



Gout is a disorder caused by hyperuricemia (serum urate > 6.8 mg/dL [> 0.4 mmol/L]) that results in the precipitation of monosodium urate crystals in and around joints, most often causing recurrent acute or chronic arthritis. The initial attack (flare) of gout is usually monarticular and often involves the 1st metatarsophalangeal joint. Symptoms of gout include acute, severe pain, tenderness, warmth, redness, and swelling. Definite diagnosis requires identification of crystals in synovial fluid. Treatment of acute flares is with anti-inflammatory drugs. The frequency of flares can be reduced by regular use of nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or both plus persistent lowering of the serum urate level below its saturation level (< 6.8 mg/dL [< 0.4 mmol/L) with allopurinol, febuxostat, or uricosuric drugs such as probenecid.Gout is a disorder caused by hyperuricemia (serum urate > 6.8 mg/dL [> 0.4 mmol/L]) that results in the precipitation of monosodium urate crystals in and around joints, most often causing recurrent acute or chronic arthritis. The initial attack (flare) of gout is usually monarticular and often involves the 1st metatarsophalangeal joint. Symptoms of gout include acute, severe pain, tenderness, warmth, redness, and swelling. Definite diagnosis requires identification of crystals in synovial fluid. Treatment of acute flares is with anti-inflammatory drugs. The frequency of flares can be reduced by regular use of nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or both plus persistent lowering of the serum urate level below its saturation level (allopurinol, febuxostat, or uricosuric drugs such as probenecid.








(See also Overview of Crystal-Induced Arthritides.)
Gout is more common among men than women. Usually, gout develops during middle age in men and after menopause in women. Gout is rare in younger people but is often more severe in people who develop the disorder before age 30. Gout often runs in families. Patients with metabolic syndrome are at increased risk of gout.
Pathophysiology of Gout
The greater the degree and duration of hyperuricemia, the greater is the likelihood that gout will develop. Urate levels can be elevated because of
Decreased renal (most common) or gastrointestinal excretion
Increased production (rare)
Increased purine intake (usually in combination with decreased excretion)
Why only some people with elevated serum uric acid (urate) levels develop gout flares is not known.
Decreased renal excretion is by far the most common cause of hyperuricemia. It may be hereditary (eg, due to variations in uric acid transporter efficiency) and also occurs in patients receiving diuretics and in those with diseases that decrease the glomerular filtration rate (GFR). Ethanol increases purine catabolism in the liver and increases the formation of lactic acid, which blocks urate secretion by the renal tubules, and ethanol may also stimulate liver urate synthesis. Lead poisoning and cyclosporine, usually in the higher doses given to transplant patients, alter renal tubular function leading to urate retention.is by far the most common cause of hyperuricemia. It may be hereditary (eg, due to variations in uric acid transporter efficiency) and also occurs in patients receiving diuretics and in those with diseases that decrease the glomerular filtration rate (GFR). Ethanol increases purine catabolism in the liver and increases the formation of lactic acid, which blocks urate secretion by the renal tubules, and ethanol may also stimulate liver urate synthesis. Lead poisoning and cyclosporine, usually in the higher doses given to transplant patients, alter renal tubular function leading to urate retention.
Increased production of urate may be caused by increased nucleoprotein turnover in hematologic conditions (eg, lymphoma, leukemia, hemolytic anemia) and in conditions with increased rates of cellular proliferation and cell death (eg, psoriasis, cytotoxic cancer therapy, radiation therapy). Increased urate production may also occur as a primary hereditary abnormality and in obesity, because urate production correlates with body surface area. In most cases, the cause of urate overproduction is unknown, but rarely can be attributable to enzyme abnormalities; deficiency of hypoxanthine-guanine phosphoribosyltransferase (complete deficiency is Lesch-Nyhan syndrome) is a possible cause, as is overactivity of phosphoribosylpyrophosphate synthetase.
Increased intake of purine-rich foods (eg, liver, kidney, anchovies, asparagus, consommé, herring, meat gravies and broths, mushrooms, mussels, sardines, sweetbreads) can contribute to hyperuricemia. Beer, including nonalcoholic beer, is particularly rich in guanosine, a purine nucleoside. However, a strict low-purine diet lowers serum urate by only about 1 mg/dL (0.1 mmol/L) and thus is rarely sufficient therapy for patients with gout.
Urate precipitates as needle-shaped monosodium urate (MSU) crystals, which are deposited extracellularly in avascular tissues (eg, cartilage) or in relatively avascular tissues (eg, tendons, tendon sheaths, ligaments, walls of bursae) and skin around cooler distal joints and tissues (eg, ears, finger pads). In severe, long-standing hyperuricemia, MSU crystals may be deposited in larger central joints and in the parenchyma of organs such as the kidney. At the acid pH of urine, urate precipitates readily as small platelike or diamond-shaped uric acid crystals that may aggregate to form gravel or stones, which may obstruct urine outflow. Tophi are MSU crystal aggregates that most often develop in joint and cutaneous tissue. They are usually encased in a fibrous granulomatous matrix, which prevents them from causing acute inflammation.
Acute gouty arthritis may be triggered by trauma, medical stress (eg, pneumonia or other infection), surgery, use of thiazide diuretics or drugs with hypouricemic effects (eg, allopurinol, febuxostat, probenecid, nitroglycerin), or indulgence in purine-rich food or alcohol. Flares are often precipitated by a sudden increase or, more commonly, a sudden decrease in serum urate levels. Why acute flares follow some of these precipitating conditions is unknown. Tophi in and around joints can limit motion and cause deformities, called chronic tophaceous gouty arthritis. Gout increases the risk of developing Acute gouty arthritis may be triggered by trauma, medical stress (eg, pneumonia or other infection), surgery, use of thiazide diuretics or drugs with hypouricemic effects (eg, allopurinol, febuxostat, probenecid, nitroglycerin), or indulgence in purine-rich food or alcohol. Flares are often precipitated by a sudden increase or, more commonly, a sudden decrease in serum urate levels. Why acute flares follow some of these precipitating conditions is unknown. Tophi in and around joints can limit motion and cause deformities, called chronic tophaceous gouty arthritis. Gout increases the risk of developingsecondary osteoarthritis.
Symptoms and Signs of Gout


© Springer Science+Business Media
Acute gouty arthritis usually begins with sudden onset of pain (often nocturnal). The metatarsophalangeal joint of a great toe is most often involved (called podagra), but the instep, ankle, knee, wrist, and elbow are also common sites. Rarely, the hip, shoulder, sacroiliac, sternoclavicular, or cervical spine joints are involved. The pain becomes progressively more severe, usually over a few hours, and is often excruciating. Swelling, warmth, redness, and exquisite tenderness may suggest infection. The overlying skin may become tense, warm, shiny, and red or purplish. Fever, tachycardia, chills, and malaise sometimes occur.
Course
The first few flares usually affect only a single joint and last only a few days. Later flares may affect several joints simultaneously or sequentially and persist up to 3 weeks if untreated. Subsequent flares develop after progressively shorter symptom-free intervals. Eventually, multiple flares may occur each year. If ongoing urate-lowering therapy is not initiated, patients can develop chronic deforming arthritis from tophaceous gout due to ongoing urate deposition.
Tophi


© Springer Science+Business Media


© Springer Science+Business Media
Palpable tophi develop in patients with gout and can rarely occur in patients who have never had acute gouty arthritis. They are usually firm yellow or white papules or nodules, single or multiple. They can develop in various locations, commonly the fingers, hands, feet, and around the olecranon or Achilles tendon. Tophi can also develop in the kidneys and other organs and under the skin on the ears. Patients with osteoarthritic Heberden nodes may develop tophi in the nodes. This development occurs most often in older women taking diuretics, and these can become dramatically inflamed and misdiagnosed as inflammatory osteoarthritis. Normally painless, tophi, especially in the olecranon bursae, can become acutely inflamed and painful, often after mild or inapparent injury. Tophi may erupt through the skin, discharging chalky masses of urate crystals. These sinus tracts can become infected. Tophi in and around joints may eventually cause deformities and secondary osteoarthritis.
Complications of gout
Gouty arthritis can cause pain, deformity, and limited joint motion. Inflammation can be flaring in some joints while subsiding in others. Patients with gout may develop urolithiasis with uric acid stones or calcium oxalate stones.
Complications of gout include renal obstruction and infection, with secondary tubulointerstitial disease. Untreated progressive renal dysfunction, most often related to coexisting hypertension or, less often, some other cause of nephropathy, further impairs excretion of urate, accelerating crystal deposition in tissues.
Cardiovascular disease, obstructive sleep apnea, nonalcoholic fatty liver disease, and components of metabolic syndrome are common among patients with gout.
Diagnosis of Gout
Clinical criteria
Synovial fluid analysis
The diagnosis of gout should be suspected in patients with acute monoarticular arthritis or oligoarticular arthritis, particularly older adults or those with other risk factors. Podagra and recurrent instep inflammation are particularly suggestive. Previous flares that began explosively and resolved spontaneously within 7 to 10 days are also characteristic. Similar symptoms can result from the following:
Acute calcium pyrophosphate arthritis (calcium pyrophosphate dihydrate (CPPD) crystal deposition disease) (however, calcium pyrophosphate deposition generally occurs in larger joints, is not associated with tophi, and its clinical course is often milder but protracted)
Acute rheumatic fever with joint involvement and juvenile idiopathic arthritis (however, these disorders occur mostly in young people, who rarely get gout)
Rheumatoid arthritis (RA) (however, RA tends to be symmetrical and persistent, with more affected joints during a flare, flares persisting for longer periods of time, and flares in all joints subsiding together; whereas in gout, inflammation is usually flaring in some joints while subsiding in others)
Acute fracture in patients unable to provide a history of injury (particularly metatarsal stress fractures)
Acute infectious arthritis or chronic infectious arthritis (differentiation requires synovial fluid analysis)
Palindromic rheumatism
Acute calcific periarthritis caused by basic calcium phosphate or calcium oxalate crystal deposition diseasebasic calcium phosphate or calcium oxalate crystal deposition disease
Palindromic rheumatism is characterized by acute, recurrent flares of inflammation in or near one or occasionally several joints or tendon sheaths with spontaneous resolution; pain and erythema can be as severe as in gout. Flares often subside spontaneously and completely in 1 to 3 days. Such flares may herald the onset of RA, and rheumatoid factor tests can help in differentiation; they are positive in about 50% of patients (these tests are positive in 10% of gouty patients also).
Synovial fluid analysis
If acute gouty arthritis is suspected, arthrocentesis and synovial fluid analysis should be done at the initial presentation. A typical recurrence in a patient with previously documented gout does not mandate arthrocentesis, but it should be done if there is any question of the diagnosis or if the patient’s risk factors or any clinical characteristics suggest infectious arthritis. In some cases, a diagnosis of gout may be reasonably presumed based on the patient’s history and clinical features or on imaging results in cases when joint fluid cannot be obtained; however, every attempt should be made to document the presence of MSU crystals in synovial fluid from an affected joint.

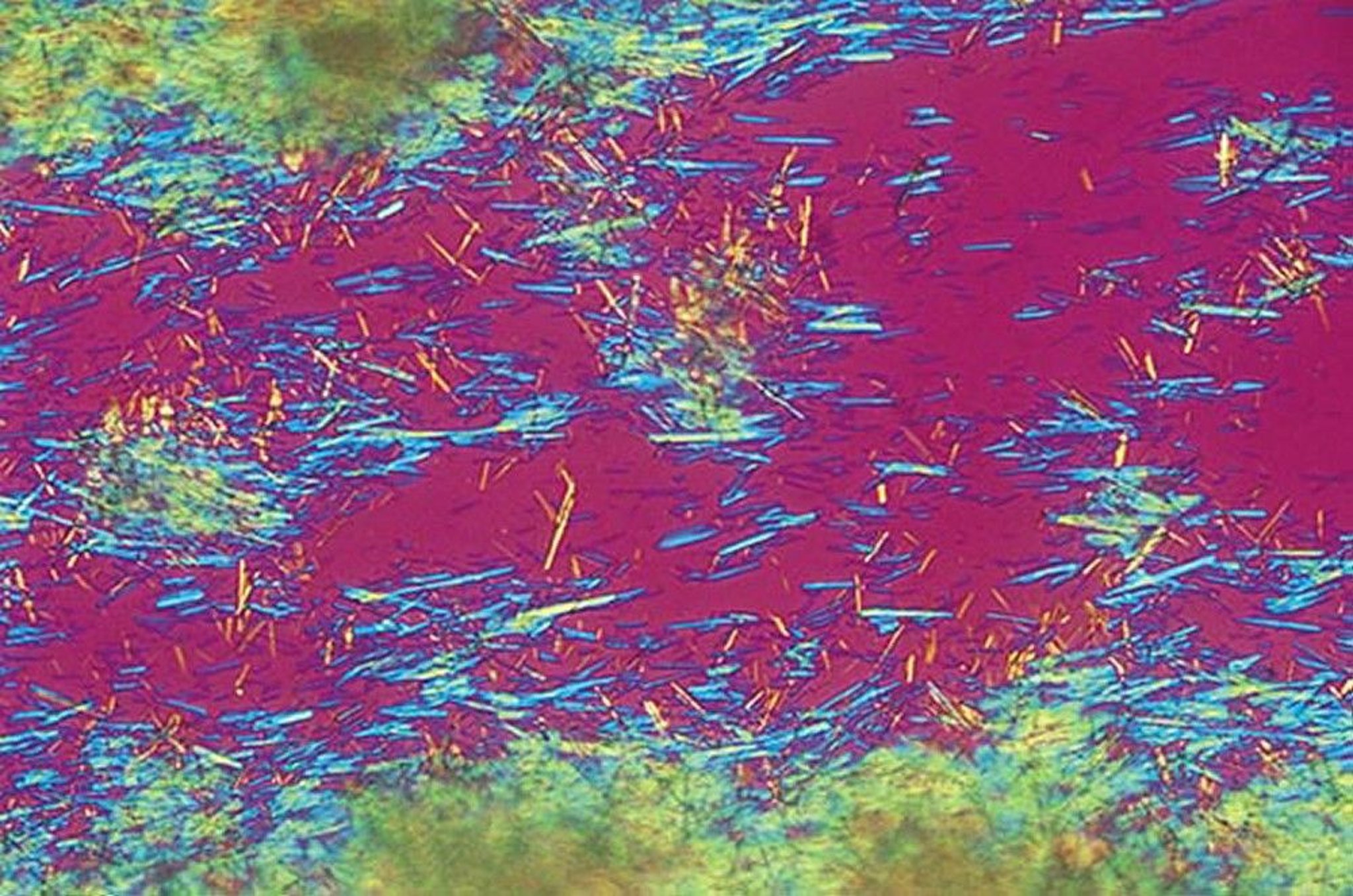
By permission of the publisher. From Myers S: Atlas of Rheumatology. Edited by G Hunder. Philadelphia, Current Medicine, 2005.
Synovial fluid analysis can confirm the diagnosis by identifying needle-shaped, strongly negatively birefringent urate crystals that are free in the fluid or engulfed by phagocytes. Synovial fluid during flares has inflammatory characteristics (see table Microscopic Examination of Crystals in Joints), usually 2,000 to 100,000 white blood cells/mcL, with > 80% polymorphonuclear white blood cells. These findings overlap considerably with infectious arthritis, which must be excluded by Gram stain (which is insensitive) and culture.
Microscopic Examination of Crystals in Joints
Crystal Type | Birefringence | Elongation* | Shape | Length (micrometer) |
|---|---|---|---|---|
Monosodium urate | Strong | Negative | Needle- or rod- shaped | 2–15 |
Weak or often not birefringent | Positive | Rhomboid- or rod- shaped | 2–15 | |
Calcium oxalate (rare)† | Weak or strong | Positive or indeterminate | Bipyramidal | 5–30 |
Not birefringent with polarized light | — | Shiny, coinlike, or slightly irregular (often too small to delineate) | 3–65 (aggregates) | |
* Elongation is determined by inserting an additional red plate or compensator between the two polarizing plates in the microscope and aligning a crystal with an orienting arrow denoting the axis of slow vibration. Crystals that have negative elongation are yellow parallel to the axis of slow vibration marked on the compensator; positive elongation appears blue in the same direction. In clinical practice, these have also been termed negative or positive birefringence. | ||||
† These crystals occur primarily in patients with renal failure. | ||||
Serum urate level
An elevated serum urate level supports the diagnosis of gout but is neither specific nor sensitive; at least 30% of patients have a normal serum urate level during an acute flare in part due to the uricosuric properties of the proinflammatory cytokine interleukin-6 (IL-6) or because a sudden lowering of the serum urate precipitated the flare. However, the baseline serum urate level between flares reflects the size of the extracellular miscible urate pool. The level should be measured on 2 or 3 occasions in patients with newly proven gout to establish a baseline. Quantitation of urinary uric acid excretion to differentiate between overproduction and underexcretion is no longer recommended; it does not predict a patient's response to allopurinol or febuxostat (both of which decrease uric acid production). The serum urate level can be low after initiation of therapy, but flares can continue to occur as long as tissue deposits remain. The dissolution of the urate deposits may take many months after initiating therapy.An elevated serum urate level supports the diagnosis of gout but is neither specific nor sensitive; at least 30% of patients have a normal serum urate level during an acute flare in part due to the uricosuric properties of the proinflammatory cytokine interleukin-6 (IL-6) or because a sudden lowering of the serum urate precipitated the flare. However, the baseline serum urate level between flares reflects the size of the extracellular miscible urate pool. The level should be measured on 2 or 3 occasions in patients with newly proven gout to establish a baseline. Quantitation of urinary uric acid excretion to differentiate between overproduction and underexcretion is no longer recommended; it does not predict a patient's response to allopurinol or febuxostat (both of which decrease uric acid production). The serum urate level can be low after initiation of therapy, but flares can continue to occur as long as tissue deposits remain. The dissolution of the urate deposits may take many months after initiating therapy.
Imaging
X-rays of the affected joint may be taken to look for bony erosions or tophi, but they are unnecessary if the diagnosis of acute gout has been established by synovial fluid analysis and rarely show erosions at the time of first flares. In calcium pyrophosphate arthritis, radiopaque deposits may sometimes be present in fibrocartilage, hyaline articular cartilage (particularly the knee), or both, but calcinosis can be seen in the absence of acute flares.
Ultrasonography is more sensitive (although operator-dependent) than plain x-rays for the diagnosis of gout. Urate deposition over the articular cartilage (double-contour sign) and clinically inapparent tophi are characteristic changes. These findings may be evident even before the first gout flare. Dual-energy CT scans (DECTs) can also reveal uric acid deposits and can be useful if the diagnosis is unclear based on standard clinical evaluation and testing, particularly if synovial fluid aspiration and analysis cannot be done.


Image courtesy of N. Lawrence Edwards, MD.


Images courtesy of Brian F. Mandell, MD.
Diagnosis of chronic gouty arthritis
Chronic gouty arthritis should be considered in patients with persistent unexplained joint disease or subcutaneous or bony tophi. Plain x-rays of the 1st metatarsophalangeal joint or other affected joint may be useful. These x-rays may show punched-out lesions of subchondral bone with overhanging bony margins, most commonly in the 1st metatarsophalangeal joint; lesions must be ≥ 5 mm in diameter to be visible on x-ray. Joint space is typically preserved until very late in the course of disease. Synovial fluid findings from chronic effusions of affected joints are usually diagnostic.
Diagnostic ultrasonography is increasingly used to detect a typical double-contour sign suggesting urate crystal deposition, but sensitivity is operator-dependent and differentiation from calcium pyrophosphate crystal deposits may be more difficult to do conclusively.
Prognosis for Gout
With early gout diagnosis, life-long urate-lowering therapy enables most patients to live a normal life. For many patients with advanced disease, aggressive lowering of the serum urate level can resolve tophi and improve joint function. Gout is generally more severe in patients whose initial symptoms appear before age 30 and whose baseline serum uric acid level is > 9 mg/dL (> 0.5 mmol/L). The high prevalence of metabolic syndrome and cardiovascular disease probably increases mortality in patients with gout.
Some patients do not improve sufficiently with treatment. The usual reasons include inadequate education provided to patients, nonadherence, alcoholism, and mainly undertreatment of the hyperuricemia by physicians.
Treatment of Gout
Termination of an acute flare with nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, corticosteroids, or an interleukin-1 (IL-1) antagonistTermination of an acute flare with nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, corticosteroids, or an interleukin-1 (IL-1) antagonist
Prevention of further deposition of monosodium urate (MSU) crystals, reduction in flare incidence, and resolution of existing tophi by lowering the serum urate level (by decreasing urate production with allopurinol or febuxostat, dissolving deposits with uricase replacement therapy, or increasing urate excretion with probenecid)Prevention of further deposition of monosodium urate (MSU) crystals, reduction in flare incidence, and resolution of existing tophi by lowering the serum urate level (by decreasing urate production with allopurinol or febuxostat, dissolving deposits with uricase replacement therapy, or increasing urate excretion with probenecid)
Prevention of recurrent acute flares with daily colchicine or an NSAIDPrevention of recurrent acute flares with daily colchicine or an NSAID
Treatment of coexisting hypertension, hyperlipidemia, and obesity and avoidance of excess dietary purines
(See also the 2020 American College of Rheumatology Guideline for the Management of Gout.)
Treatment of acute flares
Nonsteroidal anti-inflammatory drugs (NSAIDs) are effective in treating acute flares and are generally well-tolerated. However, they can have adverse effects, including gastrointestinal upset or bleeding, hyperkalemia, increases in creatinine, and fluid retention. Older and dehydrated patients are at particular risk, especially if there is a history of renal disease. Virtually any NSAID used in anti-inflammatory (high) doses is effective and is likely to exert an analgesic effect beginning within a few hours. Treatment should be continued for several days after the pain and signs of inflammation have resolved to prevent relapse.
Oral colchicine,Oral colchicine, a traditional therapy, produces a dramatic response in some patients if begun soon after the onset of symptoms; it is most effective if started within 12 to 24 hours of an acute flare. A dose of 1.2 mg can be followed with 0.6 mg 1 hour later; joint pain tends to decrease after 12 to 24 hours and sometimes ceases within 3 to 7 days, but continued dosing is generally needed to achieve resolution, which may take time. If colchicine is tolerated, 0.6 to 1.2 mg once a day can be continued as the flare subsides. Renal insufficiency and drug interactions, especially with clarithromycin and some statins, may warrant reduction of dosage or use of other treatments. Gastrointestinal upset and diarrhea are common adverse effects.a traditional therapy, produces a dramatic response in some patients if begun soon after the onset of symptoms; it is most effective if started within 12 to 24 hours of an acute flare. A dose of 1.2 mg can be followed with 0.6 mg 1 hour later; joint pain tends to decrease after 12 to 24 hours and sometimes ceases within 3 to 7 days, but continued dosing is generally needed to achieve resolution, which may take time. If colchicine is tolerated, 0.6 to 1.2 mg once a day can be continued as the flare subsides. Renal insufficiency and drug interactions, especially with clarithromycin and some statins, may warrant reduction of dosage or use of other treatments. Gastrointestinal upset and diarrhea are common adverse effects.
IV colchicineIV colchicine is no longer available in the US.
Corticosteroids are used to treat acute flares. Aspiration of affected joints, followed by instillation of corticosteroid ester crystal suspension, is very effective, particularly for monarticular symptoms; prednisolone tebutate 4 to 40 mg or prednisolone acetate 5 to 25 mg can be used, with dose depending on the size of the affected joint. Oral prednisone (about 0.5 mg/kg once a day), IM or IV corticosteroids, or single-dose adrenocorticotropic hormone (ACTH) 80 U IM is effective, particularly if multiple joints are involved. As with NSAID therapy, corticosteroids should be continued for a few days after the flare fully resolves to prevent relapse.are used to treat acute flares. Aspiration of affected joints, followed by instillation of corticosteroid ester crystal suspension, is very effective, particularly for monarticular symptoms; prednisolone tebutate 4 to 40 mg or prednisolone acetate 5 to 25 mg can be used, with dose depending on the size of the affected joint. Oral prednisone (about 0.5 mg/kg once a day), IM or IV corticosteroids, or single-dose adrenocorticotropic hormone (ACTH) 80 U IM is effective, particularly if multiple joints are involved. As with NSAID therapy, corticosteroids should be continued for a few days after the flare fully resolves to prevent relapse.
If monotherapy is ineffective or doses (eg, of NSAIDs) are limited by toxicity, colchicine can be combined with NSAIDs or corticosteroids.If monotherapy is ineffective or doses (eg, of NSAIDs) are limited by toxicity, colchicine can be combined with NSAIDs or corticosteroids.
In addition to NSAIDs or corticosteroids, supplementary analgesics, rest, ice application, and splinting of the inflamed joint may be helpful. If patients are taking urate-lowering drugs when an acute flare begins, the drugs should be continued at the same dose; dose adjustments are deferred until the flare has subsided. There is no contraindication to initiating urate-lowering therapy during an acute flare if appropriate antiinflammatory therapy is being provided.
If corticosteroids, colchicine, and NSAIDs are contraindicated or ineffective, an IL-1 antagonist, such as anakinra, can be used. Anakinra may hasten resolution of a flare and shorten the hospital stay of a patient with multiple comorbidities that limit the use of the other drugs. Anakinra is typically given as 100 mg subcutaneously once a day until symptoms resolve. Anakinra has the advantage of not affecting glucose levels or renal function or causing fluid retention and can be used in a patient with an active infection that is being appropriately treated. Due to practical considerations (eg, cost), anakinra is not typically used to treat acute gout flares in the outpatient setting.If corticosteroids, colchicine, and NSAIDs are contraindicated or ineffective, an IL-1 antagonist, such as anakinra, can be used. Anakinra may hasten resolution of a flare and shorten the hospital stay of a patient with multiple comorbidities that limit the use of the other drugs. Anakinra is typically given as 100 mg subcutaneously once a day until symptoms resolve. Anakinra has the advantage of not affecting glucose levels or renal function or causing fluid retention and can be used in a patient with an active infection that is being appropriately treated. Due to practical considerations (eg, cost), anakinra is not typically used to treat acute gout flares in the outpatient setting.
Prevention of recurrent flares
The frequency of acute flares is reduced by taking 0.6 mg of colchicine once or twice a day (maximum 1.2 mg per day depending on tolerance and renal function). An extra two 0.6-mg tablets of colchicine taken at the first suggestion of a flare may abort flares. If the patient is taking prophylactic doses of colchicine and has taken higher doses of colchicine to treat an acute flare within the past 2 weeks, an NSAID or corticosteroid should be used instead to try to abort the flare.The frequency of acute flares is reduced by taking 0.6 mg of colchicine once or twice a day (maximum 1.2 mg per day depending on tolerance and renal function). An extra two 0.6-mg tablets of colchicine taken at the first suggestion of a flare may abort flares. If the patient is taking prophylactic doses of colchicine and has taken higher doses of colchicine to treat an acute flare within the past 2 weeks, an NSAID or corticosteroid should be used instead to try to abort the flare.
A (reversible) neuropathy and/or myopathy can develop during chronic colchicine ingestion. This condition is more likely to occur in patients with renal insufficiency, and in patients also receiving certain statins or macrolides, but can rarely occur in patients with none of these risk factors.A (reversible) neuropathy and/or myopathy can develop during chronic colchicine ingestion. This condition is more likely to occur in patients with renal insufficiency, and in patients also receiving certain statins or macrolides, but can rarely occur in patients with none of these risk factors.
Flare frequency can also be decreased with daily low-dose NSAIDs if renal function allows. Chronic corticosteroid use is not an ideal prophylactic therapy because of its adverse effect potential.
Lowering the serum urate level
Colchicine, NSAIDs, and corticosteroids do not retard the progressive joint damage caused by tophi, because they do not lower the serum urate level. Joint damage can be prevented and, if present, may be reversed with urate-lowering drugs. Tophaceous deposits are resorbed by lowering serum urate or dissolved with uricase replacement therapy. Maintaining a serum urate level below the saturation point (target is usually < 6 mg/dL [< 0.35 mmol/L]) will ultimately decrease the frequency of acute arthritic flares as the deposits are dissolved. This decrease is accomplished byColchicine, NSAIDs, and corticosteroids do not retard the progressive joint damage caused by tophi, because they do not lower the serum urate level. Joint damage can be prevented and, if present, may be reversed with urate-lowering drugs. Tophaceous deposits are resorbed by lowering serum urate or dissolved with uricase replacement therapy. Maintaining a serum urate level below the saturation point (target is usually < 6 mg/dL [< 0.35 mmol/L]) will ultimately decrease the frequency of acute arthritic flares as the deposits are dissolved. This decrease is accomplished by
Blocking urate production with xanthine oxidase inhibitors (XOI) (allopurinol or febuxostat)Blocking urate production with xanthine oxidase inhibitors (XOI) (allopurinol or febuxostat)
Increasing urate excretion with a uricosuric drug (probenecid or losartan)Increasing urate excretion with a uricosuric drug (probenecid or losartan)
Using both types of drugs together in severe tophaceous gout or in patients intolerant of higher doses of a XOI
Increasing urate excretion by converting urate to allantoin, which is more soluble and readily excreted, with uricase replacement therapy in patients such as those who have severe tophaceous gout or did not respond to other urate-lowering therapy
Urate-lowering therapy is indicated for patients with
Tophaceous deposits
Evidence of joint damage due to gout on imaging studies
Frequent or disabling flares (eg, > 2 flares times a year) of gouty arthritis
Urolithiasis
Patients with infrequent flares but whose serum uric acid level is > 9 mg/dL (> 0.5 mmol/L) or for whom having any flares poses particular hardship
Multiple comorbidities (eg, peptic ulcer disease, chronic kidney disease) that are relative contraindications to the drugs used to treat recurrent acute flares (NSAIDs or corticosteroids)
Hyperuricemia is not usually treated in the absence of gout flares or uric acid nephrolithiasis.
The goal of urate-lowering therapy is to lower the serum urate level. If tophi are not present, a reasonable target level is < 6 mg/dL (< 0.35 mmol/L), which is below the level of saturation (> 6.8 mg/dL [0.4 mmol/L] at normal core body temperature and pH). Compelling data demonstrate decreased frequency of flares when the serum urate level decreases to < 6 mg/dL with this treat-to-target strategy. Two randomized controlled trials have established that significantly fewer patients with a serum urate level < 6 mg/dL experienced gout flares than those with a higher serum urate level. The patients with the target serum urate (< 6 mg/dL) who did flare had fewer gout flares than patients who were above this serum urate threshold (1).
If palpable tophi are present or if there is marked disability from tophaceous deposits, a reasonable goal is to dissolve them more rapidly, and this requires an even lower target level. The lower the serum urate level, the faster tophi resolve. After presumed complete dissolution of deposits, the serum urate can be allowed to increase to a level < 6 mg/dL.
Drugs are effective in lowering serum urate; dietary restriction of purines is less effective, but high intake of high-purine food, alcohol (beer in particular), and nonalcoholic beer should be avoided. Carbohydrate restriction (especially high-fructose corn syrup) and weight loss can lower serum urate level, particularly in patients with insulin resistance because high insulin levels suppress urate excretion. Intake of low-fat dairy products should be encouraged. Because acute flares tend to develop during the first months of urate-lowering therapy, such therapy should be started in conjunction with once or twice a day colchicine or NSAIDs. levels suppress urate excretion. Intake of low-fat dairy products should be encouraged. Because acute flares tend to develop during the first months of urate-lowering therapy, such therapy should be started in conjunction with once or twice a day colchicine or NSAIDs.
Resolution of tophi may take many months even with maintenance of serum urate at low levels. Serum urate should be measured periodically, usually monthly while determining required drug dosage and then at least yearly to confirm the effectiveness of therapy or more often if there are drug changes or weight gain. Urate-lowering therapy should not be stopped if a patient has a flare.
Allopurinol,Allopurinol, a xanthine oxidase inhibitor of urate synthesis, is the most commonly prescribed and preferred initial urate-lowering therapy. Uric acid stones or gravel may dissolve during allopurinol treatment. Treatment usually begins with 50 to100 mg orally once a day and can be slowly dose escalated up to 800 mg orally once a day. The dose can be split if single daily dosing causes gastrointestinal distress. Some clinicians recommend decreasing the starting dose in patients with renal insufficiency (eg, 50 mg orally once a day if creatinine clearance is < 60 mL/min/1.73 m2) to decrease the incidence of rare but severe systemic hypersensitivity reactions; however, data that confirm the effectiveness of this intervention are limited. The final dose of allopurinol should be determined by the target serum urate level. The most commonly used daily dose is 300 mg, but this dose is effective in lowering serum uric acid levels to < 6 mg/dL (< 0.35 mmol/L) in fewer than 40% of patients with gout. Absorption of allopurinol may decrease at doses higher than 300 mg, so split dosing (eg, twice daily dosing) should be considered.should be determined by the target serum urate level. The most commonly used daily dose is 300 mg, but this dose is effective in lowering serum uric acid levels to allopurinol may decrease at doses higher than 300 mg, so split dosing (eg, twice daily dosing) should be considered.
Adverse effects of allopurinol include mild gastrointestinal distress and rash, which can be a harbinger of Stevens-Johnson syndrome, life-threatening hepatitis, vasculitis, or leukopenia. Adverse effects are more common among patients with renal dysfunction. HLA-B*5801 carriers are at higher risk of Adverse effects of allopurinol include mild gastrointestinal distress and rash, which can be a harbinger of Stevens-Johnson syndrome, life-threatening hepatitis, vasculitis, or leukopenia. Adverse effects are more common among patients with renal dysfunction. HLA-B*5801 carriers are at higher risk ofallopurinol reactions, and HLA-B*5801 prevalence varies by race (2). Therefore, the 2020 American College of Rheumatology Guideline for the Management of Gout recommends testing patients of Southeast Asian descent (eg, Han Chinese, Korean, Thai) and Black American patients for HLA B*5801 and using an alternative drug if that genetic marker is present. Allopurinol is contraindicated in patients taking azathioprine or mercaptopurine because it can decrease metabolism of these drugs and thus potentiate their immunosuppressive and cytolytic effects. Hepatic transaminase levels can become elevated and should be measured periodically. is contraindicated in patients taking azathioprine or mercaptopurine because it can decrease metabolism of these drugs and thus potentiate their immunosuppressive and cytolytic effects. Hepatic transaminase levels can become elevated and should be measured periodically.
FebuxostatFebuxostat is a more costly (in the US) but potent xanthine oxidase inhibitor of urate synthesis. It is especially useful in patients who do not tolerate allopurinol, who have contraindications to allopurinol, or in whom allopurinol does not sufficiently decrease urate levels. is a more costly (in the US) but potent xanthine oxidase inhibitor of urate synthesis. It is especially useful in patients who do not tolerate allopurinol, who have contraindications to allopurinol, or in whom allopurinol does not sufficiently decrease urate levels.Febuxostat appears to prevent acute flares as efficaciously as allopurinol (3). Febuxostat is begun at 40 mg orally once a day and increased to 80 to 120 mg orally once a day if urate does not decrease to < 6 mg/dL (< 0.35 mmol/L). Febuxostat (like allopurinol) is contraindicated in patients taking azathioprine or mercaptopurine because it can decrease metabolism of these drugs. Compared with ) is contraindicated in patients taking azathioprine or mercaptopurine because it can decrease metabolism of these drugs. Compared withallopurinol, febuxostat increased the risk of mortality in one study of patients with known cardiovascular disease (4), but several additional studies have not confirmed this observation (5). Transaminase levels can become elevated and should be measured periodically.
PegloticasePegloticase is a pegylated form of recombinant uricase. Uricase is an enzyme, absent in humans, that converts urate to allantoin, which is more soluble. Pegloticase is expensive and is used primarily in patients with gout in whom other treatments have been unsuccessful in lowering the serum urate level. Pegloticase can also be used in patients who have a high burden of tophaceous deposits that would not likely be dissolved in a reasonable time period by other urate-lowering therapies. It is given IV every 2 to 3 weeks for many months (typically at least 6 to 9 months) to totally deplete the excess urate deposits; it often lowers the serum urate level to < 1 mg/dL (< 0.1 mmol/L). Pegloticase is contraindicated in patients with G6PD deficiency because it can cause hemolysis and methemoglobinemia. Pegloticase infusion can be associated with symptoms consistent with anaphylaxis. The effectiveness of the currently available preparation is limited by a high rate of development of drug neutralizing antibodies. Failure of urate levels to decrease to < 6 mg/dL (< 0.35 mmol/L) after a pegloticase infusion indicates the likely presence of antipolyethylene glycol (anti-PEG) antibodies and an increased risk of future allergic reactions; regular infusions are then stopped. To prevent other urate-lowering drugs from masking ineffectiveness of pegloticase, other urate-lowering drugs should not be used together with pegloticase. However, co-administration of immunosuppressants (eg, methotrexate) with . However, co-administration of immunosuppressants (eg, methotrexate) withpegloticase may prevent development of the neutralizing antibodies.
Uricosuric therapy is useful in patients who under excrete uric acid (the majority of patients with hyperuricemia), have normal renal function, and have not had renal stones. Probenecid is the only uricosuric drug available in the US. is useful in patients who under excrete uric acid (the majority of patients with hyperuricemia), have normal renal function, and have not had renal stones. Probenecid is the only uricosuric drug available in the US.
Probenecid can be used as monotherapy if both allopurinol and febuxostat are contraindicated or not tolerated. Probenecid can be used as monotherapy if both allopurinol and febuxostat are contraindicated or not tolerated.Probenecid loses efficacy with declining renal function and is generally not as useful with a glomerular filtration rate < 50 mL/min/1.73 m2. Probenecid treatment begins with 250 mg orally 2 times a day, with doses increased as needed, to a maximum of 1 g orally 3 times a day. It is also effective when added to a xanthine oxidase inhibitor.
The antihypertensive drug losartan and the triglyceride-lowering drug fenofibrate both have uricosuric effects and can be used to decrease uric acid in patients who have other reasons for taking these drugs. Low doses of salicylates may decrease uric acid excretion and worsen hyperuricemia, but only trivially, and should The antihypertensive drug losartan and the triglyceride-lowering drug fenofibrate both have uricosuric effects and can be used to decrease uric acid in patients who have other reasons for taking these drugs. Low doses of salicylates may decrease uric acid excretion and worsen hyperuricemia, but only trivially, and shouldnot be avoided if otherwise indicated as in secondary prevention of cardiovascular disease.
Other treatments
Fluid intake ≥ 3 L per day is desirable for all patients, especially those who chronically pass urate gravel or stones.
Alkalinization of urine (with potassium citrate 20 to 40 mEq orally 2 times a day or acetazolamide 500 mg orally at bedtime) is also occasionally effective for patients with persistent uric acid urolithiasis despite hypouricemic therapy and adequate hydration. However, excessive urine alkalinization may cause deposition of calcium phosphate and oxalate crystals.Alkalinization of urine (with potassium citrate 20 to 40 mEq orally 2 times a day or acetazolamide 500 mg orally at bedtime) is also occasionally effective for patients with persistent uric acid urolithiasis despite hypouricemic therapy and adequate hydration. However, excessive urine alkalinization may cause deposition of calcium phosphate and oxalate crystals.
Extracorporeal shock wave lithotripsy may be needed to disintegrate renal stones.
Large tophi in areas with healthy skin may be removed surgically; all others should slowly resolve under adequate hypouricemic therapy.
Treatment references
1. Stamp LK, Frampton C, Morillon MB, et al: Association between serum urate and flares in people with gout and evidence for surrogate status: a secondary analysis of two randomised controlled trials. Lancet Rheumatol 4: e53-e60, 2022. doi.org/10.1016/S2665-9913(21)00319-2
2. Jutkowitz E, Dubreuil M, Lu N, et al: The cost-effectiveness of HLA-B*5801 screening to guide initial urate-lowering therapy for gout in the United States. Semin Arth Rheum 46:594-600, 2017. doi: 10.1016/j.semarthrit.2016.10.009
3. O'Dell JR, Brophy MT, Pillinger MH, et al: Comparative effectiveness of allopurinol and febuxostat in gout management. NEJM Evid 1(3):10.1056/evidoa2100028, 2022. doi: 10.1056/evidoa2100028. Epub 2022 Feb 3. PMID: 35434725; PMCID: PMC9012032.
4. White WR, Saag KG, Becker MA, et al: Cardiovascular safety of febuxostat or allopurinol in patients with gout. : Cardiovascular safety of febuxostat or allopurinol in patients with gout.N Engl J Med 378:1200-1210, 2018. doi: 10.1056/NEJMoa1710895
5. Mackenzie IS, Ford I, Nuki G, et al: Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): a multicentre, prospective, randomised, open-label, non-inferiority trial. Lancet 396(10264):1745-1757, 2020. doi: 10.1016/S0140-6736(20)32234-0
Key Points
Although increased purine intake and increased production can contribute to hyperuricemia, the most common cause of gout is decreased urate excretion secondary to kidney disorders or genetic variability in uric acid transporter efficiency.
Suspect gout in patients with sudden, unexplained acute monoarticular or oligoarticular arthritis, particularly if the great toe or midfoot is affected or there is a prior history of sudden, unexplained episodes of acute arthritis with spontaneous remission in 7 to 10 days.
Confirm the diagnosis by finding needle-shaped, strongly negatively birefringent urate crystals in joint fluid; or by dual-energy CT scans or ultrasound imaging. Documentation of hyperuricemia is insufficient to confirm the diagnosis of gouty arthritis.
Treat acute flares of gout with oral colchicine, an NSAID, a corticosteroid, a combination of colchicine with an NSAID or a corticosteroid, or an interleukin-1 (IL-1) antagonist. Treat acute flares of gout with oral colchicine, an NSAID, a corticosteroid, a combination of colchicine with an NSAID or a corticosteroid, or an interleukin-1 (IL-1) antagonist.
Decrease the risk of future flares by prescribing colchicine, an NSAID, and life-long use of drugs to decrease the serum urate level.Decrease the risk of future flares by prescribing colchicine, an NSAID, and life-long use of drugs to decrease the serum urate level.
Give drugs that decrease serum urate levels if patients have tophi, > 2 flares of gout per year, urolithiasis, or multiple comorbidities that contraindicate the drugs used to relieve acute flares; individualize the use of urate-lowering ongoing therapy in other patients.
Decrease urate levels usually by prescribing allopurinol or febuxostat alone or in combination with a uricosuric drug.Decrease urate levels usually by prescribing allopurinol or febuxostat alone or in combination with a uricosuric drug.
Asymptomatic Hyperuricemia
Asymptomatic hyperuricemia is elevation of serum urate > 7 mg/dL (> 0.4 mmol/L) in the absence of clinical gout.
Generally, treatment of asymptomatic hyperuricemia is not required. Most patients with asymptomatic hyperuricemia with serum urate levels as high as 10 mg/dL (0.6 mmol/L) do not develop gout flares over 10 years. However, patients with overexcretion of urate and recurrent uric acid kidney stones despite urinary alkalinization and sufficient hydration may receive allopurinol. Generally, treatment of asymptomatic hyperuricemia is not required. Most patients with asymptomatic hyperuricemia with serum urate levels as high as 10 mg/dL (0.6 mmol/L) do not develop gout flares over 10 years. However, patients with overexcretion of urate and recurrent uric acid kidney stones despite urinary alkalinization and sufficient hydration may receive allopurinol.
Observational data suggested that hyperuricemia may contribute to the progression of chronic kidney disease, cardiovascular disease, and, in adolescents, primary hypertension. Interventional studies, however, have not demonstrated that lowering the serum urate level reduces progression of renal disease.







