


Acute infectious (septic) arthritis is a joint infection that evolves over hours or days. The infection resides in synovial or periarticular tissues and is usually bacterial. Septic arthritis can rapidly destroy joint structures. Symptoms include rapid onset of pain, effusion, and restriction of both active and passive range of motion, usually within a single joint. Diagnosis requires synovial fluid analysis and culture. Treatment is IV antibiotics, and surgical drainage of infection from joints is typically required.
")

Acute infectious arthritis is most common in older adults but may occur in children. Approximately 50% of children with joint infection are < 3 years of age. Routine childhood vaccination for Haemophilus influenzae and Streptococcus pneumoniae is decreasing the incidence of joint infection in this age group (1, 2).
General references
1. Howard AW, Viskontas D, Sabbagh C. Reduction in osteomyelitis and septic arthritis related to Haemophilus influenzae type B vaccination. J Pediatr Orthop. 1999;19(6):705-709.
2. Olarte L, Romero J, Barson W, et al. Osteoarticular Infections Caused by Streptococcus pneumoniae in Children in the Post-Pneumococcal Conjugate Vaccine Era. Pediatr Infect Dis J. 2017;36(12):1201-1204. doi:10.1097/INF.0000000000001697
Risk factors
There are many risk factors for acute joint infection (see table Risk Factors for Infectious Arthritis).
Risk of infectious arthritis is substantially increased in patients with rheumatoid arthritis and other disorders causing chronic joint damage, a past history of joint infection, injection drug use, or a prosthetic joint (see also Prosthetic Joint Infectious Arthritis). Patients with rheumatoid arthritis are at higher risk of bacterial arthritis than the general population (1, 2). Most children who develop infectious arthritis do not have identified risk factors (3, 4).
Risk Factors for Infectious Arthritis
Older age (50% of adults are > 60 years) |
Arthrocentesis (very small risk), joint injection, or joint surgery |
Cancer |
Chronic medical illness (eg, lung or liver disease) |
History of previous joint infection |
Immunodeficiency, including HIV |
Immunosuppressive therapy, including corticosteroids |
Injection drug use |
Rheumatoid arthritis and other forms of inflammatory arthritis |
Risk factors for sexually transmitted infections (eg, multiple sex partners, absence of barrier precautions) |
Skin infections |
See also Elsissy JG, Liu JN, Wilton PJ, Nwachuku I, Gowd AK, Amin NH. Bacterial Septic Arthritis of the Adult Native Knee Joint: A Review. JBJS Rev. 2020;8(1):e0059. doi:10.2106/JBJS.RVW.19.00059 |
Risk factors references
1. Gardner GC, Weisman MH. Pyarthrosis in patients with rheumatoid arthritis: a report of 13 cases and a review of the literature from the past 40 years. Am J Med. 1990;88(5):503-511. doi:10.1016/0002-9343(90)90430-l
2. Favero M, Schiavon F, Riato L, Carraro V, Punzi L. Rheumatoid arthritis is the major risk factor for septic arthritis in rheumatological settings. Autoimmun Rev. 2008;8(1):59-61. doi:10.1016/j.autrev.2008.07.018
3. Woods CR, Bradley JS, Chatterjee A, et al. Clinical Practice Guideline by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA): 2023 Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics [published correction appears in J Pediatric Infect Dis Soc. 2024 Aug 24;13(8):443. doi: 10.1093/jpids/piae065]. J Pediatric Infect Dis Soc. 2024;13(1):1-59. doi:10.1093/jpids/piad089
4. Chan BY, Crawford AM, Kobes PH, et al. Septic Arthritis: An Evidence-Based Review of Diagnosis and Image-Guided Aspiration. AJR Am J Roentgenol. 2020;215(3):568-581. doi:10.2214/AJR.20.22773
Etiology of Acute Infectious Arthritis
Infectious organisms reach joints by (1)
Direct penetration (eg, trauma, surgery, arthrocentesis, bites)
Extension from an adjacent infection (eg, osteomyelitis, a soft-tissue abscess, an infected wound)
Hematogenous spread from a remote site of infection
Common organisms are listed in table Organisms That Commonly Cause Acute Infectious Arthritis.
Organisms That Commonly Cause Acute Infectious Arthritis
Patient Group | Organism | Typical Sources |
|---|---|---|
Adults and adolescents | Staphylococcus aureus, beta-hemolytic streptococci, pneumococci, gonococci (in young adults of reproductive age), and rarely Neisseria meningitidis | Bacteremia (for staphylococci, streptococci, and pneumococci); cervical, urethral, rectal, or pharyngeal infection with bacteremic dissemination (for gonococci) |
Neonates | Group B streptococci, Escherichia coli (and other gram-negative enteric bacteria), S. aureus | Maternal-fetal transmission IV punctures or catheters with bacteremic dissemination |
Children ≤ 3 years | Streptococcus pyogenes, Streptococcus pneumoniae, S. aureus, Kingella kingae | Bacteremia (eg, otitis media, upper respiratory infections, skin infections, meningitis) |
Age 3 years to adolescence | S. aureus, streptococci, Neisseria gonorrhoeae, Pseudomonas aeruginosa, Kingella kingae | Bacteremia or contiguous spread |
Children with meningitis, bacteremia, or palpable purpura | N. meningitidis (uncommon) | |
All ages | Viruses (eg, parvovirus B19, hepatitis B, or hepatitis C virus, rubella virus [active infection and after immunization], togavirus, chikungunya virus, varicella virus, mumps virus [in adults], adenovirus, coxsackieviruses [A9, B2, B3, B4, and B6], retroviruses [including HIV], Epstein-Barr virus) | Viremia or immune complex deposition |
Patients with possible tick exposure | Borrelia burgdorferi (causing Lyme disease) | |
Patients with bite wounds (human, dog or cat, rat) | Often polymicrobial Human: Eikenella corrodens, group B streptococci, S. aureus, oral anaerobes (eg, Fusobacterium sp, peptostreptococci, Bacteroides sp) Dog or cat: S. aureus, Pasteurella multocida, Pseudomonas sp, Moraxella sp, Haemophilus sp Rat: S. aureus, Streptobacillus moniliformis, Spirillum minus | Direct joint penetration, usually of the small joints of the hands (See also Infected Bite Wounds of the Hand.) |
Older adults Patients with severe joint trauma or serious disease (eg, immunosuppression, hemodialysis, systemic lupus erythematosus, rheumatoid arthritis, diabetes, cancer) | Staphylococci (particularly in rheumatoid arthritis), gram-negative bacteria (eg, Enterobacter, P. aeruginosa, Serratia marcescens), Salmonella sp (particularly in systemic lupus erythematosus*) | Urinary tract, skin |
Patients with polyarticular infections | Streptococci, S. aureus | Pharyngitis, cellulitis, endocarditis, gastrointestinal and genitourinary infections |
Patients with joint penetration (caused by injury, arthrocentesis, or arthrotomy), contiguous infection, diabetes, or cancer | Streptococci, S. aureus Anaerobes (eg, Cutibacterium acnes, Peptostreptococcus magnus, Fusobacterium sp, Clostridium sp, Bacteroides sp); often as mixed infections with facultative or aerobic bacteria such as S. aureus, Staphylococcus epidermidis, E. coli | Skin, abdomen, genitals, odontogenic infections, sinuses, ischemic limbs, decubitus ulcers |
HIV-infected patients | S. aureus, streptococci, Salmonella sp, mycobacteria | Skin, mucous membranes, catheters |
Injection drug use, indwelling vascular catheters (eg, for hemodialysis, apheresis, chemotherapy, or parenteral nutrition) | Gram-negative bacteria, S. aureus, streptococci, Candida sp | Bacteremia, fungemia |
* Signs of inflammation can be blunted, so physicians need to have a lower threshold for aspiration and culture; some chronic conditions (eg, immunosuppression, hemodialysis, systemic lupus erythematosus, rheumatoid arthritis, diabetes, cancer) may increase risk of unusual infections (eg, fungal, mycobacterial). | ||
sp = species. | ||
In adults, most acute joint infections result from bacteria and are classified as gonococcal or nongonococcal. This distinction is important because gonococcal infections are far less destructive to the joint. In adults overall, Staphylococcus aureus tends to be the most frequent cause of infectious arthritis. Methicillin resistance is common among community isolates of S. aureus. S. aureus is associated with the largest risk of long-term complications (2).
Neisseria gonorrhoeae only accounts for slightly over 1% of septic arthritis cases, but it should be considered in sexually active adults (3). It results when N. gonorrhoeae spreads from a sometimes asymptomatic infection from mucosal surfaces (cervix, urethra, rectum, pharynx) via the bloodstream. Affected patients often have simultaneous genital infections with Chlamydia trachomatis. Streptococcus species are also frequent causes, particularly in patients with polyarticular infections. Patients receiving immunosuppressive therapy (eg, with tumor necrosis factor inhibitors or corticosteroids) may have septic arthritis from less common pathogens (eg, mycobacteria, fungi), and recognition is often delayed due to a blunted inflammatory response (4, 5).
Kingella kingae has emerged as a major cause of septic arthritis in young children (6, 7).
Etiology references
1. Mathews CJ, Weston VC, Jones A, Field M, Coakley G. Bacterial septic arthritis in adults. Lancet. 2010;375(9717):846-855. doi:10.1016/S0140-6736(09)61595-6
2. Maneiro JR, Souto A, Cervantes EC, Mera A, Carmona L, Gomez-Reino JJ. Predictors of treatment failure and mortality in native septic arthritis. Clin Rheumatol. 2015;34(11):1961-1967. doi:10.1007/s10067-014-2844-3
3. Ross JJ: Septic arthritis of native joints. Infect Dis Clin North Am. 31(2): 203−218, 2017. Epub 2017 Mar 30. doi: 10.1016/j.idc.2017.01.001
4. Kim HW, Han M, Jung I, Ahn SS. Incidence of septic arthritis in patients with ankylosing spondylitis and seropositive rheumatoid arthritis following TNF inhibitor therapy. Rheumatology (Oxford). 2023;62(8):2740-2747. doi:10.1093/rheumatology/keac721
5. Galloway JB, Hyrich KL, Mercer LK, et al. Risk of septic arthritis in patients with rheumatoid arthritis and the effect of anti-TNF therapy: results from the British Society for Rheumatology Biologics Register. Ann Rheum Dis. 2011;70(10):1810-1814. doi:10.1136/ard.2011.152769
6. Gouveia C, Duarte M, Norte S, et al. Kingella kingae Displaced S. aureus as the Most Common Cause of Acute Septic Arthritis in Children of All Ages. Pediatr Infect Dis J. 2021;40(7):623-627. doi:10.1097/INF.0000000000003105
7. Yagupsky P. Use of blood culture vials and nucleic acid amplification for the diagnosis of pediatric septic arthritis. Clin Infect Dis. 2008;46(10):1631-1632. doi:10.1086/587754
Pathophysiology of Acute Infectious Arthritis
Infecting organisms multiply in the synovial fluid and synovial lining (1). Some bacteria (eg, S. aureus) produce virulence factors (adhesins), which allow bacteria to penetrate, remain within, and infect joint tissues. Other bacterial products (eg, endotoxin from gram-negative organisms, cell wall fragments, exotoxins from gram-positive organisms, immune complexes formed by bacterial antigens and host antibodies) augment the inflammatory reaction.
Neutrophils migrate into the joint and phagocytose the infecting organisms. Phagocytosis of bacteria also results in neutrophil autolysis with release of lysosomal enzymes into the joint, which damages synovia, ligaments, and cartilage. Therefore, neutrophils are both the major host defense system and the cause of joint damage. Articular cartilage can be destroyed within hours or days.
Inflammatory synovitis may occasionally persist even after the infection has been eradicated by antibiotics. Particularly in gonococcal cases, persistent antigen debris from bacteria or infection may alter cartilage, causing it to become antigenic, and—together with the adjuvant effects of bacterial components and immune complexes—immune-mediated, “sterile,” chronic inflammatory synovitis may develop.
Pathophysiology reference
1. Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002;15(4):527-544. doi:10.1128/CMR.15.4.527-544.2002
Symptoms and Signs of Acute Infectious Arthritis
Over a few hours to a few days, patients with an acute joint infection develop moderate to severe joint pain, warmth, tenderness, effusion, restricted active and passive motion, and sometimes erythema (1). A single joint is typically affected. Polyarticular septic arthritis is more likely to occur in patients with a systemic rheumatic disease (2,3). Many, but not all, patients with acute infectious arthritis are febrile. Occasionally, systemic symptoms may be minimal or absent, although signs of sepsis may be present in patients who have bacteremia, particularly with a virulent pathogen such as S. aureus, beta-hemolytic streptococci, or gram-negative bacilli.
Infants and children may present with limited spontaneous movement of a limb (pseudoparalysis), irritability, feeding disturbances. They may also present with a high or low-grade fever. Sometimes the patient may be afebrile (4).
Gonococcal arthritis
Gonococcal arthritis can cause a distinctive dermatitis-polyarthritis-tenosynovitis syndrome.
Classic manifestations are (5)
Fever (for 5 to 7 days)
Multiple skin lesions (petechiae, papules, pustules, hemorrhagic vesicles or bullae, necrotic lesions) on mucosal surfaces and on the skin of the trunk, hands, or lower extremities; however, genital lesions are often absent
Absence of genital symptoms
Migratory arthralgias, arthritis, and tenosynovitis (often involves multiple tendons), most often in the small joints of the hands, wrists, elbows, knees, and ankles, and rarely the axial skeletal joints
Monarthritis or oligoarthritis affecting a knee, ankles, wrists, or elbows (5)


Image courtesy of Dr. S. E. Thompson and J. Pledger via the Public Health Image Library of the Centers for Disease Control and Prevention.
Symptoms of the original mucosal infection (eg, urethritis, cervicitis) may not be present.
Nongonococcal bacterial arthritis
Nongonococcal bacterial arthritis causes progressive moderate to severe joint pain that is markedly worsened by movement or palpation (1). Most infected joints are swollen, erythematous, and warm. Fever is present in most, but not all, cases. Virulent organisms (eg, S. aureus, Pseudomonas aeruginosa) generally cause a more fulminant arthritis, whereas less virulent organisms (eg, coagulase-negative staphylococci, Propionibacterium acnes) cause a less fulminant arthritis.
In 80% of adults, nongonococcal bacterial arthritis is monoarticular and usually occurs in a peripheral joint: knee, hip, shoulder, wrist, ankle, or elbow. In children, ≥ 90% of cases are monoarticular, mostly involving the knee, hip, and ankle (6).
Polyarticular involvement is somewhat more common among patients who are immunosuppressed, who have an underlying chronic arthritis (eg, rheumatoid arthritis, osteoarthritis), or who have a streptococcal or staphylococcal infection (especially beta-hemolytic streptococcus or S. aureus). In people who use injection drugs and patients with indwelling vascular catheters, axial joints (eg, sternoclavicular, costochondral, hip, shoulder, vertebral, symphysis pubis, sacroiliac) are often involved (7). H. influenza may cause a dermatitis-arthritis syndrome similar to gonococcal infection.
Infectious arthritis secondary to bite wounds
Infection due to human, dog, or cat bites (see Human and Mammal Bites) usually develops within 48 hours. Interpretation of the physical examination is often complicated by the presence of traumatic injury as well as infection.
Rat bites cause systemic symptoms such as fever, rash, and joint pain or true arthritis with regional adenopathy within approximately 2 to 10 days (8).
Viral infectious arthritis
Viral infectious arthritis sometimes causes symptoms similar to acute nongonococcal bacterial arthritis and is more likely to be polyarticular than bacterial arthritis (9).
Borrelia burgdorferi arthritis
Patients with B. burgdorferi arthritis may have other symptoms of Lyme disease or present only with acute monarthritis or oligoarthritis, which, if untreated, may resolve spontaneously after a few weeks to months but then recur (10). Lyme arthritis most often involves the knee and large joints and typically presents without fever. Chronic pain that remains after appropriate antibiotic therapy is likely to be of noninfectious etiology.
A polyarticular rheumatoid arthritis–like syndrome is distinctly unusual and more likely to be from another diagnosis.
Symptoms and signs references
1. Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis?. JAMA. 2007;297(13):1478-1488. doi:10.1001/jama.297.13.1478
2. Dubost JJ, Fis I, Denis P, et al. Polyarticular septic arthritis. Medicine (Baltimore). 1993;72(5):296-310. doi:10.1097/00005792-199309000-00002
3. Lieber SB, Fowler ML, Zhu C, Moore A, Shmerling RH, Paz Z. Clinical characteristics and outcomes in polyarticular septic arthritis. Joint Bone Spine. 2018;85(4):469-473. doi:10.1016/j.jbspin.2017.09.00
4. Woods CR, Bradley JS, Chatterjee A, et al. Clinical Practice Guideline by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA): 2023 Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics [published correction appears in J Pediatric Infect Dis Soc. 2024 Aug 24;13(8):443. doi: 10.1093/jpids/piae065]. J Pediatric Infect Dis Soc. 2024;13(1):1-59. doi:10.1093/jpids/piad089
5. Moussiegt A, François C, Belmonte O, et al. Gonococcal arthritis: case series of 58 hospital cases. Clin Rheumatol. 2022;41(9):2855-2862. doi:10.1007/s10067-022-06208-w
6. Okubo Y, Nochioka K, Marcia T. Nationwide survey of pediatric septic arthritis in the United States. J Orthop. 2017;14(3):342-346. Published 2017 Jun 23. doi:10.1016/j.jor.2017.06.004
7. Ross JJ, Ard KL, Carlile N. Septic Arthritis and the Opioid Epidemic: 1465 Cases of Culture-Positive Native Joint Septic Arthritis From 1990-2018. Open Forum Infect Dis. 2020;7(3):ofaa089. Published 2020 Mar 12. doi:10.1093/ofid/ofaa089
8. Elliott SP. Rat bite fever and Streptobacillus moniliformis. Clin Microbiol Rev. 2007;20(1):13-22. doi:10.1128/CMR.00016-06
9. Calabrese LH, Naides SJ. Viral arthritis. Infect Dis Clin North Am. 2005;19(4):963-x. doi:10.1016/j.idc.2005.09.002
10. Bockenstedt LK, Wormser GP. Review: unraveling Lyme disease. Arthritis Rheumatol. 2014;66(9):2313-2323. doi:10.1002/art.38756
Diagnosis of Acute Infectious Arthritis
Arthrocentesis with synovial fluid examination and culture
Blood culture
Usually complete blood count and erythrocyte sedimentation rate (and/or C-reactive protein)
Molecular testing (eg, polymerase chain reaction)
Sometimes imaging studies
Infectious arthritis is suspected in patients with acute monoarticular or oligoarticular arthritis and in patients with other combinations of symptoms characteristic of particular infectious arthritis syndromes (eg, migratory polyarthritis, tenosynovitis, and skin lesions typical of disseminated gonococcal infection; erythema migrans or other symptoms and signs of Lyme disease).
Even mild monoarticular or oligoarticular joint symptoms should arouse suspicion in patients taking immunosuppressive therapy (eg, corticosteroids, tumor necrosis factor or interleukin-6 inhibitors) with risk factors (eg, rheumatoid arthritis), a prosthetic joint, or an extra-articular infection capable of spreading to a joint (eg, genital gonococcal infection, pneumonia, bacteremia, any anaerobic infection).
Pearls & Pitfalls
|
Infectious arthritis
Synovial fluid examination is the cornerstone of diagnosis of acute joint infection (1). Fluid is examined grossly and sent for cell count and differential, Gram stain, aerobic and anaerobic culture, and crystal analysis. Foul-smelling synovial fluid suggests anaerobic infection. Fluid from an acutely infected joint usually reveals a white blood cell (WBC) count > 50,000 cells/mcL (50 × 109/L) (sometimes > 100,000 cells/mcL [100 × 109/L ]) consisting of > 95% polymorphonuclear leukocytes (2). WBC counts tend to be higher in nongonococcal bacterial than in gonococcal infectious arthritis. WBC counts may also be lower in early or partially treated infections; therefore, a white cell count < 50,000 cells/mcL does not exclude infectious arthritis (3,4).
Gram stain reveals organisms in only 50 to 75% of joints with acute bacterial arthritis, most often staphylococci. A positive Gram stain is suggestive (5), but false positive results occur. Cultures are definitive, but are limited in the presence of prior antibiotic use (6).
Inoculation of synovial fluid into aerobic blood culture bottles can improve detection of Kingella kingae (7).
The presence of crystals does not exclude coexisting infectious arthritis. Initial synovial fluid analysis cannot differentiate between infectious and other inflammatory synovial fluid (8). There is significant overlap between the synovial cell counts in fluids from patients with gout, calcium pyrophosphate crystal–associated arthritis, and infection. If differentiation is impossible by clinical means or synovial fluid examination, infectious arthritis should be assumed and treated, pending culture results.
Blood tests, such as blood cultures, complete blood count, and erythrocyte sedimentation rate (or C-reactive protein), are usually obtained. However, normal results do not exclude infection. WBC count, erythrocyte sedimentation rate, or C-reactive protein may be increased in noninfectious joint inflammation (including gout) as well as infectious joint inflammation (4). The serum urate level should not be used to diagnose or exclude gout as the cause of the arthritis, because the level can be normal or even low in gout, and may be high, although unrelated to gout, in patients with an acute bacterial infection (8).
Molecular testing (eg, polymerase chain reaction) may be used to directly detect organisms in clinical specimens. Gonococci may be detected outside of the infected joint with nucleic acid amplification testing (NAAT) of specimens from the cervix, urethra, oropharynx, or rectum (9). The approach to diagnosing gonococcal arthritis is discussed in more detail below. Some difficult-to-cultivate organisms, such as Mycobacterium tuberculosis and Tropheryma whipplei, may be directly detected in synovial fluid using polymerase chain reaction (PCR). Metagenomic next-generation sequencing (mNGS) may also be used as a tool for pathogen identification in difficult cases. mNGS has higher sensitivity compared with microbial culture and may be a useful diagnostic tool to test for pathogens in patients treated with antibiotics (10).
Radiographs of the involved joint are not diagnostic of acute infection but can exclude other conditions sometimes under consideration (eg, fractures). Abnormalities in early acute bacterial arthritis are limited to soft-tissue swelling and signs of synovial effusions (11). After 10 to 14 days of untreated bacterial infection, destructive changes of joint space narrowing (reflecting cartilage destruction) and erosions or foci of subchondral osteomyelitis may appear. Gas visible within the joints suggests infection with Escherichia coli or anaerobes.

© Springer Science+Business Media
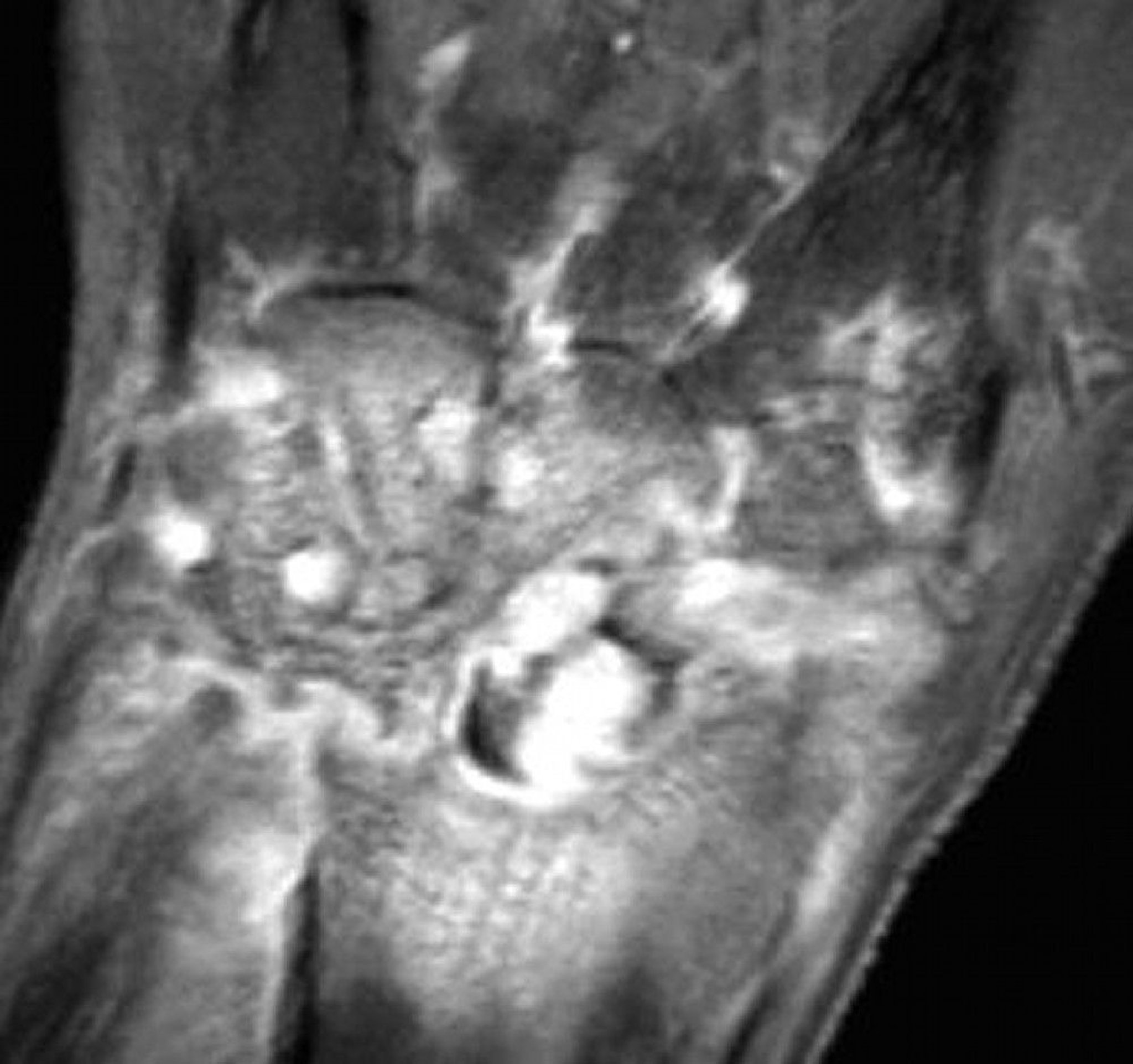
MRI is considered if the joint is not easily accessible for examination and aspiration (eg, an axial joint). MRI or ultrasound can identify sites of effusion or abscess that can be aspirated or drained for both diagnosis and therapy (12). MRI can provide early suggestion of associated osteomyelitis (13). Bone scans using technetium-99m can be falsely negative in infectious arthritis. Also, because they show increased uptake with increased blood flow in inflamed synovial membranes and in metabolically active bone, they can be falsely positive in noninfectious inflammatory arthritis such as gout. Nuclear imaging and MRI do not distinguish infection from crystal-induced arthritis (11).
Gonococcal arthritis
If gonococcal arthritis is suspected, blood and synovial fluid samples should be immediately plated on nonselective chocolate agar. Specimens should also be collected from the urethra, endocervix, rectum, and pharynx and be plated on selective Thayer-Martin medium. Genital, rectal, and oral cultures or NAAT testing is also recommended. Blood cultures may be positive during the first week and may assist in microbiologic diagnosis.
Synovial fluid cultures from joints with frank purulent arthritis may be positive, and fluid from skin lesions may also be positive. PCR testing from the synovial fluid should be completed because PCR may be positive in patients whose synovial fluid cultures are negative (9). If disseminated gonococcal infection is suspected based on clinical criteria, it is assumed to be present even if all gonococcal cultures are negative. Clinical response to antibiotics (anticipated within 5 to 7 days) can strongly support the diagnosis of gonorrhea.
Diagnosis references
1. Woods CR, Bradley JS, Chatterjee A, et al. Clinical Practice Guideline by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA): 2023 Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics [published correction appears in J Pediatric Infect Dis Soc. 2024 Aug 24;13(8):443. doi: 10.1093/jpids/piae065]. J Pediatric Infect Dis Soc. 2024;13(1):1-59. doi:10.1093/jpids/piad089
2. Margaretten ME, Kohlwes J, Moore D, Bent S. Does this adult patient have septic arthritis?. JAMA. 2007;297(13):1478-1488. doi:10.1001/jama.297.13.1478
3. Pesante BD, Salimi M, Miller WL, Young HL, Jenkins TC, Parry JA. The Effect of Crystal Arthropathy on the Diagnostic Criteria of Native Septic Arthritis. J Am Acad Orthop Surg. 2024;32(12):570-575. doi:10.5435/JAAOS-D-23-00857
4. Eren TK, Aktekin CN. How reliable are the synovial cell count and blood parameters in the diagnosis of septic arthritis?. Jt Dis Relat Surg. 2023;34(3):724-730. Published 2023 Aug 21. doi:10.52312/jdrs.2023.1222
5. Weston VC, Jones AC, Bradbury N, Fawthrop F, Doherty M. Clinical features and outcome of septic arthritis in a single UK Health District 1982-1991. Ann Rheum Dis.
6. Puzzitiello RN, Lipson SE, Michaud RG Jr, et al. Effect of Antibiotic Administration Before Joint Aspiration on Synovial Fluid White Blood Cell Count in Native Joint Septic Arthritis. Open Forum Infect Dis. 2024;11(1):ofad600. Published 2024 Jan 11. doi:10.1093/ofid/ofad600
7. Yagupsky P, Press J. Use of the isolator 1.5 microbial tube for culture of synovial fluid from patients with septic arthritis. J Clin Microbiol.1997;35(9):2410-2412. doi:10.1128/jcm.35.9.2410-2412.1997
8. Tzanis P, Klavdianou K, Lazarini A, et al. Septic Arthritis Complicating a Gout Flare: Report of Two Cases and Review of the Literature. Mediterr J Rheumatol. 2022;33(1):75-80. Published 2022 Mar 31. doi:10.31138/mjr.33.1.75
9. Moussiegt A, François C, Belmonte O, et al. Gonococcal arthritis: case series of 58 hospital cases. Clin Rheumatol. 2022;41(9):2855-2862. doi:10.1007/s10067-022-06208-w
10. Huang ZD, Zhang ZJ, Yang B, et al. Pathogenic Detection by Metagenomic Next-Generation Sequencing in Osteoarticular Infections. Front Cell Infect Microbiol. 2020;10:471. Published 2020 Sep 17. doi:10.3389/fcimb.2020.00471
11. Greenspan A, Tehranzadeh J. Imaging of infectious arthritis. Radiol Clin North Am. 2001;39(2):267-276. doi:10.1016/s0033-8389(05)70277-3
12. Chan BY, Crawford AM, Kobes PH, et al. Septic Arthritis: An Evidence-Based Review of Diagnosis and Image-Guided Aspiration. AJR Am J Roentgenol. 2020;215(3):568-581. doi:10.2214/AJR.20.22773
13. Karchevsky M, Schweitzer ME, Morrison WB, Parellada JA. MRI findings of septic arthritis and associated osteomyelitis in adults. AJR Am J Roentgenol. 2004;182(1):119-122. doi:10.2214/ajr.182.1.1820119
Treatment of Acute Infectious Arthritis
IV antibiotics
Drainage of infected fluid from joint
Antibiotic therapy
Initial antibiotic selection is directed at the most likely pathogens (1). The regimen is adjusted based on the results of culture and susceptibility testing.
Gonococcal arthritis is treated with
Ceftriaxone 1 g IV once a dayCeftriaxone 1 g IV once a day
IV ceftriaxone is continued until at least 24 hours after symptoms and signs resolve, followed by cefixime 400 mg orally twice a day for 7 to 14 days if the organism is proved susceptible. If IV ceftriaxone is continued until at least 24 hours after symptoms and signs resolve, followed by cefixime 400 mg orally twice a day for 7 to 14 days if the organism is proved susceptible. IfChlamydia trachomatis infection has not been excluded, doxycycline 100 mg orally twice a day for 7 days should be added. Consult an infectious disease specialist if the patient does not improve on this regimen or cannot tolerate cephalosporins. In such cases, alternative regimens may include azithromycin plus either gemifloxacin or gentamicin. Ciprofloxacin 500 mg orally twice a day may be used only if the organism is isolated and proved susceptible (infection has not been excluded, doxycycline 100 mg orally twice a day for 7 days should be added. Consult an infectious disease specialist if the patient does not improve on this regimen or cannot tolerate cephalosporins. In such cases, alternative regimens may include azithromycin plus either gemifloxacin or gentamicin. Ciprofloxacin 500 mg orally twice a day may be used only if the organism is isolated and proved susceptible (2).
If nongonococcal gram-positive infection is suspected by Gram stain in an adult, or if no organisms are seen, initial treatment is with
Vancomycin 1 g IV every 12 hoursVancomycin 1 g IV every 12 hours
Because methicillin resistance is common in community-acquired S. aureus, for patients with gram-positive cocci in clusters on Gram stain or a negative Gram stain when S. aureus is suspected, vancomycin is the empiric drug of choice. Options for patients with gram-positive cocci in clusters on Gram stain with methicillin-sensitive is suspected, vancomycin is the empiric drug of choice. Options for patients with gram-positive cocci in clusters on Gram stain with methicillin-sensitiveS. aureus include a semisynthetic penicillin (eg, nafcillin 2 g IV every 4 hours) or a cephalosporin (eg, cefazolin 2 g IV every 8 hours) (include a semisynthetic penicillin (eg, nafcillin 2 g IV every 4 hours) or a cephalosporin (eg, cefazolin 2 g IV every 8 hours) (3).
If gram-negative infection is suspected (eg, in patients with immunosuppression or serious comorbid disorders, injection drug use, a recent infection with antibiotic use, or an indwelling vascular catheter), empiric treatment includes a parenteral antibiotic with antipseudomonal activity (eg, ceftazidime 2 g IV every 8 hours; cefepime 2 g every 8 hours; piperacillin/tazobactam 4.5 g every 6 hours) (is suspected (eg, in patients with immunosuppression or serious comorbid disorders, injection drug use, a recent infection with antibiotic use, or an indwelling vascular catheter), empiric treatment includes a parenteral antibiotic with antipseudomonal activity (eg, ceftazidime 2 g IV every 8 hours; cefepime 2 g every 8 hours; piperacillin/tazobactam 4.5 g every 6 hours) (3).
Neonates should be treated initially with an antibiotic that covers gram-positive infection, (eg, nafcillin or vancomycin forshould be treated initially with an antibiotic that covers gram-positive infection, (eg, nafcillin or vancomycin forS. aureus infection) plus an antibiotic that covers gram-negative infection (eg, gentamicin or a third-generation cephalosporin such as cefotaxime for infection) plus an antibiotic that covers gram-negative infection (eg, gentamicin or a third-generation cephalosporin such as cefotaxime forK. kingae infection) (1).
Children > 48 months of age should be treated with empiric therapy to cover S. aureus. The need for coverage against community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is based on local susceptibility data (1).
Parenteral antibiotics are continued until clinical improvement is clear, and oral antibiotics should be given at high doses for another 2 to 4 weeks according to the clinical response. Children with rapid clinical improvement with no evidence of osteomyelitis may be treated with a course of therapy as short as 10-14 days. For those with a slower clinical response, inadequate source control, or ongoing signs of infection (eg, elevated C-reactive protein) a 21-28 day course of therapy is preferred (1).
Infections caused by streptococci and Haemophilus are usually eradicated after 2 weeks of oral antibiotics after IV treatment.
Staphylococcal infections and other routine bacterial pathogens are treated with antibiotics for at least 3 weeks and often 4 weeks or longer, especially in patients with prior arthritis in the affected joint, with immunosuppression, or whose diagnosis was delayed.
Drainage of infected fluid
In addition to antibiotics, acute nongonococcal bacterial arthritis requires large-bore needle aspiration of intra-articular fluid at least once a day, or tidal irrigation lavage, arthroscopic lavage, or arthrotomy for debridement. Patients with rheumatoid arthritis receiving immunosuppressive therapy or those with a delayed diagnosis should generally undergo early and aggressive surgical debridement and drainage. Arthroscopic wash out and open arthrotomy are commonly used as surgical interventions with similar efficacy. Arthroscopy seems to be preferable because it has a lower all-cause complication rate (4, 5).
For gonococcal arthritis with persistent effusion, infected fluid is aspirated and drainage may need to be repeated as necessary.
Acute bacterial arthritis requires joint splinting for the first few days to reduce pain, followed by passive and active range-of-motion exercises to limit contractures, with muscle strengthening as soon as it can be tolerated. nonsteroidal anti-inflammatory drugs (NSAIDs) can help decrease pain and inflammation once a diagnosis is confirmed (5). Intra-articular corticosteroids should be avoided during the acute infection. Because bacteriologic tests may be falsely negative, potent anti-inflammatory therapy should generally be avoided until a bacterial source has been definitively excluded. Opioids can be used for pain control.
Treatment references
1. Woods CR, Bradley JS, Chatterjee A, et al. Clinical Practice Guideline by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA): 2023 Guideline on Diagnosis and Management of Acute Bacterial Arthritis in Pediatrics [published correction appears in J Pediatric Infect Dis Soc. 2024 Aug 24;13(8):443. doi: 10.1093/jpids/piae065]. J Pediatric Infect Dis Soc. 2024;13(1):1-59. doi:10.1093/jpids/piad089
2. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187. Published 2021 Jul 23. doi:10.15585/mmwr.rr7004a1
3. Ohl, CA. Infectious Arthritis of Native Joints. In: Bennett JE, Dolin R, Blaser, MJ. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. Elsevier; 2019:103.
4. McKenna DP, Miller P, McAleese T, Cleary M. Arthroscopy or arthrotomy for native knee septic arthritis: A systematic review. J Exp Orthop. 2024;11(3):e12041. Published 2024 Jun 6. doi:10.1002/jeo2.12041
5. Donatto KC. Orthopedic management of septic arthritis. Rheum Dis Clin North Am. 1998;24(2):275-286. doi:10.1016/s0889-857x(05)70009-0
Prognosis for Acute Infectious Arthritis
Acute nongonococcal bacterial arthritis can destroy articular cartilage, permanently damaging the joint within hours or days (1).
Gonococcal arthritis does not usually damage joints permanently. Factors that increase susceptibility to infectious arthritis may also increase disease severity.
In patients with rheumatoid arthritis, functional outcome is particularly poor, and the mortality rate is increased.
Prognosis reference
1. Gardner GC, Weisman MH. Pyarthrosis in patients with rheumatoid arthritis: a report of 13 cases and a review of the literature from the past 40 years. Am J Med. 1990;88(5):503-511. doi:10.1016/0002-9343(90)90430-l
Key Points
Gonococcal arthritis manifests with less severe acute inflammation than does acute nongonococcal bacterial arthritis and is less likely to cause residual joint damage.
Suspect infectious arthritis if patients have acute monoarticular or oligoarticular arthritis, particularly in patients at increased risk.
Test and culture synovial fluid to confirm or exclude the diagnosis; radiographs and routine laboratory studies are usually of little help.
Diagnose and treat infectious arthritis, particularly nongonococcal bacterial arthritis, as soon as possible.
Direct initial antibiotic therapy at pathogens suspected based on clinical and Gram stain findings.
Infected joints should be drained by serial aspiration, arthroscopic lavage, or arthrotomy for debridement.







