


Pleural disease, a hallmark of asbestos exposure, includes formation of pleural plaques, calcification, thickening, rounded atelectasis, adhesions, effusion, and mesothelioma. Diagnosis is based on history and chest x-ray or CT findings. Treatment is supportive.
(See also Overview of Asbestos-Related Disorders and Overview of Environmental and Occupational Pulmonary Disease.)
Asbestos is a family of naturally occurring silicates whose heat-resistant and structural properties are useful in construction and shipbuilding materials, automobile brakes, and some textiles. There are two main classes of asbestos: serpentine (which includes chrysotile) and amphibole (which includes amosite, crocidolite, anthophyllite, tremolite, and actinolite).
Asbestos can cause pleural disease other than mesothelioma, including pleural effusion, pleural plaques, and pleural thickening. Nonmalignant asbestos-related pleural disease is more common than parenchymal asbestosis and generally requires less exposure to develop.
Asbestos-related pleural disease is diagnosed by history of exposure and typical chest x-ray or CT findings. Bilateral pleural plaques and/or calcification of the diaphragm are virtually pathognomonic of previous exposure to asbestos. Chest CT is more sensitive than chest x-ray for detecting pleural disorders.
Benign asbestos pleural effusions (BAPE) are typically unilateral and occur ≥ 10 years after initial asbestos exposure. Analysis of the pleural effusion demonstrates an exudative process and can be serous, serosanguinous, or overtly bloody. Diagnostic evaluation should be undertaken to rule out cancer. BAPE can resolve over time and alone does not predict risk of cancer. Patients should be monitored for the development of other asbestos-related conditions.
Discrete pleural plaques typically affect the parietal pleura bilaterally and areas adjacent to the diaphragm. The apices and costophrenic angles tend to be spared. Plaque calcification is common. Chest CT can distinguish pleural disease from parenchymal disease and pleural fat. The latency from time of exposure to development of pleural plaques is generally ≥ 20 years. Pleural plaques are a marker of significant asbestos exposure; therefore, patients with pleural plaques should be monitored for the development of other asbestos-related diseases.

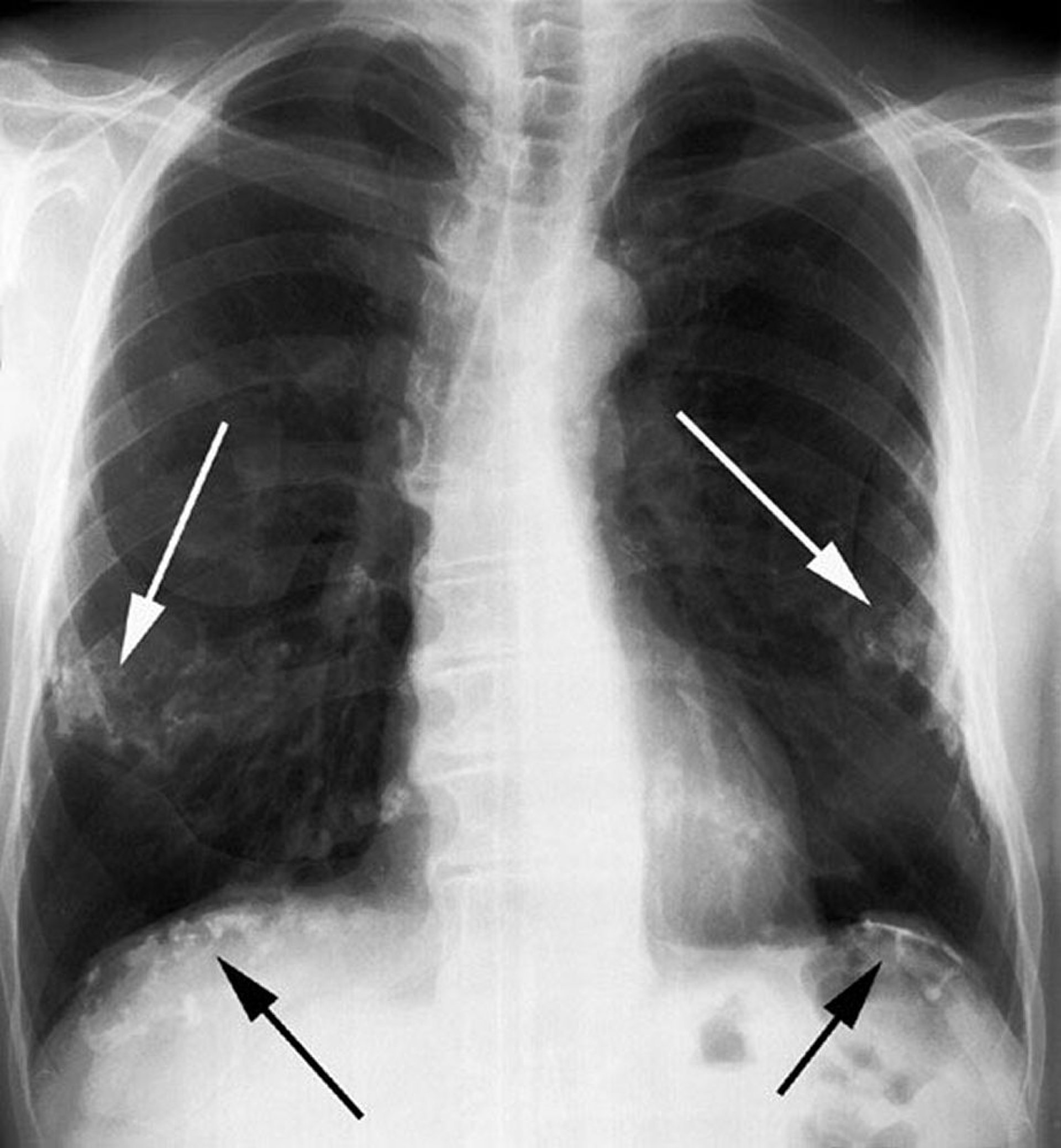
Image courtesy of David W. Cugell, MD.

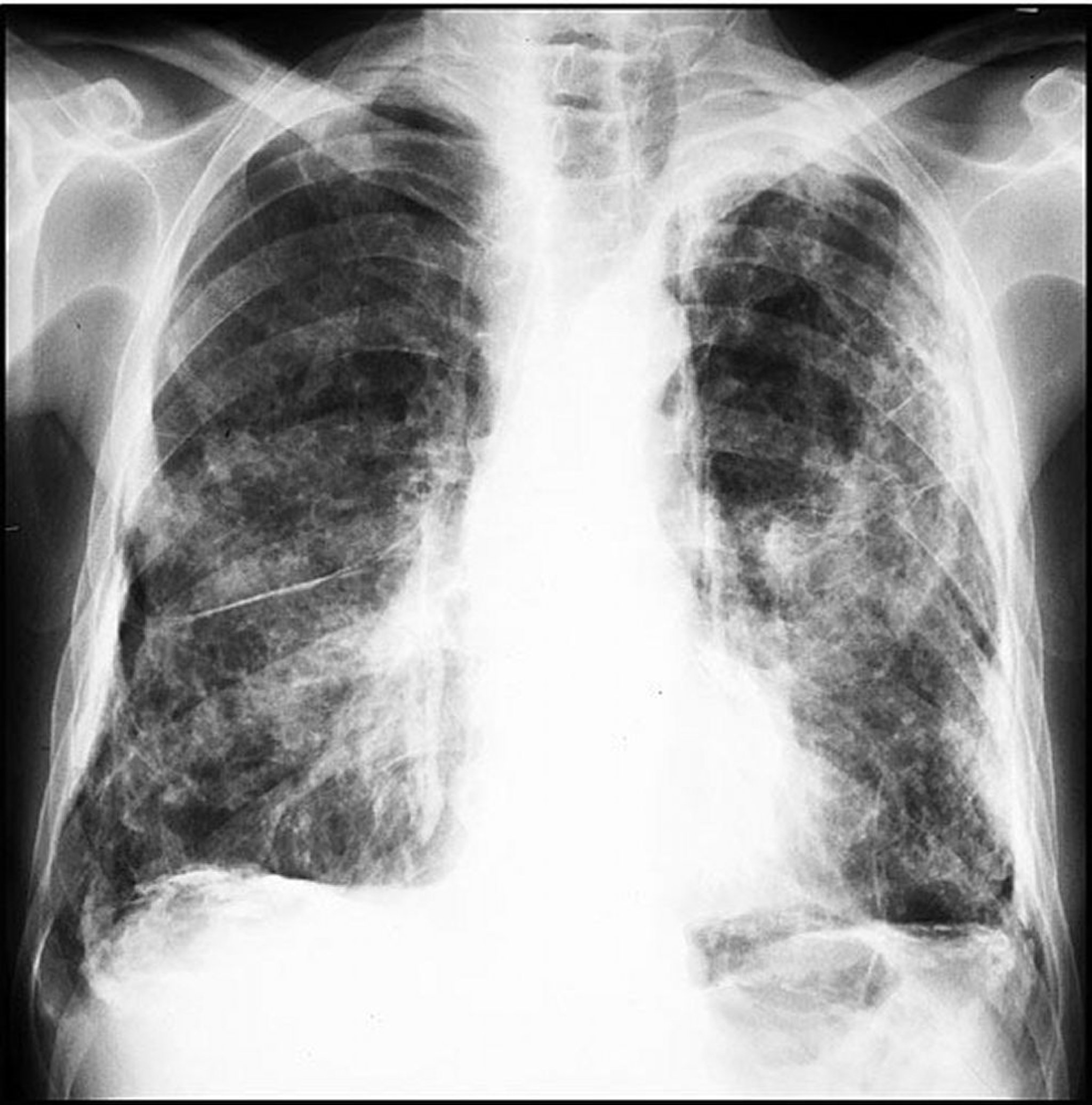
Image courtesy of David W. Cugell, MD.
Diffuse thickening affects visceral as well as parietal pleurae and may be a nonspecific reaction to pleural effusion. Diffuse pleural thickening can cause a restrictive defect, which may be symptomatic.
Rounded atelectasis is a benign manifestation of pleural thickening in which invagination of pleura into the parenchyma can entrap lung tissue, causing atelectasis. On chest x-ray and chest CT, rounded atelectasis typically appears as a curvilinear, scar-like mass, often in the lower lung zones, and should be differentiated from lung cancer.







