



Metabolic and bariatric surgery is the surgical alteration of the stomach, intestine, or both to cause weight loss in patients with obesity-related metabolic disorders and their sequellae.

")


In the United States, about 260,000 bariatric operations are done in each year (1). Development of safer, minimally invasive approaches has made this surgery more prevalent.
(See also Obesity.)
Reference
1. Clapp B, Ponce J, DeMaria, et al: American Society for Metabolic and Bariatric Surgery 2020 estimate of metabolic and bariatric procedures performed in the United State. Aurg Obes Relat Dis 18 (9):1134–1140, 2022. doi: 10.1016/j.soard.2022.06.284 Epub 2022 Jun 26.
Indications for Bariatric Surgery
In 2022, the American Society for Metabolic and Bariatric Surgery (ASMBS) and the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) updated recommendations for metabolic and bariatric surgery to include patients with a BMI > 35 kg/m2 regardless of comorbidities and those with a BMI 30 to 34.5 kg/m2 with metabolic disorders. Comorbidities include the following:
Cardiovascular disorders
Metabolic dysfunction-associated steatotic liver disease and steatohepatitis
Pseudotumor cerebri
Bone and joint disorders
The updated recommendations also specify that BMI thresholds should be adjusted in Asian populations and that patients with a BMI ≥ 27.5 kg/m2 should be offered surgery (1).
Metabolic and bariatric surgery is offered as part of a weight-loss program that usually includes
Provider seminar classes
Psychological assessment of the patient
Consultation with a surgeon
Consultation with registered dietitians
Routine laboratory tests
Screening for obstructive sleep apnea (OSA)
Operative risk stratification
Contraindications include
An uncontrolled psychiatric disorder such as major depression
Current substance or alcohol use disorder
Cancer that is not in remission
Another life-threatening disorder
Inability to comply with nutritional requirements, including life-long vitamin replacement (when indicated)

Indications reference
1. Eisenberg D, Shikora SA, Aarts E, et al: 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for metabolic and bariatric surgery. Surg Obes Relat Dis 18 (12):1345-1356, 2022. doi: 10.1016/j.soard.2022.08.013 Epub 2022 Oct 21.
Procedures for Bariatric Surgery
The most common metabolic and bariatric procedures performed in the United States include
Procedures such as the vertical banded gastroplasty or adjustable gastric banding are rarely used. Bariatric surgeons should be familiar with historical procedures because surgical complications can develop at any time—months to years—after surgery (1).
Despite a growing percentage of the population with obesity, metabolic and bariatric surgery remains underused. Fewer than 1% of patients who qualify for surgery have the procedure. Telemedicine has allowed greater access to preoperative consultation; nonetheless, overall rates remain low (2).
Usually, minimally invasive techniques—either laparoscopically or robotically—are used, resulting in less pain and a shorter healing time than after open surgery. Traditionally, bariatric surgery has been classified as restrictive and/or malabsorptive, referring to the presumptive mechanism of weight loss. However, other factors appear to contribute to weight loss; for example, both RYGB (traditionally classified as malabsorptive) and sleeve gastrectomy (traditionally classified as restrictive) result in metabolic or hormonal changes that favor satiety and weight loss and in other hormonal changes (eg, an increase in insulin release [incretin effect]) that appear to contribute to the rapid remission of diabetes.
After RYGB (particularly) or sleeve gastrectomy, levels of gastrointestinal hormones, such as glucagon-like peptide-1 (GLP-1) and peptide YY (PYY), are increased, possibly contributing to satiety, weight loss, and remission of diabetes. Increased insulin sensitivity is evident immediately postoperatively, before significant weight loss occurs, suggesting that neurohormonal factors are prominent in remission of diabetes. A change in gut microbiome may also contribute to changes in weight after RYGB. Metabolic and bariatric surgery reduces risk of mortality caused by cardiovascular disorders, diabetes, and cancer.
Sleeve gastrectomy
Sleeve gastrectomy is the most commonly used metabolic and bariatric surgical procedure in the United States. About 80% of the stomach is removed, creating a tubular stomach passage that resembles a banana. The resulting sleeve holds less food and thus reduces the number of calories consumed. Patients also experience less hunger, which correlates with decreased levels of ghrelin and other neurohormonal alterations. The procedures is technically simpler than bypass procedures and can be done as the first step toward a biliopancreatic diversion with duodenal switch (BPD-DS) or single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). Sleeve gastrectomy does not alter the small intestine.
Rare but serious complications include sleeve leakage and bleeding. Patients may also experience worsening or new-onset gastroesophageal reflux disease (GERD).
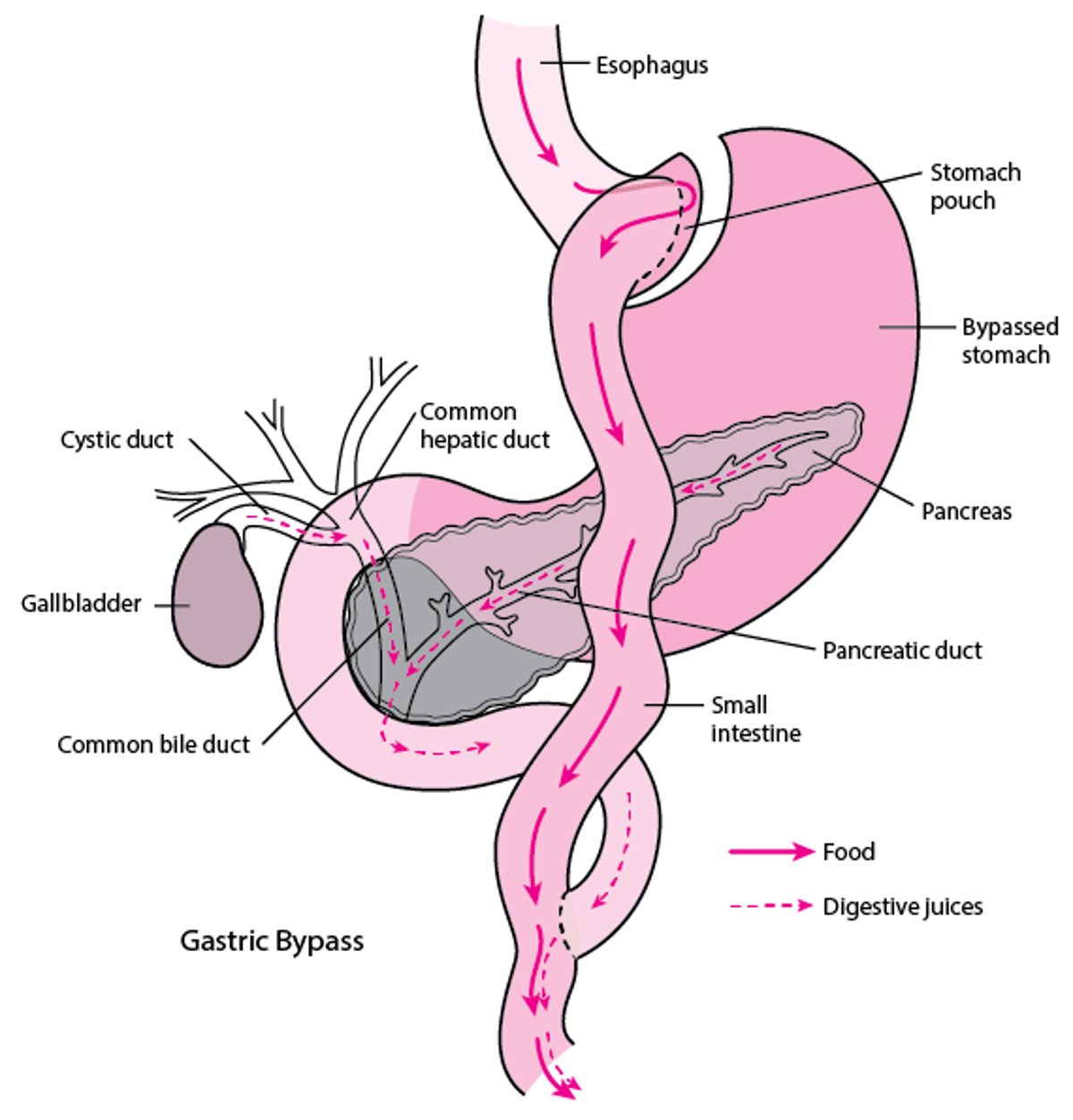
Roux-en-Y gastric bypass (RYGB) surgery
RYGB is considered a restrictive and malabsorptive procedure. A small part of the proximal stomach is detached from the rest, creating a stomach pouch of < 30 mL. Food bypasses part of the remaining stomach and proximal small intestine, where it is normally absorbed, reducing the amount of food and calories absorbed. The pouch is connected to the proximal jejunum; the opening between them is narrow, limiting the rate of gastric emptying. The segment of small intestine connected to the bypassed stomach is attached to the distal small intestine. This arrangement allows bile acids and pancreatic enzymes to mix with gastrointestinal contents, limiting malabsorption and nutritional deficiencies.
RYGB is particularly effective in treating diabetes; remission rates are up to 62% after 6 years (3). RYGB has also been shown to reduce the risk of obesity-related diseases including cardiovascular disease, diabetes, and cancer, as well as overall mortality and mortality related to these diseases (4, 5).
Short-term complications include anastomotic leak (more commonly at the gastrojejunal connection) and bleeding. Dumping syndrome can occur after eating high-fat and high-sugar foods; symptoms can include light-headedness, diaphoresis, nausea, abdominal pain, and diarrhea. Long-term risk of ulceration at the gastrojejunal anastomosis can occur in patients who take nonsteroidal anti-inflammatory drugs (NSAIDs) or smoke cigarettes after RYGB. Bowel obstruction can occur if internal hernia or intussusception develops.
Roux-en-Y Gastric Bypass Surgery

Revisional procedures
An increasing number of patients are having revisional procedures to manage inadequate weight loss, weight regain, or other complications, such as development of GERD after sleeve gastrectomy.
For RYGB, revision may involve shortening the gastric pouch or the duodenal segment that is attached to the stomach. The purpose is reduce absorption of calories and nutrients.
Preoperative evaluation usually includes endoscopy and x-ray studies (eg, barium swallow).
Biliopancreatic diversion with a duodenal switch (BPD-DS)
BPD-DS accounts for < 5% of bariatric procedures done in the United States, but the annual number of procedures is increasing. It is usually reserved for patients with extreme morbid obesity (BMI > 50 kg/m2). BPD-DS can be done as one procedure or staged (first sleeve gastrectomy alone, then biliopancreatic diversion with duodenal switch after initial weight loss). About two-thirds to three-fourths of the upper small intestine is bypassed in the procedure.
After sleeve gastrectomy, the duodenum is divided just distal to the pylorus, and a segment of ileum is brought up and anastomosed to the proximal duodenum, creating an approximately 200-cm alimentary limb that bypasses much of the small intestine and the sphincter of Oddi (where bile acids and pancreatic enzymes enter). As a result, food absorption is decreased. The other cut end of the duodenum is tied off, and a second anastomosis is made between the remainder of the excluded loop and the ileum, creating a 100-cm channel for biliary and pancreatic enzymes to enter the distal small intestine and facilitate digestion.
BPD-DS is technically more difficult than sleeve gastrectomy or RYGB, but it is the most effective procedure for weight loss and resolution of type 2 diabetes. Complication rates are slightly higher than with other procedures, and malabsorption, steatorrhea, and nutritional deficiencies can occur. Patients must take nutritional supplements and be monitored for deficiencies for the rest of their life.
Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S)
Like BPD-DS, SADI-S includes sleeve gastrectomy and division at the first portion of the duodenum. It can be performed in one or two stages. The main difference is that SADI-S features a single loop anastomosis with a longer common channel for absorption. It is a slightly simpler and faster procedure and has less risk of nutritional deficiencies than BPD-DS. But it has a greater potential to worsen or lead to new-onset gastroesophageal reflux symptoms. Bile reflux can also occur because there is no roux limb.
Endoscopic procedures
Newer endoscopic procedures can help treat patients who are not candidates for surgery or who prefer a less invasive, nonsurgical approach.
An intragastric balloon may be used. An uninflated silicone balloon is passed into the stomach, then filled with saline. The balloon decreases gastric volume and promotes satiety. After 6 months, the balloon is removed. Patients lose weight initially, but long-term success is limited.
Endoscopic sleeve gastroplasty reduces the size of the stomach by suturing it from within. Because the sutures bring folds of the stomach together, it has been called the accordion procedure. Overall complication rates are low; the most common complications include nausea, gastrointestinal bleeding, perigastric leakage, and accumulation of fluid.
Sleeve gastroplasty has a lower reflux rate than endoscopic sleeve gastrectomy, and the procedure is potentially reversible. Five-year data suggest sustained weight loss; however, longer-term data are lacking (6).
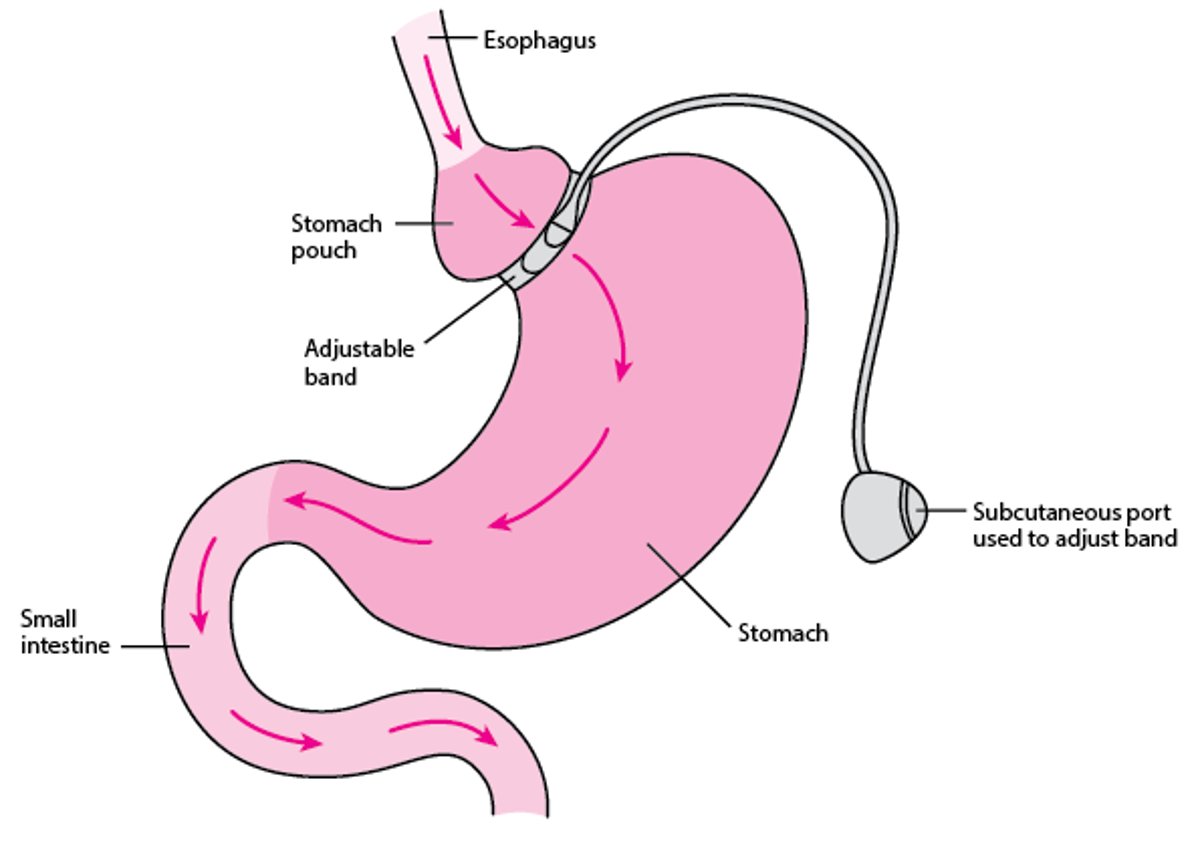
Adjustable gastric banding
Adjustable gastric banding is rarely performed in the United States. More often, patients who have had this procedure have the bands removed and undergo sleeve gastrectomy or RYGB.
For adjustable gastric banding, the band is placed around the upper part of the stomach to divide the stomach into a small upper pouch and a larger lower pouch. Typically, the band is adjusted 4 to 6 times by injecting saline into the band via a port that is placed subcutaneously. When saline is injected, the band expands, restricting the upper pouch of the stomach. As a result, the pouch can hold much less food, patients eat more slowly, and satiety occurs earlier. Saline can be removed from the band if a complication occurs or if the band is overly restrictive.
Weight loss with the band varies and is related to the frequency of follow-up; more frequent follow-ups result in greater weight loss. Early postoperative morbidity and mortality rates are lower than with other procedures. Long-term complications include gastroesophageal reflux, esophagitis, slipped bands, and erosion.
Removing the bands is sometimes technically challenging because scar tissue forms around the band.
Adjustable Gastric Banding

Procedures references
1. Coblijn UK, Karres J, de Raaff CAL, et al: Predicting postoperative complications after bariatric surgery: The Bariatric Surgery Index for Complications, BASIC. Surg Endosc 31 (11):4438–4445, 2017. doi: 10.1007/s00464-017-5494-0 Epub 2017 Mar 31.
2. Hlavin C, Ingraham P, Byrd T, et al: Clinical outcomes and hospital utilization among patients undergoing bariatric surgery with telemedicine preoperative care. JAMA Netw Open 6 (2):e2255994, 2023. doi: 10.1001/jamanetworkopen.2022.55994
3. Adams TD, Davidson LE, Litwin SE, et al: Weight and metabolic outcomes 12 years after gastric bypass. N Engl J Med 377 (12):1143–1155, 2017. doi: 10.1056/NEJMoa1700459
4 Carlsson LMS, Carlsson B, Jacobson P, et al: Life expectancy after bariatric surgery or usual care in patients with or without baseline type 2 diabetes in Swedish obese subjects. Int J Obes (Lond). 47 (10):931–938, 2023. doi: 10.1038/s41366-023-01332-2 Epub 2023 Jul 12.
5. Adams TD, Gress RE, Smith SC, et al: Long-term mortality after gastric bypass surgery. N Engl J Med 357(8):753–761, 2007. doi: 10.1056/NEJMoa066603
6. Yoon JY, Arau RT; Study Group for Endoscopic Bariatric and Metabolic Therapies of the Korean Society of Gastrointestinal Endoscopy.: The efficacy and safety of endoscopic sleeve gastroplasty as an alternative to laparoscopic sleeve gastrectomy. Clin Endosc 54 (1):17–24, 2021. doi: 10.5946/ce.2021.019 Epub 2021 Jan 22.
Preoperative Evaluation for Metabolic and Bariatric Surgery
Preoperative evaluation consists of
Diagnosis and correction of comorbid conditions as much as possible
Assessment of readiness and ability to engage in lifestyle modification
Exclusion of contraindications to surgery
Review of the postoperative diet and assessment of the patient's ability to make dietary changes by a dietitian
Identification of any uncontrolled psychiatric disorder and any dependencies that would preclude surgery and identification and discussion of potential obstacles to adherence to lifestyle changes postoperatively by a psychologist or other qualified mental health care practitioner
Extensive preoperative evaluation is not routinely necessary, but preoperative testing may be necessary based on clinical findings, and measures to control certain conditions (eg, hypertension) or reduce risk may be taken.
Pulmonary: Patients at risk of obstructive sleep apnea based on clinical suspicion should be screened with polysomnography, and if obstructive sleep apnea is present, patients should be treated with continuous positive airway pressure (CPAP). This diagnosis indicates risk of cardiovascular morbidity and premature death. Smoking increases risk of pulmonary complications, ulcers, and gastrointestinal (GI) bleeding postoperatively. Smoking should be stopped at least 6 weeks but preferably 1 year before surgery to minimize perioperative complications and indefinitely thereafter.
Cardiac: Preoperative ECG and other noninvasive cardiac testing is considered if individual risk warrants, even for asymptomatic patients, to identify occult coronary artery disease. Even though obesity increases risk of pulmonary hypertension, echocardiography is not done routinely. Other cardiac testing is not done routinely; rather it is done based on the patient's risk factors for coronary artery disease, risk of surgery, and functional status. Blood pressure should be optimally controlled before surgery. During the perioperative period, risk of acute kidney injury is increased; thus, diuretics, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin II receptor blockers (ARBs), if needed, should be used cautiously during this time. is increased; thus, diuretics, angiotensin-converting enzyme (ACE) inhibitors, and angiotensin II receptor blockers (ARBs), if needed, should be used cautiously during this time.
Gastrointestinal (GI): Preoperative endoscopy or GI imaging studies should be done if patients have clinically significant GI symptoms. To reduce the risk of marginal ulcers, clinicians may test for and treat Helicobacter pylori infection, although evidence for the necessity of such treatment preoperatively is inconsistent.
Hepatic: Increased liver enzymes, especially alanine aminotransferase (ALT), are common among candidates for metabolic and bariatric surgery and may indicate metabolic dysfunction-associated steatotic liver disease, previously referred to as fatty liver disease. Clinically significant and persistently elevated liver enzymes should not be assumed to result from fatty liver and should prompt an investigation for other causes. If prophylactic cholecystectomy is planned during metabolic and bariatric surgery (to decrease risk of cholelithiasis), liver ultrasonography may be done.
Metabolic bone disease: Patients with obesity are at risk of vitamin D deficiencyvitamin D deficiency and metabolic bone disease, sometimes with secondary hyperparathyroidism. Patients should be screened and treated for these disorders before surgery, particularly because vitamin D deficiency is common preoperatively and poor absorption develops postoperatively.
Diabetes: Because poorly controlled diabetes increases the risk of adverse surgical outcomes, glycemic control should be optimized before surgery. A reasonable target range for HbA1c, corresponding to preoperative blood sugar control that may predict shorter hospital stays and improved bariatric procedure outcomes, is 6.5 to 7.0%.
Nutrition: Patients with obesity are at risk of nutritional deficiencies, which can be exacerbated postoperatively because food preferences and tolerance change, stomach acidity changes, and absorption from the small intestine is decreased. Routine measurement of vitamin D, vitamin B12, folate, and iron levels is recommended. For certain patients, measuring levels of other nutrients, such as thiamin (vitamin B1), may also be indicated.
Reproductive health: Women of reproductive age should be advised that their fertility may improve after surgery. These women should be counseled on contraceptive choice before and after bariatric procedures and should not become pregnant before surgery and postoperatively for 12 to 18 months. Patients having had malabsorptive procedures should have nutritional surveillance and laboratory testing for nutrient deficiencies during subsequent pregnancies.
Risks of Metabolic and Bariatric Surgery
Perioperative risks are lowest when metabolic and bariatric surgery is done in an accredited center.
Complications include
Gastric and/or anastomotic leaks (in 1 to 3%)
Pulmonary complications (eg, ventilator dependence, pneumonia, pulmonary embolism)
Wound infection
Incisional hernia
Gastrointestinal bleeding
Ventral hernia
These complications can cause significant morbidity, prolong hospitalization, and increase costs. Tachycardia may be the only early sign of anastomotic leak.
Later problems may include prolonged nausea and vomiting secondary to small-bowel obstruction and anastomotic stenosis.
Nutritional deficiencies (eg, protein-energy undernutrition, vitamin B12 deficiency, iron deficiency) may result from inadequate intake, inadequate supplementation, or malabsorption. Malodorous flatulence, diarrhea, or both may develop, particularly after malabsorptive procedures. Calcium and vitamin D absorption may be impaired, causing deficiencies and sometimes hypocalcemia and secondary hyperparathyroidism. With prolonged vomiting, thiamin deficiency may occur.
Patients may have symptoms of reflux, especially after sleeve gastrectomy. During rapid weight loss, cholelithiasis (often symptomatic), gout, and nephrolithiasis may develop. Concurrent cholecystectomy is considered if patients have preoperative symptomatic biliary disease but is no longer performed prophylactically.
Incidence of psychologic disorders such as depression is increased in patients having metabolic and bariatric surgery. A 2016 meta-analysis confirmed this increase in preoperative depression and reported a postoperative decrease in the prevalence and severity of depression (1). In a large review of retrospective and prospective studies, self-harm and suicide were higher in patients after metabolic and bariatric surgery than in control subjects; various presurgical and postsurgical factors may be involved (2). Incidence of alcohol use disorder also appears to be increased after bariatric surgery (3).
Eating habits may be disordered. Adjusting to new eating habits can be difficult.
Risks references
1. Dawes AJ, Maggard-Gibbons M, Maher AR, et al: Mental health conditions among patients seeking and undergoing bariatric surgery: A meta-analysis. JAMA 315 (2):150–163, 2016. doi: 10.1001/jama.2015.18118
2. Castaneda D, Popov VB, Wander P, et al:Risk of suicide and self-harm is increased after bariatric surgery—A systematic review and meta-analysis. Obes Surg 29 (1):322–333, 2019. doi: 10.1007/s11695-018-3493-4
3. Heinberg LJ, Ashton K, Coughlin J: Alcohol and bariatric surgery: review and suggested recommendations for assessment and management. Surg Obes Relat Dis 8 (3):357-363, 2012. doi: 10.1016/j.soard.2012.01.016
Prognosis for Metabolic and Bariatric Surgery
In hospitals accredited by the American Society of Bariatric Surgery as centers of excellence (COE), in-hospital mortality was 0.08% (1). However, some data indicate that lower rates of serious complications are predicted more accurately by the number of procedures done in the hospital and by the surgeon than by COE status. Risk of death associated with bariatric surgery is about 0.1%; overall risk of serious complications is about 4%. For most patients, the risk of obesity and its complications outweigh the immediate risk of surgery (2).
Factors that predict higher risk of mortality include a history of deep venous thrombosis or pulmonary embolism, obstructive sleep apnea, and poor functional status. Other factors such as severe obesity (BMI > 50), older age, and male sex have also been associated with higher risk, but the evidence is inconsistent.
Average excess weight loss depends on the procedure.
For sleeve gastrectomy, loss of excess weight is
33 to 58% at 2 years
58 to 72% at 3 to 6 years
For Roux-en-Y gastric bypass, loss of excess weight is
50 to 65% after 2 years
Weight loss after RYGB is maintained for up to 10 years.
For BPD-DS and SADI-S, patients lose
75 to 90% of excess body weight
In people who have severe obesity (≥ 50 kg/m2), weight loss is greater after BPD-DS than after RYGB (3).
Comorbidities that tend to abate or resolve after metabolic and bariatric surgery include a large number of cardiovascular risk factors (eg, dyslipidemia, hypertension, diabetes), cardiovascular disorders, diabetes, obstructive sleep apnea, osteoarthritis, and depression. Diabetes is particularly likely to remit (eg, with RYGB, up to 62% of patients at 6 years [4]). All-cause mortality decreases by 25%, primarily because cardiovascular and cancer mortality is reduced.
Prognosis references
1. Gebhart A, Young M, Phelan M, Nguyen NT: Impact of accreditation in bariatric surgery. Surg Obes Relat Dis 10 (5):767–773, 2014. doi: 10.1016/j.soard.2014.03.009 Epub 2014 Mar 15.
2. American Society for Metabolic and Bariatric Surgery: Metabolic and Bariatric Surgery. Published 2021. Accessed 10/31/23.
3. Prachand VN, Davee RT, Alverdy JC: Duodenal switch provides superior weight loss in the super-obese (BMI ≥ 50 kg/m2) compared with gastric bypass. Ann Surg 244 (4):611–619, 2006. doi: 10.1097/01.sla.0000239086.30518.2a
4. Courcoulas AP, King WC, Belle SH, et al; Seven-year weight trajectories and health outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) study. JAMA Surg. 153 (5), 20:427–434. doi: 10.1001/jamasurg.2017.5025.
Follow-up after Bariatric Surgery
Regular long-term follow-up after metabolic and bariatric surgery helps ensure adequate weight loss and prevent complications. After Roux-en-Y gastric bypass or sleeve gastrectomy, patients should be monitored every 4 to 12 weeks during the period of rapid weight loss (usually about the first 6 months after surgery), then every 6 to 12 months thereafter.
Weight and blood pressure are checked, and eating habits are reviewed. Blood tests (usually complete blood count; electrolyte, glucose, blood urea nitrogen, creatinine, albumin, and protein levels; and liver tests) are done at regular intervals. Glycosylated Hb (HbA1c) and fasting lipid levels should be monitored if they were abnormal before surgery. Depending on the type of procedure, vitamin and mineral levels, including calcium, Weight and blood pressure are checked, and eating habits are reviewed. Blood tests (usually complete blood count; electrolyte, glucose, blood urea nitrogen, creatinine, albumin, and protein levels; and liver tests) are done at regular intervals. Glycosylated Hb (HbA1c) and fasting lipid levels should be monitored if they were abnormal before surgery. Depending on the type of procedure, vitamin and mineral levels, including calcium,vitamin D, vitamin B12, folate, iron, and thiamin (vitamin B1), may need to be monitored. Because secondary hyperparathyroidism is a risk, parathyroid hormone levels should also be monitored. Bone density should be measured after sleeve gastrectomy or Roux-en-Y gastric bypass. , vitamin B12, folate, iron, and thiamin (vitamin B1), may need to be monitored. Because secondary hyperparathyroidism is a risk, parathyroid hormone levels should also be monitored. Bone density should be measured after sleeve gastrectomy or Roux-en-Y gastric bypass.
Clinicians should check for any changes in response to antihypertensives, insulin, oral hypoglycemics, or lipid-lowering medications during the period of rapid weight loss after surgery. Clinicians should check for any changes in response to antihypertensives, insulin, oral hypoglycemics, or lipid-lowering medications during the period of rapid weight loss after surgery.
Patients should also be regularly screened for depression and alcohol use, particularly if alcohol use was heavy preoperatively.
To minimize risk of hypoglycemia (due to increased insulin sensitivity after bariatric surgery) in patients with diabetes, clinicians should adjust the dose of insulin and decrease the dose of oral hypoglycemics (particularly sulfonylureas) or stop them after Roux-en-Y gastric bypass or sleeve gastrectomy.sensitivity after bariatric surgery) in patients with diabetes, clinicians should adjust the dose of insulin and decrease the dose of oral hypoglycemics (particularly sulfonylureas) or stop them after Roux-en-Y gastric bypass or sleeve gastrectomy.
Key Points
Consider weight loss surgery if patients have a BMI of > 35 kg/m2 or a BMI of > 30 kg/m2 plus obesity-related comorbidities (eg, diabetes, hypertension, obstructive sleep apnea, high-risk lipid profile).
Contraindications to metabolic and bariatric surgery include an uncontrolled psychiatric disorder (eg, major depression), substance or alcohol use disorder, cancer that is not in remission, or another life-threatening disorder and inability to comply with nutritional requirements (including life-long vitamin replacement when indicated).
Sleeve gastrectomy is currently the most commonly used metabolic and bariatric surgical procedure in the United States.
Monitor patients regularly after surgery for maintenance of weight loss, resolution of weight-related comorbidities, and complications of surgery (eg, nutritional deficiencies, metabolic bone disease, gout, cholelithiasis, nephrolithiasis, depression, alcohol use disorder).







