





")
The forces of labor and delivery occasionally cause physical injury to the infant. The incidence of neonatal injury resulting from difficult or traumatic deliveries is decreasing due to increasing rates of cesarean delivery in place of difficult versions, vacuum extractions, or mid- or high-forceps deliveries.
There is an increased risk of trauma when the infant is large for gestational age (which is sometimes associated with maternal chronic diabetes or maternal gestational diabetes) or when there is a breech or other abnormal presentation, especially in a primipara.
Facial Nerve Injury in Neonates
The facial nerve is the nerve injured most often. Although forceps pressure is a common cause, some injuries probably result from pressure on the nerve in utero, which may be due to fetal positioning (eg, from the infant's head lying against their own shoulder or against the pregnant patient's sacral promontory or a uterine fibroid).
Facial nerve injury usually occurs at or distal to its exit from the stylomastoid foramen and results in facial asymmetry, especially during crying. Identifying which side of the face is affected can be confusing, but the facial muscles on the side of the nerve injury cannot move. Injury can also occur to individual branches of the nerve, most often the mandibular.
Another cause of facial asymmetry is mandibular asymmetry resulting from intrauterine pressure; in this case, muscle innervation is intact and both sides of the face can move. In mandibular asymmetry, the maxillary and the mandibular occlusal surfaces are not parallel, which differentiates it from a facial nerve injury. A congenital anomaly that can cause an asymmetric smile is unilateral absence of the depressor anguli oris muscle; this anomaly is clinically insignificant but must be differentiated from facial nerve injury.
Testing for or treatment of facial nerve injury is not needed for peripheral facial nerve injuries or mandibular asymmetry. They usually resolve by age 2 to 3 months.
Brachial Plexus Injuries in Neonates
Brachial plexus injuries frequently follow lateral stretching of the neck during delivery caused by shoulder dystocia, breech extraction, or hyperabduction of the neck in cephalic presentations. Injuries can be due to simple stretching of the nerve, hemorrhage within a nerve, tearing of the nerve or root, or avulsion of the roots with accompanying cervical cord injury. Associated injuries (eg, fractures of the clavicle or humerus or subluxations of the shoulder or cervical spine) may occur. Intrauterine compression may also cause some cases.
Injuries may involve the
Upper brachial plexus (C5 to C7): Affects muscles around the shoulder and elbow
Lower plexus (C8 to T1): Primarily affects muscles of the forearm and hand
Entire brachial plexus: Affects entire upper extremity and often sympathetic fibers of T1
The site and type of nerve root injury determine the prognosis.
Erb palsy is a common brachial plexus injury. It is an upper brachial plexus (C5 to C7) injury causing adduction and internal rotation of the shoulder with pronation of the forearm. Sometimes the biceps reflex is absent and the Moro reflex is asymmetric. Ipsilateral paralysis of the diaphragm due to phrenic nerve injury also is common. Treatment of Erb palsy is usually supportive with physical therapy and protective positioning, which includes protecting the shoulder from excessive motion by immobilizing the arm across the upper abdomen and preventing contractures by gently doing passive range-of-motion exercises to involved joints every day starting at 1 week of age.


Klumpke palsy is rare and is a lower plexus injury that causes weakness or paralysis of the hand and wrist. The grasp reflex is usually absent, but the biceps reflex is present. Often, the sympathetic fibers of T1 are involved causing an ipsilateral Horner syndrome (miosis, ptosis, facial anhidrosis). Passive range-of-motion exercises are usually the only treatment needed.
Neither Erb palsy nor Klumpke palsy commonly causes demonstrable sensory loss, which suggests a tear or avulsion. These conditions usually improve rapidly, but deficits can persist. If the deficit is more severe or lasts for more than 1 or 2 weeks, physical therapy or occupational therapy for proper positioning and gentle movement of the arm are recommended. If there is no improvement over 1 or 2 months, there is increased risk of long-term disability and impaired growth. Evaluation by a pediatric neurologist and/or orthopedist at a pediatric specialty hospital is indicated to determine whether surgical exploration and microsurgical repair of the brachial plexus with nerve grafts may improve the outcome.
Involvement of the entire plexus is less common and results in a flaccid upper extremity with little or no movement, absent reflexes, and usually sensory loss. Ipsilateral Horner syndrome is present in the most severe cases. Ipsilateral pyramidal signs (eg, decreased movement, Babinski sign) indicate spinal cord trauma, and an MRI should be done.
Phrenic Nerve Injuries in Neonates
Most phrenic nerve injuries (about 75%) are associated with brachial plexus injury. Injury is usually unilateral and caused by a traction injury of the head and neck.
Infants have respiratory distress and decreased breath sounds on the affected side.
Treatment of phrenic nerve injury is supportive and typically requires continuous positive airway pressure or mechanical ventilation.
About one-third of infants recover spontaneously within the first month. Infants who do not recover may require surgical diaphragmatic plication.
Other Peripheral Nerve Injuries in Neonates
Injuries to other peripheral nerves (eg, the radial, sciatic, or obturator) are rare in neonates and are usually not related to labor and delivery. They are usually secondary to a local traumatic event (eg, an injection in or near the sciatic nerve).
Treatment of peripheral nerve injury includes placing the muscles antagonistic to those paralyzed at rest until recovery. Neurosurgical exploration of the nerve is seldom indicated.
In most peripheral nerve injuries, recovery is complete.
Spinal Cord Injury in Neonates
Spinal cord injury (see also Spinal Cord Injury in Children) is rare and involves variable degrees of cord disruption, often with hemorrhage. Complete disruption of the cord is very rare. Trauma usually occurs in breech deliveries after excess longitudinal traction to the spine. It can also be caused by cord compression due to epidural hemorrhage or hyperextension of the fetal neck in utero (the “flying fetus”). Injury usually affects the lower cervical region (C5 to C7). When the injury is higher, lesions are usually fatal because respiration is completely compromised. Sometimes a click or snap is heard at delivery.
Spinal shock with flaccidity below the level of injury occurs initially. Usually, there is patchy retention of sensation or movement below the lesion. Spasticity develops within days or weeks. Breathing is diaphragmatic because the phrenic nerve remains intact because its origin is higher (at C3 to C5) than the typical cord lesion. When the spinal cord lesion is complete, the intercostal and abdominal muscles become paralyzed and rectal and bladder sphincters cannot develop voluntary control. Sensation and sweating are lost below the involved level, which can cause fluctuations of body temperature with environmental changes.
An MRI of the cervical cord may show the lesion and excludes surgically treatable lesions, such as congenital tumors or hematomas pressing on the cord. The cerebrospinal fluid is usually bloody.
Treatment of spinal cord injury includes nursing care to prevent skin ulcerations, prompt treatment of urinary and respiratory infections, and regular evaluations to identify obstructive uropathy early.
With appropriate care, most infants survive for many years. The usual causes of death are recurring pneumonia and progressive loss of renal function.
Extracranial Head Injuries in Neonates
Head injury is the most common birth-related injury and is usually minor, but serious injuries sometimes occur.
Head molding
Head molding is not an injury, but parents may be concerned about it. It is common in vaginal delivery due to the pressure exerted by uterine contractions on the neonate’s malleable cranium as it passes through the birth canal. This molding is a normal process and is not a sign of trauma. It does not require treatment.
Scalp abrasions
Scalp abrasions and lesions, which are usually superficial and minor, can occur during deliveries that require the use of instruments (in up to 10% of neonates who had vacuum extraction) or scalp electrode monitoring. Unless there is infection, these abrasions usually require no treatment.
Caput succedaneum
Caput succedaneum is an extraperiosteal subcutaneous collection of serosanguinous fluid on the presenting portion of the scalp resulting from pressure during labor as the head delivers. It typically crosses suture lines.
Subgaleal hemorrhage
Subgaleal hemorrhage occurs between the galea aponeurosis and periosteum. It is characterized by a fluctuant mass over the entire scalp, including the temporal regions, and possibly the neck. The mass manifests in the first few hours after birth. This potential space under the scalp is large, and there can be significant blood loss and hemorrhagic shock, which may require a blood transfusion. A subgaleal hemorrhage may result from the use of forceps or a vacuum extractor, or may result from a coagulation disorder.
In some cases, severe hypovolemia and shock develop before the full extent of the subgaleal hemorrhage is clinically evident.
Treatment of subgaleal hemorrhage is mostly supportive with infusion of saline and packed red blood cells as required.
Cephalhematoma
Cephalhematoma is hemorrhage beneath the periosteum. It can be differentiated from subgaleal hemorrhage because it is sharply limited to the area overlying a single bone, the periosteum being adherent at the sutures. Cephalhematomas are commonly unilateral and occipital or parietal. In a small percentage of neonates, there is a linear fracture of the underlying bone. The hematoma usually manifests in the first few days of life and resolves over weeks.
Treatment of cephalhematoma is not required, but anemia or hyperbilirubinemia may result.
Occasionally, the hematoma calcifies into a bony mass.
Depressed skull fractures
Depressed skull fractures are uncommon. Most result from the head resting on a bony prominence in utero or from an assisted delivery using forceps. Infants with depressed skull fractures or other head trauma may also have subdural bleeding, subarachnoid hemorrhage, or contusion or laceration of the brain itself (see Intracranial Hemorrhage). Depressed skull fractures cause a palpable (and sometimes visible) step-off deformity, which must be differentiated from the palpable, elevated periosteal rim occurring with cephalhematomas.
CT is done to confirm the diagnosis of depressed skull fracture, and both CT and MRI may be useful when evaluating the neonate for other complications.
Neurosurgical elevation may be needed, and there is a risk of leptomeningeal cyst.
Intracranial Hemorrhage in Neonates
Hemorrhage in or around the brain can occur in any neonate but is particularly common among those born prematurely.
Major causes of intracranial hemorrhage include
Hypoxia-ischemia
Variations in blood pressure
Hypoperfusion with reperfusion
Abnormal pressures exerted on the head during labor
The germinal matrix is a mass of embryonic cells lying over the caudate nucleus on the lateral wall of the lateral ventricles that is vulnerable to hemorrhage. The presence of the germinal matrix makes intraventricular hemorrhage more likely in preterm infants. Risk of any intracranial hemorrhage also is increased by hematologic disorders (eg, vitamin K deficiency, hemophilia, disseminated intravascular coagulation).
Hemorrhage can occur in several central nervous system (CNS) spaces. Small hemorrhages in the subarachnoid space, falx, and tentorium are frequent incidental findings at autopsy of neonates who have died of non-CNS causes. Larger hemorrhages in the subarachnoid or subdural space, brain parenchyma, or ventricles are less common but more serious.
Intracranial hemorrhage is suspected in neonates with
Apnea
Seizures
Lethargy
Abnormal neurologic examination
Such infants should have a cranial imaging study as part of the initial evaluation. Cranial ultrasound is risk free, requires no sedation, and can readily identify blood within the ventricles or brain substance. CT is more sensitive than ultrasound for thin layers of blood in the subarachnoid or subdural spaces and for bony injury, but CT exposes the infant to ionizing radiation. MRI is more sensitive and specific than CT or ultrasound for intracranial blood and for brain injury but takes longer to produce images than CT and may require the infant to be sedated to limit movement and thereby improve image quality. CT is done to rapidly identify intracranial hemorrhage.
Treatment of intracranial hemorrhage depends on the location and severity of the hemorrhage but usually is only supportive, including giving vitamin K if not previously given and managing any underlying coagulation abnormality. In cases of significant hemorrhage (eg, subdural hemorrhage), neurosurgical consultation should be obtained to help identify infants requiring intervention.
Types of Intracranial Hemorrhage

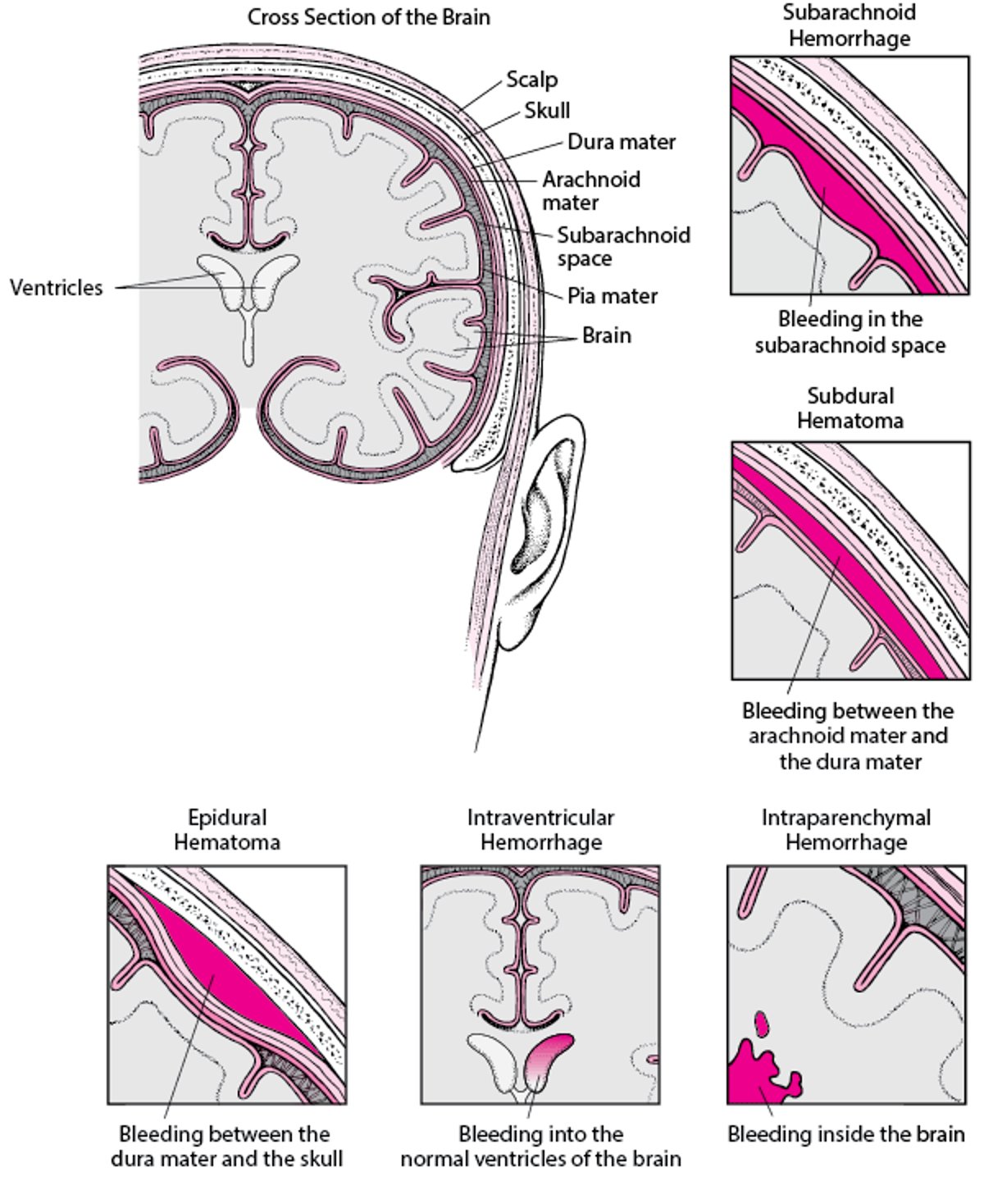
Epidural hematoma
Epidural hematoma is a collection of blood between the skull and the dura mater. It is rare in neonates but can occur in association with a skull fracture or cephalhematoma. Infants may present with apnea, seizures, or focal neurologic abnormalities. The fontanelles may be bulging if intracranial pressure is increased.
Most epidural hematomas are self-limiting and do not require treatment. If an intervention is required, surgical and nonsurgical options exist. Nonsurgical options are percutaneous epidural tapping or ultrasound-guided needle aspiration. Surgical options include craniotomy, which is reserved for cases that are rapidly progressing or not responsive to other interventions.
If identified and treated promptly, neurologic outcomes are good.
Intraventricular hemorrhage and/or intraparenchymal hemorrhage
Intraventricular hemorrhage (IVH) and/or intraparenchymal hemorrhage usually occurs during the first 3 days of life in infants < 1500 grams and/or < 32 weeks of gestational age. These hemorrhages are the most serious types of intracranial bleeding.
Hemorrhages occur most often in preterm infants, are often bilateral, and usually arise in the germinal matrix. The germinal matrix involutes after 32 weeks of gestation, thus IVH in term infants is rare but does occur.
IVH is graded as follows (1):
Grade 1: Limited to the germinal matrix
Grade 2: Hemorrhage into the ventricle without dilation
Grade 3: IVH with dilation of the ventricle
Grade 4: Same as grade III plus secondary intraparenchymal hemorrhage
Most bleeding episodes are subependymal or intraventricular and involve a small amount of blood. In severe hemorrhage (grades 3 and 4), there may be bleeding into the parenchyma with large amounts of blood in the cisterna magna and basal cisterns. Hypoxia-ischemia often precedes intraventricular and subarachnoid bleeding. Hypoxia-ischemia damages the capillary endothelium, impairs cerebral vascular autoregulation (already compromised in the preterm compared to the term infant) (2), and can increase cerebral blood flow and venous pressure, all of which make hemorrhage more likely. Most intraventricular hemorrhages are asymptomatic, but larger hemorrhages and those in infants with associated hydrocephalus may cause apnea, cyanosis, or sudden cardiovascular instability.
Treatment for most hemorrhages is supportive. However, infants with progressive hydrocephalus may require cerebrospinal fluid drainage by placement of a subcutaneous ventricular reservoir or shunt. Endoscopic ventriculostomy is increasingly being used to treat hydrocephalus in selected patients. Because many infants will have neurologic deficits, follow-up and referral for early intervention services are important.
Prognosis for infants with small IVHs (grades 1 and 2) is good. However, infants with large IVHs (grades 3 and 4) have a poor prognosis, especially if the hemorrhage extends into the parenchyma. Many infants who survive have residual neurologic deficits. Preterm infants with a history of severe IVH are at risk of developing posthemorrhagic hydrocephalus and must be monitored closely with physical examinations, head circumference measurements, and cranial ultrasound as indicated.
IVH and/or intraparenchymal hemorrhage references
1. Papile LA, Burstein J, Burstein R, Koffler H: Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1,500 gm. J Pediatr 92(4):529-534, 1978. doi: 10.1016/s0022-3476(78)80282-0
2. Gilard V, Tebani A, Bekri S, Marret S: Intraventricular Hemorrhage in Very Preterm Infants: A Comprehensive Review. J Clin Med 9(8):2447, 2020. doi: 10.3390/jcm9082447
Subarachnoid hemorrhage
Subarachnoid hemorrhage probably is the most common type of intracranial hemorrhage. It involves bleeding between the arachnoid membrane and the pia mater. Neonates typically present in the second or third day of life with apnea, seizures, lethargy, or an abnormal neurologic examination.
Treatment of subarachnoid hemorrhage is supportive with appropriate monitoring to detect hydrocephalus.
The prognosis for subarachnoid hemorrhage is usually good, with no significant long-term sequelae. However, with large hemorrhages, the associated meningeal inflammation may lead to a communicating hydrocephalus as the infant grows.
Subdural hemorrhage
Subdural hemorrhage involves bleeding between the dura and the pia mater. It results from tears in the falx, tentorium, or bridging veins.
Small, subdural hemorrhages up to 3 mm in thickness are very common, occurring in about half of asymptomatic full-term newborns who had MRI at ≤ 72 hours of age. Such hemorrhages are typically benign.
Large subdural hemorrhages tend to occur in neonates of primiparas, in large neonates, or after difficult deliveries. Neonates may present with apnea, seizures, a rapidly enlarging head, an abnormal neurologic examination with hypotonia, a poor Moro reflex, or extensive retinal hemorrhages.
Treatment of large subdural hemorrhage is supportive, but neurosurgical drainage of the hematoma may be necessary for rapidly progressing bleeding with compression of vital intracranial structures and worsening clinical and vital signs.
The prognosis for large subdural hemorrhage is guarded.

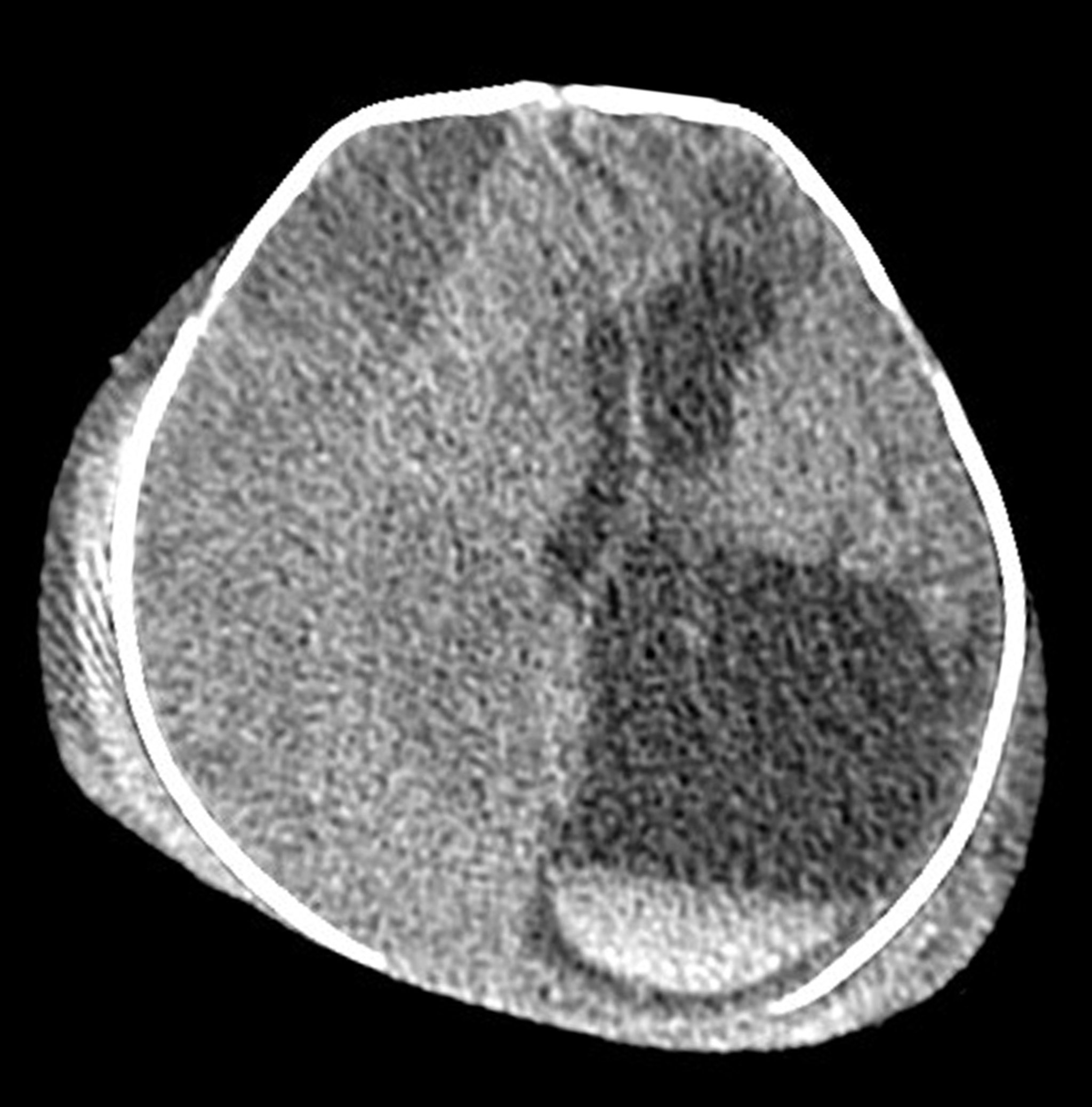
Living Art Enterprises, LLC/SCIENCE PHOTO LIBRARY
Fractures in Neonates
Midclavicular fracture, the most common fracture during birth, occurs with shoulder dystocia and with normal, nontraumatic deliveries. Initially, the neonate is sometimes irritable and may not move the arm on the involved side either spontaneously or when the Moro reflex is elicited. Most clavicular fractures are greenstick and heal rapidly and uneventfully. These fractures are commonly missed on examination in the hospital and are often diagnosed when a large callus forms at the fracture site within a week. Remodeling is completed within a month and there are no sequelae.
Specific treatment is not necessary, but some physicians recommend attempting to immobilize the arm for a week by pinning the shirt sleeve of the involved side to the opposite side of the neonate’s clothing. Analgesics usually are not necessary because neonates with a clavicular fracture typically do not show signs of pain.
The humerus and femur may be fractured in difficult deliveries. Most of these are greenstick, mid-shaft fractures, and excellent remodeling of the bone usually follows, even if moderate angulation occurs initially. A long bone may be fractured through its epiphysis, but prognosis is excellent.
Soft-Tissue Injuries in Neonates
All soft tissues are susceptible to injury during birth if they have been the presenting part or the fulcrum for the forces of uterine contraction. Edema and ecchymosis often follow injury, particularly of the periorbital and facial tissues in face presentations and of the scrotum or labia during breech deliveries.
Breakdown of blood within the tissues and conversion of heme to bilirubin result whenever a hematoma develops. This added burden of bilirubin may cause sufficient neonatal hyperbilirubinemia to require phototherapy and, rarely, exchange transfusion. No other treatment is needed.







