indicates risk of undernutrition. In such cases, the complete MNA should be done (8).
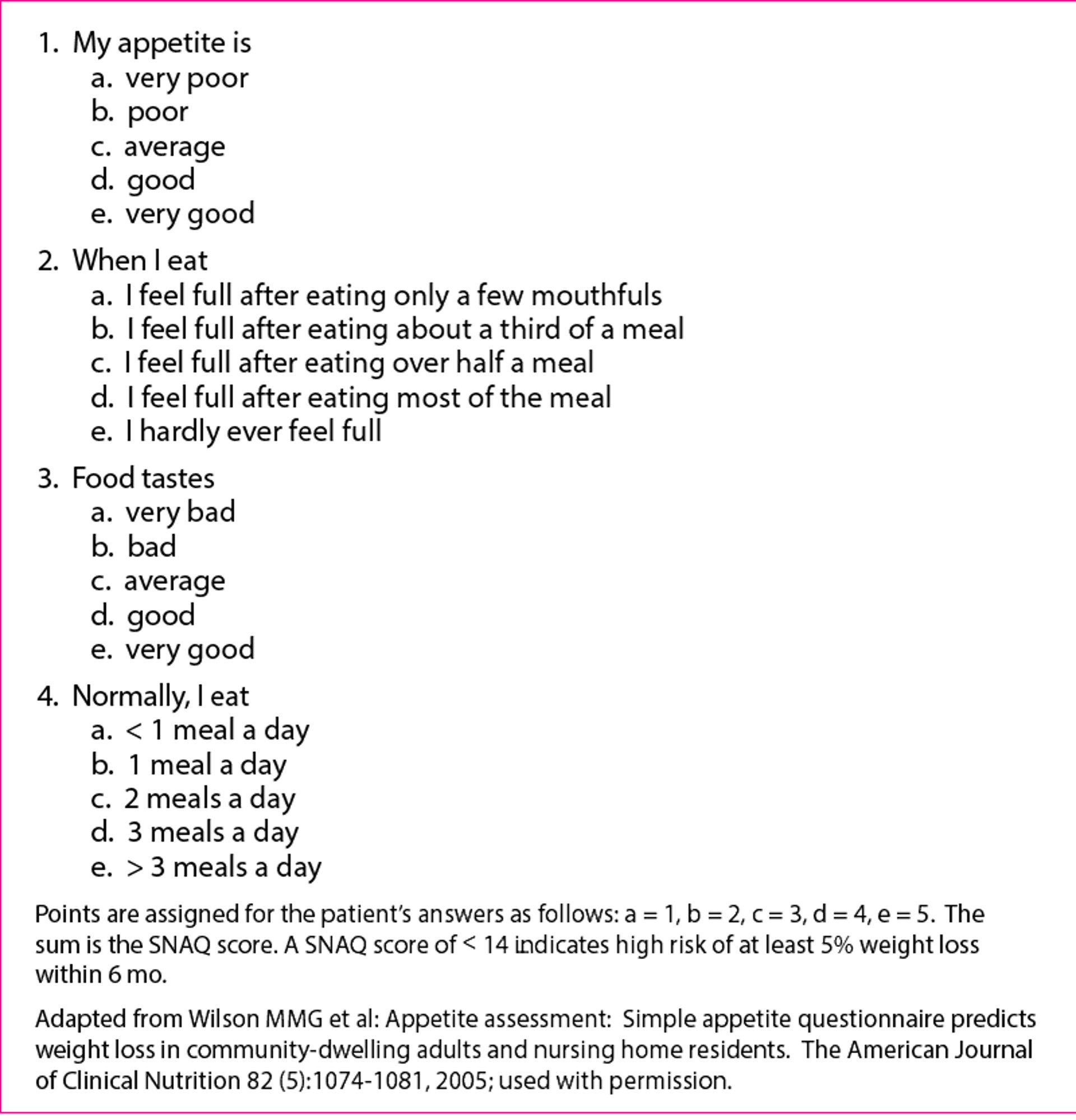
The Simplified Nutrition Assessment Questionnaire (SNAQ), a simple, validated method of predicting future weight loss, may be used.
Simplified Nutrition Assessment Questionnaire (SNAQ)

Testing
The extent of laboratory testing needed is unclear and may depend on the patient’s circumstances. If the cause is obvious and correctable (eg, a wilderness survival situation), testing is probably of little benefit. Other patients may require more detailed evaluation.
Serum albumin measurementSerum albumin measurement is the laboratory test most often used. Decreases in albumin and other proteins (eg, prealbumin [transthyretin], transferrin, retinol-binding protein) may indicate protein deficiency or protein-energy undernutrition (PEU). As undernutrition progresses, albumin decreases slowly; prealbumin, transferrin, and retinol-binding protein decrease rapidly. Albumin measurement is inexpensive and predicts morbidity and mortality better than measurement of the other proteins. However, the correlation of albumin with morbidity and mortality may be related to nonnutritional as well as nutritional factors. Inflammation produces cytokines that cause albumin and other nutritional protein markers to extravasate, decreasing serum levels. Because prealbumin, transferrin, and retinol-binding protein decrease more rapidly during starvation than does albumin, their measurements are sometimes used to diagnose or assess the severity of acute starvation. However, whether they are more sensitive or specific than albumin is unclear.
Total lymphocyte count, which often decreases as undernutrition progresses, may be determined. Undernutrition causes a marked decline in CD4+ T lymphocytes, so this count may not be useful in patients who have AIDS.
Urinary creatinine is related to muscle mass. Urinary creatinine excretion over a 24-hour period can be used to compute the creatinine height index (CHI [%]), which reflects lean muscle mass. The CHI is calculated as (24-hour urine creatinine x 100)/ideal creatinine excretion for height (obtained from standard tables). The CHI indicates extent of muscle depletion as follows: > 30% is severe, 15 to 30% is moderate, and 5 to 15% is mild (9).
Skin tests using antigens can detect impaired cell-mediated immunity in PEU and in some other disorders of undernutrition.
Other laboratory tests, such as measuring vitamin and mineral levels, are used selectively to diagnose specific deficiencies.
Evaluation references
1. Cederholm T, Jensen GL, Correia MITD, et al: GLIM (Global Leadership Initiative on Malnutrition) criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. Clin Nutr 38 (1):1–9, 2019. doi: 10.1016/j.clnu.2018.08.002
2. Guigoz Y, Vellas B: Nutritional assessment in older adults: MNA® 25 years of a screening tool and a reference standard for care and research; What next? J Nutr Health Aging 25 (4):528–583, 2021. doi: 10.1007/s12603-021-1601-y
3. Bromage S, Batis C, Bhupathiraju SN, et al: Development and validation of a novel food-based Global Diet Quality Score (GDQS). J Nutr 151 (12 Suppl 2):75S–92S, 2021. doi: 10.1093/jn/nxab244
4. Fryar CD, Gu Q, Ogden CL, Flegal KM: Anthropometric reference data for children and adults: United States, 2011–2014. National Center for Health Statistics. Vital Health Stat 3 (39), 2016.
5. Laporte M, Keller HH, Payette H. et al: Validity and reliability of the new Canadian Nutrition Screening Tool in the ‘real-world’ hospital setting. Eur J Clin Nutr 69 (5):558–564, 2015. doi: 10.1038/ejcn.2014.270 Epub 2014 Dec 17.
6. Kaiser MJ, Bauer JM, Rämsch C, et al: Frequency of malnutrition in older adults: A multinational perspective using the mini nutritional assessment. J Am Geriatr Soc 58 (9):1734–1738, 2010. doi: 10.1111/j.1532-5415.2010.03016.x
7. Guigoz Y: The Mini Nutritional Assessment (MNA) review of the literature—What does it tell us? J Nutr Health Aging 10 (6):466–485; discussion 485–487, 2006.
8. Soysal P, Veronese N, Arik F, et al: Mini Nutritional Assessment Scale-Short Form can be useful for frailty screening in older adults. Clin Interv Aging 14:693–699, 2019. doi: 10.2147/CIA.S196770 eCollection 2019.
9. Hamada Y: Objective data assessment (ODA) methods as nutritional assessment tools. J Med Invest 62 (3–4):119–122, 2015. doi: 10.2152/jmi.62.119
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
The State of Food Security and Nutrition in the World 2023: This report discusses global hunger, malnutrition, food insecurity, and the effects of urbanization on food systems, including the availability and affordability of healthful diets.
Drugs Mentioned In This Article






