


Pathophysiology of Osteoporosis
Bone is continually being formed and resorbed. Normally, bone formation and resorption are closely balanced. Osteoblasts (cells that make the organic matrix of bone and then mineralize bone) and osteoclasts (cells that resorb bone) are regulated by parathyroid hormone (PTH), calcitonin, estrogen, vitamin D, various cytokines, and other local factors such as prostaglandins.
Peak bone mass in men and women occurs around age 30. Men have higher bone mass than women. (Previous data suggesting people with African ancestry achieve higher peak bone mass are currently being questioned.) After achieving its peak, bone mass plateaus for approximately 10 years, during which time bone formation approximately equals bone resorption. Beginning with menopause, bone loss accelerates in women to approximately 2% a year for approximately 10 years and then the rate of loss decelerates (1).
Osteoporotic bone loss affects cortical and trabecular (cancellous) bone. Cortical thickness and the number and size of trabeculae decrease, resulting in increased porosity. Trabeculae may be disrupted or entirely absent. Trabecular bone loss occurs more rapidly than cortical bone loss because trabecular bone is more porous and bone turnover is higher. However, loss of both types contributes to skeletal fragility.

Fragility fractures
A fragility fracture is one that occurs after less trauma than might be expected to fracture a normal bone. Fractures resulting from falls from a standing height or less, including falls out of bed, are typically considered fragility fractures. The most common sites for fragility fractures are the following:
Spine (thoracic and lumbar vertebral compression fractures—the most common osteoporosis-related fracture)
Other sites may include the proximal humerus and pelvis.
Fractures at sites such as the nose, ribs, clavicle, patella, and metatarsals are not considered osteoporosis-related fractures.
Pathophysiology reference
1. Finkelstein JS, Brockwell SE, Mehta V, et al. Bone mineral density changes during the menopause transition in a multiethnic cohort of women. J Clin Endocrinol Metab. 93(3):861-868, 2008. doi:10.1210/jc.2007-1876
Classification of Osteoporosis
Osteoporosis can develop as a primary disorder of bone turnover or secondarily due to some other factor. The sites of fracture are similar in primary and secondary osteoporosis.
Primary osteoporosis
Nearly all occurrences of osteoporosis in men and women are primary, without an identifiable underlying cause. Most cases occur in postmenopausal women and older men. However, certain conditions may accelerate bone loss in patients with primary osteoporosis. Gonadal insufficiency is an important factor in both men and women; other factors include decreased calcium intake, low vitamin D levels, certain medications, and hyperparathyroidism. Some patients have an inadequate intake of calcium during the bone growth years of adolescence and thus never achieve ideal peak bone mass.
The major mechanism of bone loss is increased bone resorption, resulting in decreased bone mass and microarchitectural deterioration, but sometimes bone formation is impaired. The mechanisms of bone loss may involve the following:
Local changes in cytokine production, particularly involving cytokines such as receptor activator of nuclear factor kappa-B ligand [RANKL] that increase bone resorption by promoting differentiation and maturation of active osteoclasts
Impaired formation response during bone remodeling, probably caused by age-related decline in the number and activity of osteoblasts, partly related to cytokine-mediated increases in the protein sclerostin
Other factors that affect bone resorption such as parathyroid hormone (PTH) and vitamin D level abnormalities
Idiopathic osteoporosis refers to the rare cases of fragility fractures in children, adolescents, premenopausal women, or men < 50 years with normal gonadal function and no detectable secondary cause, including those with low bone mass for age (low Z-scores on dual-energy x-ray absorptiometry [DXA] scans).
Secondary osteoporosis
Secondary osteoporosis accounts for up to 30% of osteoporosis in postmenopausal women, > 50% in premenopausal women, and approximately 50 to 80% in men (1). The causes (see table Causes of Secondary Osteoporosis) may also further accelerate bone loss and increase fracture risk in patients with primary osteoporosis.
Patients with chronic kidney disease may have several factors contributing to low bone mass, including secondary hyperparathyroidism, elevated serum phosphorus, calcitriol deficiency, abnormalities of serum calcium and vitamin D, osteomalacia, and low-turnover bone disorders (adynamic bone disease).
Causes of Secondary Osteoporosis
Cancer (eg, multiple myeloma) |
COPD (chronic obstructive pulmonary disease) due to the disorder and tobacco use, decreased physical activity, and treatment with glucocorticoids |
Medications and substances (eg, chronic use of glucocorticoids, antiseizure medications, medroxyprogesterone, aromatase inhibitors, rosiglitazone, pioglitazone, thyroid replacement therapy, heparin, ethanol, tobacco, , medroxyprogesterone, aromatase inhibitors, rosiglitazone, pioglitazone, thyroid replacement therapy, heparin, ethanol, tobacco,proton pump inhibitors, H2 blockers) |
Endocrine disease (eg, Cushing syndrome, hyperparathyroidism, hyperthyroidism, hypogonadism, hyperprolactinemia, diabetes mellitus) |
Hypercalciuria |
Hypophosphatemia (chronic) |
Immobilization |
Liver disease |
Prolonged weightlessness (as occurs in space flight) |
Classification reference
1. Ebeling PR, Nguyen HH, Aleksova J, et al. Secondary Osteoporosis. Endocr Rev. 2022;43(2):240-313. doi:10.1210/endrev/bnab028
Risk Factors for Osteoporosis
Because mechanical stress, including weight bearing, is necessary for bone growth, immobilization or extended sedentary periods result in bone loss. A low body mass index predisposes to decreased bone mass.
Insufficient dietary intake of calcium, phosphorus, magnesium, and vitamin D predisposes to bone loss, as does endogenous acidosis. Tobacco and alcohol use also adversely affect bone mass. A family history of osteoporosis, particularly a parental history of hip fracture, also increases risk. Patients who have had one fragility fracture are at increased risk of having other clinical (symptomatic) fractures and clinically asymptomatic vertebral compression fractures.
Certain populations, including non-Hispanic White and Asian women, have been thought to have a higher risk of osteoporosis than other groups (1). However, these purported population differences are likely more complex and impacted by social determinants of health. Therefore, fracture risk should likely be assessed using population-specific risk calculators rather than those that incorporate race and ethnicity (2).
Risk factors references
1. Noel SE, Santos MP, Wright NC. Racial and Ethnic Disparities in Bone Health and Outcomes in the United States. J Bone Miner Res. 2021;36(10):1881-1905. doi:10.1002/jbmr.4417
2. Leslie WD; ASBMR Task Force on Clinical Algorithms for Fracture Risk. Effect of Race/Ethnicity on United States FRAX Calculations and Treatment Qualification: A Registry-Based Study. J Bone Miner Res. 2023;38(12):1742-1748. doi:10.1002/jbmr.4896
Symptoms and Signs of Osteoporosis
Patients with osteoporosis are asymptomatic unless a fracture has occurred. Nonvertebral fractures are typically symptomatic, but approximately two-thirds of vertebral compression fractures are asymptomatic (although patients may have underlying chronic back pain due to other causes such as osteoarthritis). A vertebral compression fracture that is symptomatic begins with acute onset of pain that usually does not radiate, is aggravated by weight bearing, may be accompanied by point spinal tenderness, and typically begins to subside in 1 week. Residual pain may last for months or be constant, in which case additional fractures or underlying spine disorders (including malignancy or infection) should be suspected.
Multiple thoracic compression fractures eventually cause dorsal kyphosis, with exaggerated cervical lordosis (dowager hump). Abnormal stress on the spinal muscles and ligaments may cause chronic, dull, aching pain, particularly in the lower back. Patients may have shortness of breath due to the reduced intrathoracic volume and/or early satiety due to the compression of the abdominal cavity as the rib cage approaches the pelvis.
Diagnosis of Osteoporosis
Dual-energy x-ray absorptiometry (DXA)
Presence of a fragility fracture
Although low bone mineral density (and the associated increased risk of fracture) can be suggested by radiographic findings, it must be confirmed by a bone mineral density measurement. Typically DXA is used; quantitative CT scanning can produce similar bone mineral density measurements but is not widely available.
Alternatively, osteoporosis can also be diagnosed based on the occurrence of a fragility fracture, regardless of the bone mineral density score. This diagnostic criterion is particularly relevant for fractures of the spine, hip, humerus, or distal radius.
Dual-energy x-ray absorptiometry (DXA)
Bone mineral density should be measured using a DXA scan to screen people at risk, provide a quantitative measure of bone loss, help predict the risk of fracture, and monitor those undergoing treatment (1 ). In a DXA scan, the target areas, typically the spine and one or both hips, are imaged using x-rays of high and low energy (hence the term "dual energy"). The difference in attenuation between high and low energy beams is a reflection of bone mineral content. The bone mineral content divided by area of bone (also measured in the DXA scan) is the bone mineral density in g/cm2. The presence of significant osteoarthritis in the target areas may increase the reported bone density.
If the spine or a hip is unsuitable for accurate assessment by DXA (eg, because of hardware from prior total hip arthroplasty or spinal fusion surgery), the distal radius can be scanned (called "1/3 radius" on the DXA scan report). The distal radius should also be scanned in a patient with hyperparathyroidism because this is the most common site of bone loss in hyperparathyroidism.
DXA results are reported as T-scores and Z-scores.
The T-score corresponds to the number of standard deviations that the patient's bone mineral density differs from the peak bone mass of a healthy, young person of the same sex and race/ethnicity. The World Health Organization establishes cutoff values for T-scores that define osteopenia and osteoporosis (2). A T-score < -1.0 and > -2.5 defines osteopenia. A T-score ≤ -2.5 defines osteoporosis.
The Z-score corresponds to the number of standard deviations that the patient's bone mineral density differs from that of a person of the same age and sex and should be used for children, premenopausal women, or men < 50 years. If the Z-score is ≤ -2.0, bone mineral density is low for the patient's age and secondary causes of bone loss should be considered.

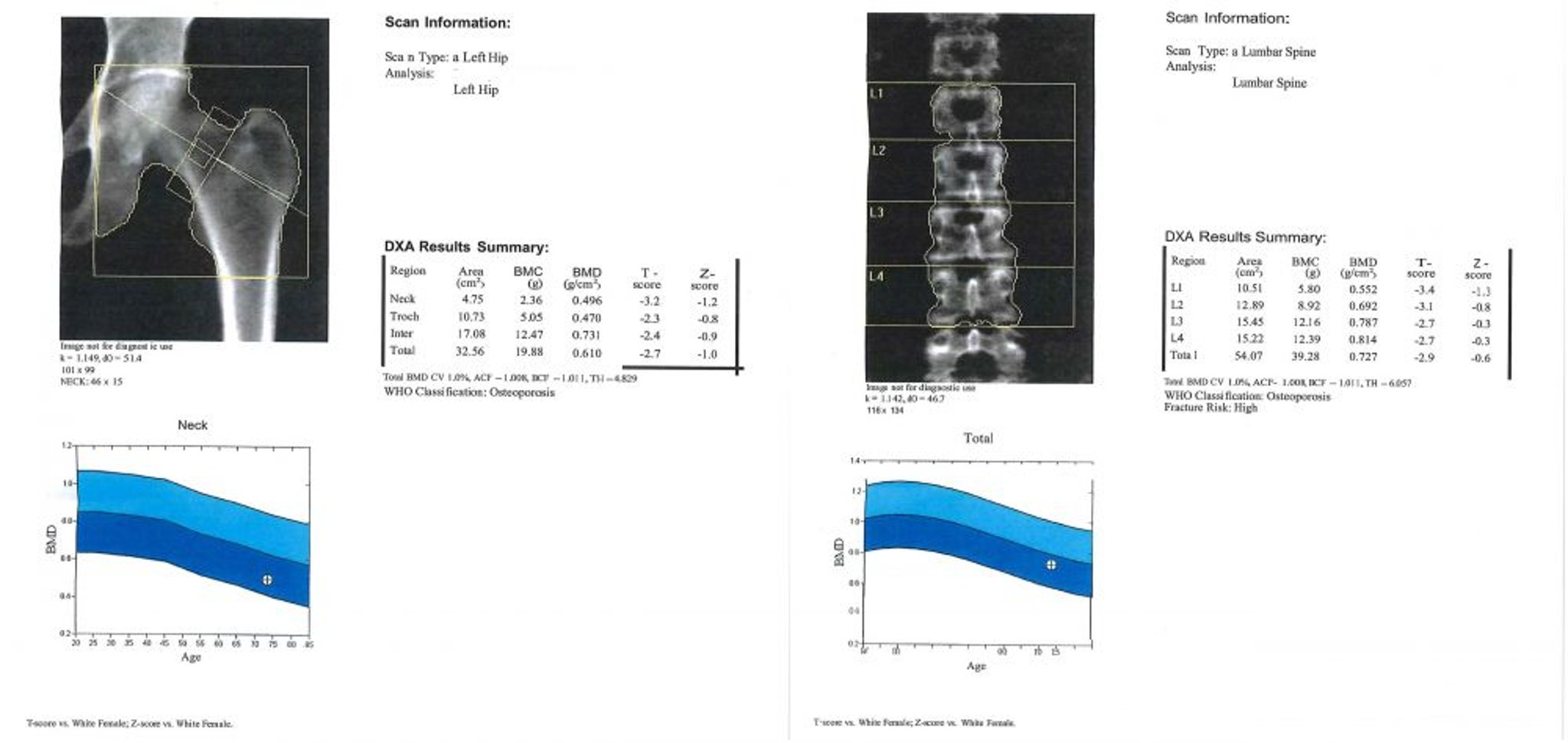
Image courtesy of Marcy B. Bolster, MD.
A DXA scan is recommended for the following patients (1, 3):
All women ≥ 65 years
Women between menopause and age 65 who have risk factors, including a family history of osteoporosis, a low body mass index, cigarette smoking, use of excess alcohol (eg, >3 or more standard drinks per day is used in the FRAX score) and/or use of medications with a high risk of bone loss (eg, glucocorticoids, aromatase inhibitors)
Patients (men and women) of any age who have had 1 or more fragility fractures
Patients with evidence on imaging studies of decreased bone mineral density or asymptomatic vertebral compression fractures incidentally noted on imaging studies
Patients at risk of secondary osteoporosis
DXA scans can also assess vertebral deformities in the lower thoracic and lumbar spine, a procedure termed vertebral fracture assessment (VFA), which can be performed during bone mineral density testing with DXA (4). Vertebral compression deformities in the absence of trauma, even those clinically silent, are diagnostic of osteoporosis and are predictive of an increased risk of future fractures. VFA is more likely to be useful in patients with height loss ≥ 3 cm. If the VFA results reveal suspected abnormalities, radiographs should be performed to confirm the diagnosis.
The need for pharmacologic therapy is based on the probability of future fractures, which is related to DXA results as well as other factors. The fracture risk assessment (FRAX) score (see Fracture Risk Assessment Tool) predicts the 10-year probability of a major osteoporotic (hip, spine, forearm, or humerus) fracture in untreated patients. The score accounts for several significant risk factors for bone loss and fracture, including bone mineral density, multiple clinical features, and country of origin of the patient (to account for observed population differences). If the FRAX score is above certain thresholds (in the United States, a ≥ 20% probability of major osteoporotic fracture or 3% probability of hip fracture), pharmacologic therapy should generally be recommended (5). There are limitations to the use of the FRAX score because it does not account for several factors, including history of falls or increased fall risk, the patient's bone mineral density at the lumbar spine, or family history of vertebral fractures.
Radiographs
Osteoporotic bones typically show decreased radiodensity and loss of trabecular structure but are inadequate for diagnostic purposes. However, radiographs are important for documenting fractures resulting from bone loss. Loss of vertebral body height and increased biconcavity characterize vertebral compression fractures. Thoracic vertebral fractures may cause anterior wedging of the bone. Vertebral fractures most commonly occur at the mid-thoracic level when due to osteoporosis (6). Vertebral fractures above the mid-thoracic region should raise consideration for malignancy or trauma as the etiology. Radiographs of the spine to look for asymptomatic vertebral fragility fractures should be considered in older patients with severe back pain and localized vertebral spinous tenderness and in patients who report > 3 cm height loss.

Photo courtesy of Marcy B. Bolster, MD.
Corticosteroid-related osteoporosis, also called glucocorticoid-induced osteoporosis (GIOP), is most likely to cause vertebral compression fractures but may also cause fractures at other sites where osteoporotic fractures are common (7). Hyperparathyroidism can be differentiated when it causes subperiosteal resorption or cystic bone lesions (rarely). Osteomalacia may cause abnormalities on imaging tests similar to those of osteoporosis.
Other testing
An evaluation for secondary causes of bone loss should be considered in a patient with a Z-score ≤ -2.0. Laboratory testing should usually include the following:
Serum calcium, magnesium, and phosphorus
25-Hydroxy vitamin D level
Liver tests, including testing for a low alkaline phosphatase (hypophosphatasia)
Intact PTH level (hyperparathyroidism)
Serum testosterone in men (hypogonadism)
24-hour urine for calcium and creatinine (hypercalciuria)
Other tests such as thyroid-stimulating hormone or free thyroxine to evaluate for hyperthyroidism, measurements of 24-hour urinary free cortisol to evaluate for Cushing syndrome, and blood counts and other tests to exclude cancer, especially myeloma (eg, serum protein electrophoresis, serum free light chains, urine protein electrophoresis), should be considered depending on the clinical presentation.
Patients with weight loss should be screened for gastrointestinal disorders (eg, malabsorption, celiac disease, inflammatory bowel disease) as well as cancer. Bone biopsy is reserved for unusual cases (eg, young patients with fragility fractures and no apparent cause, patients with chronic kidney disease who may have other bone disorders, patients with persistently very low vitamin D levels suspected of having osteomalacia).
Levels of fasting serum C-telopeptide cross-links (CTX) or urine N-telopeptide cross-links (NTX) reflect increased bone resorption. However, the reliability of the assays vary, which complicates their utility for routine clinical care. These tests should be performed as fasting labs obtained first thing in the morning. Studies suggest that elevated levels of CTX and NTX may be helpful in predicting fracture risk in an untreated patient. These bone turnover markers may help with monitoring response to antiresorptive therapy, and determine the timing and duration of a drug holiday (8). In patients on antiresorptive therapy, levels should be markedly suppressed. If not, abnormal absorption or poor adherence to treatment regimen should be suspected.
Diagnosis references
1. US Preventive Services Task Force, Nicholson WK, Silverstein M, et al. Screening for Osteoporosis to Prevent Fractures: US Preventive Services Task Force Recommendation Statement. JAMA 333(6):498-508, 2025. doi:10.1001/jama.2024.27154
2. Kanis JA, McCloskey EV, Johansson H, et al. A reference standard for the description of osteoporosis. Bone 42(3):467-475, 2008. doi:10.1016/j.bone.2007.11.001
3. Kahwati LC, Kistler CE, Booth G, et al. Screening for Osteoporosis to Prevent Fractures: A Systematic Evidence Review for the US Preventive Services Task Force. JAMA. 333(6):509-531, 2025. doi:10.1001/jama.2024.21653
4. Expert Panel on Musculoskeletal Imaging, Yu JS, Krishna NG, et al. ACR Appropriateness Criteria® Osteoporosis and Bone Mineral Density: 2022 Update. J Am Coll Radiol. 2022;19(11S):S417-S432. doi:10.1016/j.jacr.2022.09.007
5. Siris ES, Adler R, Bilezikian J, et al. The clinical diagnosis of osteoporosis: a position statement from the National Bone Health Alliance Working Group. Osteoporos Int. 25(5):1439-1443, 2014. doi:10.1007/s00198-014-2655-z
6. Alsoof D, Anderson G, McDonald CL, et al. Diagnosis and management of vertebral compression fracture. Am J Med. 135(7):815-821, 2022. doi:10.1016/j.amjmed.2022.02.035
7. Van Staa TP, Leufkens HG, Abenhaim L, et al. Use of oral corticosteroids and risk of fractures. J Bone Miner Res. 15(6):993-1000, 2000. doi:10.1359/jbmr.2000.15.6.993
8. Lorentzon M, Branco J, Brandi ML et al. Algorithm for the use of biochemical markers of bone turnover in the diagnosis, assessment, and follow-up or treatment of osteoporosis. Adv Ther. 36(10): 2811–2824, 2019. doi: 10.1007/s12325-019-01063-9
Treatment of Osteoporosis
Risk factor modification
Calcium and vitamin D adequacy by dietary intake or with use of supplementsCalcium and vitamin D adequacy by dietary intake or with use of supplements
Antiresorptive medications (eg, bisphosphonates, hormone replacement therapy, a selective estrogen receptor modulator, receptor activator of nuclear factor kappa-B ligand [RANKL] inhibitor [denosumab])receptor modulator, receptor activator of nuclear factor kappa-B ligand [RANKL] inhibitor [denosumab])
Anabolic agents (eg, parathyroid hormone (PTH) analogues such as teriparatide and abaloparatide)Anabolic agents (eg, parathyroid hormone (PTH) analogues such as teriparatide and abaloparatide)
Romosozumab, a monoclonal antibody against sclerostin with both antiresorptive and anabolic effectsRomosozumab, a monoclonal antibody against sclerostin with both antiresorptive and anabolic effects
The goals of treatment of osteoporosis are to preserve bone mass, prevent fractures, decrease pain, and maintain function.
The rate of bone loss can be slowed with pharmacotherapy, but adequate calcium and vitamin D ingestion and physical activity are critical to maintaining optimal bone mineral density. Modifiable risk factors should also be addressed.The rate of bone loss can be slowed with pharmacotherapy, but adequate calcium and vitamin D ingestion and physical activity are critical to maintaining optimal bone mineral density. Modifiable risk factors should also be addressed.
Risk factor modification
Risk factor modifications aim to reduce risk of osteoporosis and risk of fractures. Measures include:
Weight-bearing exercise
Moderation of alcohol intake
Fall prevention measures
Weight-bearing exercise can help increase bone mineral density (1). The optimal amount of weight-bearing exercise is not established, but an average of 30 minutes a day is recommended (2). However, excessive exercise without adequate dietary caloric intake in premenopausal women may lead to weight loss and amenorrhea, and subsequent bone loss. If alcohol is consumed, intake should be no more than 1 drink a day for women and 2 drinks a day for men.
Clinicians should routinely ask about recent falls and otherwise assess fall risk. Many older patients are at risk of falls because of poor coordination and balance, poor vision, muscle weakness, confusion, and use of medications that cause postural hypotension or alter the sensorium. Physical therapists can evaluate a patient's gait and fall risk and help create safe individualized programs of core-strengthening exercises to help increase stability and decrease risk of falls. Educating patients about the risks of falls and fractures, instructing how to safely perform daily activities, and modifying the home environment for safety also are important for preventing fractures.
Calcium and vitamin D
All men and women should consume at least 1000 mg of elemental calcium daily. An intake of 1200 mg a day (including dietary consumption) is recommended for postmenopausal women and older men and for periods of increased requirements, such as pubertal growth, pregnancy, and lactation. Calcium intake should ideally be from dietary sources, with the addition of supplements if dietary intake is insufficient. Calcium supplements are taken most commonly as calcium carbonate or calcium citrate. Calcium citrate is better absorbed in patients with achlorhydria, but both are well absorbed when taken with meals. Patients taking gastric acid suppressants (eg, proton pump inhibitors, H2 blockers) or those who have had All men and women should consume at least 1000 mg of elemental calcium daily. An intake of 1200 mg a day (including dietary consumption) is recommended for postmenopausal women and older men and for periods of increased requirements, such as pubertal growth, pregnancy, and lactation. Calcium intake should ideally be from dietary sources, with the addition of supplements if dietary intake is insufficient. Calcium supplements are taken most commonly as calcium carbonate or calcium citrate. Calcium citrate is better absorbed in patients with achlorhydria, but both are well absorbed when taken with meals. Patients taking gastric acid suppressants (eg, proton pump inhibitors, H2 blockers) or those who have hadgastric bypass surgery should take calcium citrate to maximize absorption. Calcium should be taken in divided doses, usually 500 to 600 mg 2 times a day.should take calcium citrate to maximize absorption. Calcium should be taken in divided doses, usually 500 to 600 mg 2 times a day.
Vitamin D supplementation with 600 to 800 international units a day is recommended. Patients with vitamin D deficiency may need even higher doses. Supplemental vitamin D is usually given as cholecalciferol, the natural form of deficiency may need even higher doses. Supplemental vitamin D is usually given as cholecalciferol, the natural form ofvitamin D, although ergocalciferol, the synthetic plant-derived form, is also acceptable. The 25-hydroxy vitamin D level should be ≥ 30 ng/mL.
Antiresorptive medications
Bisphosphonates are first-line therapy (3, 4, 5, 6). By inhibiting bone resorption, bisphosphonates preserve bone mass and can decrease vertebral and hip fractures by up to 50% (7). Bone turnover is reduced after 3 months of bisphosphonate therapy and fracture risk reduction is evident as early as 1 year after beginning therapy. Bisphosphonates can be given orally or IV.
Evidence supports a treatment duration with oral bisphosphonates (eg, alendronate or risedronate) for 5 years or with IV zoledronic acid for 3 years; however, a longer treatment duration may be warranted in some patients at particularly high fracture risk (Evidence supports a treatment duration with oral bisphosphonates (eg, alendronate or risedronate) for 5 years or with IV zoledronic acid for 3 years; however, a longer treatment duration may be warranted in some patients at particularly high fracture risk (8).
Oral bisphosphonates must be taken on an empty stomach with a full (8-oz, 250 mL) glass of water. After administration, the patient must remain upright for at least 30 minutes (60 minutes for ibandronate) and not take anything else by mouth during this time period, because food decreases bioavailability. These medications are safe to use in patients with a creatinine clearance > 35 mL/minute. Oral bisphosphonates can cause esophageal irritation. Esophageal disorders that delay transit time and symptoms of upper gastrointestinal disorders are relative contraindications to oral bisphosphonates. IV bisphosphonates are indicated if a patient is unable to tolerate or is nonadherent with oral bisphosphonates. Oral bisphosphonates must be taken on an empty stomach with a full (8-oz, 250 mL) glass of water. After administration, the patient must remain upright for at least 30 minutes (60 minutes for ibandronate) and not take anything else by mouth during this time period, because food decreases bioavailability. These medications are safe to use in patients with a creatinine clearance > 35 mL/minute. Oral bisphosphonates can cause esophageal irritation. Esophageal disorders that delay transit time and symptoms of upper gastrointestinal disorders are relative contraindications to oral bisphosphonates. IV bisphosphonates are indicated if a patient is unable to tolerate or is nonadherent with oral bisphosphonates.
Osteonecrosis of the jaw (ONJ) and atypical femoral fractures have been rarely reported in patients receiving antiresorptive therapy with bisphosphonates, and also with use of romosozumab, or (ONJ) and atypical femoral fractures have been rarely reported in patients receiving antiresorptive therapy with bisphosphonates, and also with use of romosozumab, ordenosumab (9). Risk factors for ONJ include invasive dental procedures, IV bisphosphonate use, and radiation to the head and neck to treat cancer. The benefits of reduction of osteoporosis-related fractures far outweigh this small risk. Although some dentists ask a patient to discontinue a bisphosphonate for several weeks or months before an invasive dental procedure, it is not clear that doing so decreases the risk of osteonecrosis of the jaw.
Long-term bisphosphonate use may increase the risk of atypical femoral fractures (10). These fractures occur in the mid-shaft of the femur with minimal or no trauma and may be preceded by weeks or months of thigh pain. The fractures may be bilateral even if symptoms are only unilateral.
To minimize atypical fracture incidence, consideration should be given to stopping bisphosphonates after approximately:
3 to 5 years of use in patients with osteoporosis (by DXA scan) but few or no other risk factors for bone loss (3 years for IV zoledronic acid and 5 years for oral bisphosphonates)(3 years for IV zoledronic acid and 5 years for oral bisphosphonates)
5 to 10 years of use in patients with osteoporosis (by DXA scan) and fractures or additional significant ongoing risk factors for bone loss and future osteoporotic fractures (11, 12)
Intermittent cessation of bisphosphonate treatment (drug holiday), as well as initiation and duration of therapy, depend on patient risk factors such as age, comorbidities, prior fracture history, DXA scan results, and fall risk. The drug holiday is 1 year or longer. Patients on a bisphosphonate holiday should be closely monitored for a new fracture or accelerated bone loss evident on a DXA scan, especially after being off therapy for 2 years or more.
During therapy with an antiresorptive medication such as a bisphosphonate, bone turnover is suppressed, as evidenced by low serum or urinary levels of (fasting) N-telopeptide cross-links (NTX) or C-telopeptide cross-links (CTX). Thus, measures of bone turnover markers can help determine adherence to therapy, as well as sufficient absorption, which are particularly useful for monitoring in patients taking oral bisphosphonates. These markers may remain low for ≥ 2 years off therapy. In untreated patients, an increase in levels of bone turnover markers, particularly with higher levels, indicates an increased risk of fracture. However, it is not clear whether levels of bone turnover markers should be used as criteria for when to start or end a drug holiday.
The immediate initiation of a bisphosphonate after an osteoporotic fracture has been controversial because of a theoretical concern that these agents may impede bone healing; although this has not been borne out in the clinical literature. Most experts recommend starting a bisphosphonate during the hospitalization for the fracture (13). There is no reason to delay therapy in order to obtain a DXA scan because a hip or vertebral fragility fracture establishes the presence of osteoporosis.
DenosumabDenosumab is a monoclonal antibody against the receptor activator of nuclear factor kappa-B ligand (RANKL) and reduces bone resorption by inhibiting osteoclast differentiation and formation (14). Denosumab may be helpful in patients intolerant of or unresponsive to other therapies or in patients with impaired renal function. This medication has been found to have a good safety profile at 10 years of therapy (15). Denosumab is contraindicated in patients with hypocalcemia because it can cause calcium shifts that result in profound hypocalcemia and adverse effects such as tetany. Osteonecrosis of the jaw and atypical femoral fractures have been rarely reported in patients taking denosumab.
Patients taking denosumab should not undergo a drug holiday because discontinuation may cause a rapid loss in bone mineral density and, importantly, increase the risk of fractures, particularly vertebral fractures, often multiple (16). If and when denosumab is discontinued, patients should be transitioned to a bisphosphonate such as IV zoledronic acid for at least a year, longer if there is ongoing risk of fracture or evidence of loss of bone mineral density after only a single IV zoledronic acid infusion (is discontinued, patients should be transitioned to a bisphosphonate such as IV zoledronic acid for at least a year, longer if there is ongoing risk of fracture or evidence of loss of bone mineral density after only a single IV zoledronic acid infusion (17).
RaloxifeneRaloxifene is a selective estrogen receptor modulator (SERM) that may be appropriate for treatment of osteoporosis in women who cannot take bisphosphonates or denosumab. It is given orally once daily and reduces vertebral fractures by approximately 50% but has not been shown to reduce hip fractures () that may be appropriate for treatment of osteoporosis in women who cannot take bisphosphonates or denosumab. It is given orally once daily and reduces vertebral fractures by approximately 50% but has not been shown to reduce hip fractures (18). Raloxifene does not stimulate the uterus and antagonizes estrogen effects in the breast. It reduces the risk of invasive breast cancer. Raloxifene may increase risk of thromboembolism.
Estrogen therapy preserves bone mineral density and decreases the risk of fractures (19). However, because of the availability of other more effective treatments and the potential risks associated with continued therapy, estrogen is not typically used as first-line therapy for the sole indication of treating osteoporosis. The use of estrogen increases the risk of thromboembolism and endometrial cancer and is also associated with additional risks (eg, breast cancer, endometrial cancer, coronary artery disease, stroke, and gallbladder disease), some of which vary depending on the use of estrogen-alone versus estrogen combined with a progestin (20, 21). Thus, the potential harms of estrogen treatment for osteoporosis outweigh its potential benefits for most women.
Intranasal salmon calcitoninIntranasal salmon calcitonin should not regularly be used for treating osteoporosis. Salmon calcitonin may provide short-term analgesia after an acute fracture, such as a painful vertebral fracture, due to an endorphin effect (should not regularly be used for treating osteoporosis. Salmon calcitonin may provide short-term analgesia after an acute fracture, such as a painful vertebral fracture, due to an endorphin effect (22). It has not been shown to reduce future fractures.
Anabolic agents
Anabolic agents include teriparatide (synthetic PTH [PTH1-34]) (Anabolic agents include teriparatide (synthetic PTH [PTH1-34]) (23) and abaloparatide (a human PTH analog that binds to PTH type 1 receptor) () and abaloparatide (a human PTH analog that binds to PTH type 1 receptor) (24). They are given daily by subcutaneous injection and increase bone mass, stimulate new bone formation, and reduce the risk of fractures. Patients taking a PTH analog should have a creatinine clearance > 35 mL/minute. Romosozumab, the monoclonal antibody against sclerostin, has both anabolic and antiresorptive effects.). They are given daily by subcutaneous injection and increase bone mass, stimulate new bone formation, and reduce the risk of fractures. Patients taking a PTH analog should have a creatinine clearance > 35 mL/minute. Romosozumab, the monoclonal antibody against sclerostin, has both anabolic and antiresorptive effects.
These three anabolic agents (teriparatide, abaloparatide, and romosozumab) are generally indicated for patients who have the following characteristics:These three anabolic agents (teriparatide, abaloparatide, and romosozumab) are generally indicated for patients who have the following characteristics:
Cannot tolerate antiresorptive medications or have contraindications to their use
Fail to respond (ie, develop new fractures or lose bone mineral density) to antiresorptive medication, as well as calcium, vitamin D, and weight bearing exerciseFail to respond (ie, develop new fractures or lose bone mineral density) to antiresorptive medication, as well as calcium, vitamin D, and weight bearing exercise
Possibly have severe osteoporosis (eg, T-score < -3.0) or multiple vertebral fragility fractures
Have glucocorticoid-induced osteoporosis (teriparatide only)Have glucocorticoid-induced osteoporosis (teriparatide only)
Any of these three anabolic agents can be considered for use during a bisphosphonate holiday.
The use of anabolic agents to treat osteoporosis had been limited to 2 years based on a boxed warning because of concern of increased risk of developing osteosarcoma in initial 2-year clinical trials, but the restriction of 2 years of therapy is no longer required. Consequently, although 2 years of treatment with an anabolic agent remains a reasonable course of therapy, giving a second 2-year course of therapy can now be considered. However, after completion of a treatment course with an anabolic agent, the bone mineral density gains are quickly lost if a patient is not promptly transitioned to an antiresorptive agent such as a bisphosphonate. Anabolic agents should ideally be used before antiresorptive agents (25). Gains in bone mineral density are greater if an anabolic agent is used prior to an antiresorptive agent (ie, considering an "anabolic window"), and bone mineral density gains are attenuated if an anabolic agent is administered following an antiresorptive medication.
Anabolic agents are safe to initiate at any time after a fracture. It is not clear whether early post-fracture use of anabolic agents accelerates bone healing.
Other medications for osteoporosis
RomosozumabRomosozumab is a monoclonal antibody against sclerostin (a small protein made by osteocytes that inhibits new bone formation by osteoblasts). It has both antiresorptive and anabolic effects and has been shown to increase bone mineral density in the hip and lumbar spine and reduce fracture risk in postmenopausal women (26). Romosozumab is indicated for patients with severe osteoporosis, particularly in older adults, those who are frail, and those with an increased risk of falling. It should also be considered in patients who fracture despite adequate antiresorptive therapy. It is given via monthly subcutaneous injection for 1 year (27).
Romosozumab treatment for 1 year followed by alendronate for 1 year is more efficacious than treatment with treatment for 1 year followed by alendronate for 1 year is more efficacious than treatment withalendronate for 2 years (28), and romosozumab for 1 year followed by denosumab for 2 years decreases fracture risk and increases bone mineral density (for 1 year followed by denosumab for 2 years decreases fracture risk and increases bone mineral density (28). As with denosumab, when romosozumab is discontinued, antiresorptive therapy should be given to prevent rapid bone loss (29). Romosozumab carries a boxed warning due to increased risk for cardiovascular events, including myocardial infarction, stroke, and cardiovascular death. Romosozumab should not be initiated within 12 months of a patient having had a myocardial infarction or stroke.
Monitoring response to treatment
Monitoring for ongoing bone loss or the response to treatment with serial DXA scans should be performed using the same DXA machine, and the comparison should use actual bone mineral density (g/cm2) rather than T-score. In patients with osteopenia, DXA should be repeated periodically to determine whether there is ongoing bone loss or development of frank osteoporosis requiring treatment. The frequency for follow-up DXA scanning varies from patient to patient, but some reasonable guidelines are as follows:
Patients being treated with oral bisphosphonates: Repeat DXA scan usually after 2 to 3 years of therapy. DXA scan may be repeated more frequently if clinically warranted, for example in a patient taking glucocorticoids.
Patients treated with IV bisphosphonates: Repeat DXA scan for monitoring after 3 years of therapy to help determine if treatment has been adequate or a longer therapy course is warranted.
Patients treated with anabolic therapy: Repeat DXA scan upon completion of therapy (18 to 24 months of teriparatide or abaloparatide, 1 year of romosozumab) to document improvement in bone mineral density with anabolic therapy and to establish a new baseline.Patients treated with anabolic therapy: Repeat DXA scan upon completion of therapy (18 to 24 months of teriparatide or abaloparatide, 1 year of romosozumab) to document improvement in bone mineral density with anabolic therapy and to establish a new baseline.
Results may help identify patients at higher risk of fractures due to a suboptimal response to osteoporosis treatment. Patients who have a significantly lower bone mineral density despite treatment, or those who sustain a fracture while on treatment, should be evaluated for secondary causes of bone loss, poor medication absorption (if taking an oral bisphosphonate), and (except for patients treated with IV bisphosphonates or parenteral medications given in the office) medication adherence.
Treating pain and maintaining function
Acute back pain resulting from a vertebral compression fracture can be treated with short-term orthopedic bracing as needed, analgesics, and, when muscle spasm is prominent, moist heat and massage. Core-strengthening exercises are helpful for patients who have back pain and a prior healed vertebral fracture. Chronic backache may be relieved by exercises to strengthen paravertebral muscles. Avoiding heavy lifting can help. Bed rest should be minimized, and consistent, carefully designed weight-bearing exercise should be encouraged.
In some patients, vertebroplasty or kyphoplasty can be used to relieve severe pain due to a new vertebral fragility fracture; however, the evidence for efficacy is inconclusive (30, 31). In vertebroplasty, methyl methacrylate is injected into the vertebral body. In kyphoplasty, the vertebral body is first expanded with a balloon then injected with methyl methacrylate. These procedures may reduce deformity in the injected vertebrae but do not reduce and may even increase the risk of fractures in adjacent vertebrae. Other adverse effects include rib fractures, cement leakage, pulmonary embolism, and myocardial infarction. Further study to determine indications for these procedures is warranted.
Treatment references
1. Howe TE, Shea B, Dawson LJ, et al. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst Rev. (7):CD000333, 2011. Published 2011 Jul 6. doi:10.1002/14651858.CD000333.pub2
2. Brooke-Wavell K, Skelton DA, Barker KL, et al. Strong, steady and straight: UK consensus statement on physical activity and exercise for osteoporosis [published online ahead of print, 2022 May 16]. Br J Sports Med. 56(15):837-846, 2022. doi:10.1136/bjsports-2021-104634
3. Management of osteoporosis in postmenopausal women: the 2021 position statement of The North American Menopause Society. Menopause. 2021;28(9):973-997. doi:10.1097/GME.0000000000001831
4. Shoback D, Rosen CJ, Black DM, et al. Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Guideline Update. J Clin Endocrinol Metab. 2020;105(3):dgaa048. doi:10.1210/clinem/dgaa048
5. ACOG Committee on Clinical Practice Guidelines–Gynecology. Management of Postmenopausal Osteoporosis: ACOG Clinical Practice Guideline No. 2 [published correction appears in Obstet Gynecol. 2022 Jul 01;140(1):138. doi: 10.1097/AOG.0000000000004855.]. Obstet Gynecol. 2022;139(4):698-717. doi:10.1097/AOG.0000000000004730
6. Camacho PM, Petak SM, Binkley N, et al. AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS/AMERICAN COLLEGE OF ENDOCRINOLOGY CLINICAL PRACTICE GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF POSTMENOPAUSAL OSTEOPOROSIS-2020 UPDATE. Endocr Pract. 2020;26(Suppl 1):1-46. doi:10.4158/GL-2020-0524SUPPL
7. Ayers C, Kansagara D, Lazur B, Fu R, Kwon A, Harrod C. Effectiveness and safety of treatments to prevent fractures in people with low bone mass or primary osteoporosis: a living systematic review and network meta-analysis for the American College of Physicians [published correction appears in Ann Intern Med 176(6):884, 2023]. Ann Intern Med. 176(2):182-195, 2023. doi:10.7326/M22-0684
8. Black DM, Reid IR, Boonen S, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: A randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res. 27(2): 243–254, 2012. doi: 10.1002/jbmr.1494
9. Khan AA, Morrison A, Hanley DA, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res. 30(1):3-23, 2015. doi:10.1002/jbmr.2405
10. Black DM, Abrahamsen B, Bouxsein ML, et al. Atypical Femur Fractures: Review of Epidemiology, Relationship to Bisphosphonates, Prevention, and Clinical Management. Endocr Rev. 40(2):333-368, 2019. doi:10.1210/er.2018-00001
11. Black DM, Schwartz AV, Ensrud KE, et al. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. . Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial.JAMA. 296(24):2927-2938, 2006. doi:10.1001/jama.296.24.2927
12. Black DM, Reid IR, Boonen S, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT) [published correction appears in . The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT) [published correction appears inJ Bone Miner Res. 27(12):2612, 2012]. J Bone Miner Res 27(2):243-254, 2012. doi:10.1002/jbmr.1494
13. Conley RB, Adib G, Adler RA, et al. Secondary Fracture Prevention: Consensus Clinical Recommendations from a Multistakeholder Coalition. J Bone Miner Res. 35(1):36-52, 2020. doi:10.1002/jbmr.3877
14. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis [published correction appears in N Engl J Med 361(19):1914, 2009]. N Engl J Med. 361(8):756-765, 2009. doi:10.1056/NEJMoa0809493
15. Bone HG, Wagman RB, Brandi ML, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol. 5(7):513-523, 2017. doi:10.1016/S2213-8587(17)30138-9
16. Lyu H, Yoshida K, Zhao SS, et al. Delayed Denosumab Injections and Fracture Risk Among Patients With Osteoporosis : A Population-Based Cohort Study. Ann Intern Med. 173(7):516-526, 2020. doi:10.7326/M20-0882
17. Sølling AS, Harsløf T, Langdahl B. Treatment with zoledronate subsequent to denosumab in osteoporosis: a 2-year randomized study. J Bone Miner Res. 36(7):1245-1254, 2021. doi:10.1002/jbmr.4305
18. Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators [published correction appears in JAMA. 282(22):2124, 1999]. JAMA 282(7):637-645, 1999. doi:10.1001/jama.282.7.637
19. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA. 2002;288(3):321-333. doi:10.1001/jama.288.3.321
20. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701-1712. doi:10.1001/jama.291.14.1701
21. Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women's Health Initiative randomized trials. JAMA. 2013;310(13):1353-1368. doi:10.1001/jama.2013.278040
22. Knopp-Sihota JA, Newburn-Cook CV, Homik J, et al. Calcitonin for treating acute and chronic pain of recent and remote osteoporotic vertebral compression fractures: a systematic review and meta-analysis. Osteoporos Int. 23(1):17-38, 2012. doi:10.1007/s00198-011-1676-0
23. Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. . Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis.N Engl J Med. 344(19):1434-1441, 2001. doi:10.1056/NEJM200105103441904
24. Miller PD, Hattersley G, Riis BJ, et al. Effect of abaloparatide vs placebo on new Vertebral fractures in postmenopausal women with osteoporosis: a randomized clinical trial [published correction appears in JAMA. 2017 Jan 24;317(4):442]. JAMA. 316(7):722-733, 2016. doi:10.1001/jama.2016.11136
25. Curtis EM, Reginster JY, Al-Daghri N, et al. Management of patients at very high risk of osteoporotic fractures through sequential treatments. Aging Clin Exp Res. 34(4):695-714, 2022. doi:10.1007/s40520-022-02100-4
26. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med. 375(16):1532-1543, 2016. doi: 10.1056/NEJMoa1607948
27. Saag KG, Petersen J, Brandi ML, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med. 377(15):1417-1427, 2017. doi: 10.1056/NEJMoa1708322
28. Lewiecki EM, Dinavahi RV, Lazaretti-Castro M, et al. One year of romosozumab followed by two years of denosumab maintains fracture risk reductions: Results of the FRAME Extension Study. J Bone Miner Res. 34(3):419-428, 2019. doi: 10.1002/jbmr.3622
29. McClung MR, Brown JP, Diez-Perez A, et al. Effects of 24 Months of Treatment With Romosozumab Followed by 12 Months of Denosumab or Placebo in Postmenopausal Women With Low Bone Mineral Density: A Randomized, Double-Blind, Phase 2, Parallel Group Study. J Bone Miner Res. 33(8):1397-1406, 2018. doi:10.1002/jbmr.3452
30. Buchbinder R, Johnston RV, Rischin KJ, et al. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database Syst Rev. 4(4):CD006349, 2018. Published 2018 Apr 4. doi:10.1002/14651858.CD006349.pub3
31. Lou S, Shi X, Zhang X, Lyu H, Li Z, Wang Y. Percutaneous vertebroplasty versus non-operative treatment for osteoporotic vertebral compression fractures: a meta-analysis of randomized controlled trials. Osteoporos Int. 30(12):2369-2380, 2019. doi:10.1007/s00198-019-05101-8
Prevention of Osteoporosis
The goals of prevention are 2-fold: preserve bone mass and prevent fractures. Preventive measures are indicated for the following:
Postmenopausal women
Older men (typically men > 70 years old)
Patients who have osteopenia
Patients who already have osteoporosis (to prevent worsening)
Patients taking high-dose and/or long-term systemic glucocorticoids or aromatase inhibitors
Patients with secondary causes for bone loss
Preventive measures for all of these patients include appropriate calcium and vitamin D intake, weight-bearing exercise, tobacco avoidance, and limiting alcohol ingestion. Patients should also be counseled on measures to reduce the risk of falls. In addition, pharmacologic therapy is indicated for most patients who have osteopenia if they are at increased risk of fracture, such as those with a high FRAX score, and patients taking corticosteroids or aromatase inhibitors. Educating patients and the community about the importance of bone health remains of utmost importance.Preventive measures for all of these patients include appropriate calcium and vitamin D intake, weight-bearing exercise, tobacco avoidance, and limiting alcohol ingestion. Patients should also be counseled on measures to reduce the risk of falls. In addition, pharmacologic therapy is indicated for most patients who have osteopenia if they are at increased risk of fracture, such as those with a high FRAX score, and patients taking corticosteroids or aromatase inhibitors. Educating patients and the community about the importance of bone health remains of utmost importance.
Key Points
Peak bone mass in men and women occurs around age 30; in women, bone loss accelerates after menopause to approximately 2% a year for approximately 10 years.
Nearly all cases of osteoporosis in men and women are primary, without an identifiable cause.
Suspect osteoporosis in patients who have fractures caused by unexpectedly little force (fragility fractures) of the spine, hip, humerus, or distal radius.
Use DXA to measure bone mineral density in women ≥ 65 years; women between menopause and age 65 who have risk factors (eg, family history of osteoporosis, a low body mass index, and use of tobacco, alcohol, and/or medications with a high risk of bone loss [eg, chronic glucocorticoid use]); men and women of any age who have fragility fractures; evidence on imaging studies of decreased bone mineral density or asymptomatic vertebral compression fractures; and patients at risk of secondary osteoporosis.
Consider testing patients for causes of secondary bone loss if they have a Z-score ≤ -2.0, a decline in bone mineral density, an unexplained fracture while on treatment for osteoporosis, or a cause of secondary bone loss is clinically suspected.
For treatment and prevention, ensure adequate intake of calcium and vitamin D, using supplements when necessary, and modify risk factors to help preserve bone mass (eg, with weight-bearing exercise and by minimizing use of alcohol and tobacco) and reduce fall risk.For treatment and prevention, ensure adequate intake of calcium and vitamin D, using supplements when necessary, and modify risk factors to help preserve bone mass (eg, with weight-bearing exercise and by minimizing use of alcohol and tobacco) and reduce fall risk.
Medications include antiresorptives (eg, bisphosphonates, a receptor activator of nuclear factor kappa-B ligand [RANKL] inhibitor, a selective estrogen receptor modulator, medications used for hormone replacement therapy) or anabolic agents such as teriparatide, abaloparatide, or romosozumab.receptor modulator, medications used for hormone replacement therapy) or anabolic agents such as teriparatide, abaloparatide, or romosozumab.
Monitor response to treatment with DXA at appropriate intervals depending upon the specific medication regimen used.


