


Pneumothorax is air in the pleural space causing partial or complete lung collapse. Pneumothorax can occur spontaneously or result from trauma or medical procedures. Diagnosis is based on clinical criteria and chest x-ray. Most pneumothoraces require transcatheter aspiration or tube thoracostomy.
Etiology of Pneumothorax
Primary spontaneous pneumothorax occurs in patients without underlying pulmonary disease, classically in tall, thin young men in their teens and 20s. It is thought to be due to spontaneous rupture of subpleural apical blebs or bullae that result from smoking or that are inherited. It generally occurs at rest, although some cases occur during activities involving reaching or stretching. Primary spontaneous pneumothorax also occurs during diving and high-altitude flying.
Secondary spontaneous pneumothorax occurs in patients with underlying pulmonary disease. It most often results from rupture of a bleb or bulla in patients with severe chronic obstructive pulmonary disease (forced expiratory volume in one second [FEV1] < 1 L), HIV-related Pneumocystis jirovecii infection, cystic fibrosis, or any underlying pulmonary parenchymal disease (see table Causes of Secondary Spontaneous Pneumothorax). Secondary spontaneous pneumothorax is more serious than primary spontaneous pneumothorax because it occurs in patients whose underlying lung disease decreases their pulmonary reserve.
Catamenial pneumothorax is a rare form of secondary spontaneous pneumothorax that occurs within 48 hours of the onset of menstruation in premenopausal women and sometimes in postmenopausal women taking estrogen. The cause is intrathoracic endometriosis, possibly due to migration of peritoneal endometrial tissue through diaphragmatic defects or embolization through pelvic veins.
Causes of Secondary Spontaneous Pneumothorax
Type | Disorder |
|---|---|
More common | |
Pulmonary | Chronic obstructive pulmonary disease (COPD) Necrotizing pneumonia |
Less common | |
Pulmonary | |
Connective tissue disorders | |
Systemic rheumatic disorders | |
Other | Sarcoma Thoracic endometriosis |
Traumatic pneumothorax is a common complication of penetrating or blunt chest injuries.
Iatrogenic pneumothorax is caused by medical interventions, including transthoracic needle aspiration, thoracentesis, central venous catheter placement, mechanical ventilation, and cardiopulmonary resuscitation.
Pathophysiology of Pneumothorax
Intrapleural pressure is normally negative (less than atmospheric pressure) because of inward lung and outward chest wall recoil. In pneumothorax, air enters the pleural space from outside the chest or from the lung itself via mediastinal tissue planes or direct pleural perforation. Intrapleural pressure increases, and lung volume decreases.
Tension pneumothorax is a pneumothorax causing a progressive rise in intrapleural pressure to levels that become positive throughout the respiratory cycle and collapses the lung, shifts the mediastinum, and impairs venous return to the heart. Air continues to get into the pleural space but cannot exit. Without appropriate treatment, the impaired venous return can cause systemic hypotension, respiratory arrest, and cardiac arrest (pulseless electrical activity) within minutes. Tension pneumothorax most commonly occurs in patients receiving positive-pressure ventilation (with mechanical ventilation or particularly during resuscitation). Rarely, it is a complication of traumatic pneumothorax, when a chest wound acts as a one-way valve that traps increasing volumes of air in the pleural space during inspiration.

Symptoms and Signs of Pneumothorax
Small pneumothoraces are occasionally asymptomatic. Symptoms of pneumothorax include dyspnea and pleuritic chest pain. Dyspnea may be sudden or gradual in onset depending on the rate of development and size of the pneumothorax. Pain can simulate pericarditis, pneumonia, pleuritis, pulmonary embolism, musculoskeletal injury (when referred to the shoulder), or an intra-abdominal process (when referred to the abdomen). Pain can also simulate cardiac ischemia, although typically the pain of cardiac ischemia is not pleuritic.
Physical findings classically consist of absent tactile fremitus, hyperresonance to percussion, and decreased breath sounds on the affected side. If the pneumothorax is large, the affected side may be enlarged with the trachea visibly shifted to the opposite side. With tension pneumothorax, hypotension can occur.
Diagnosis of Pneumothorax
Chest imaging


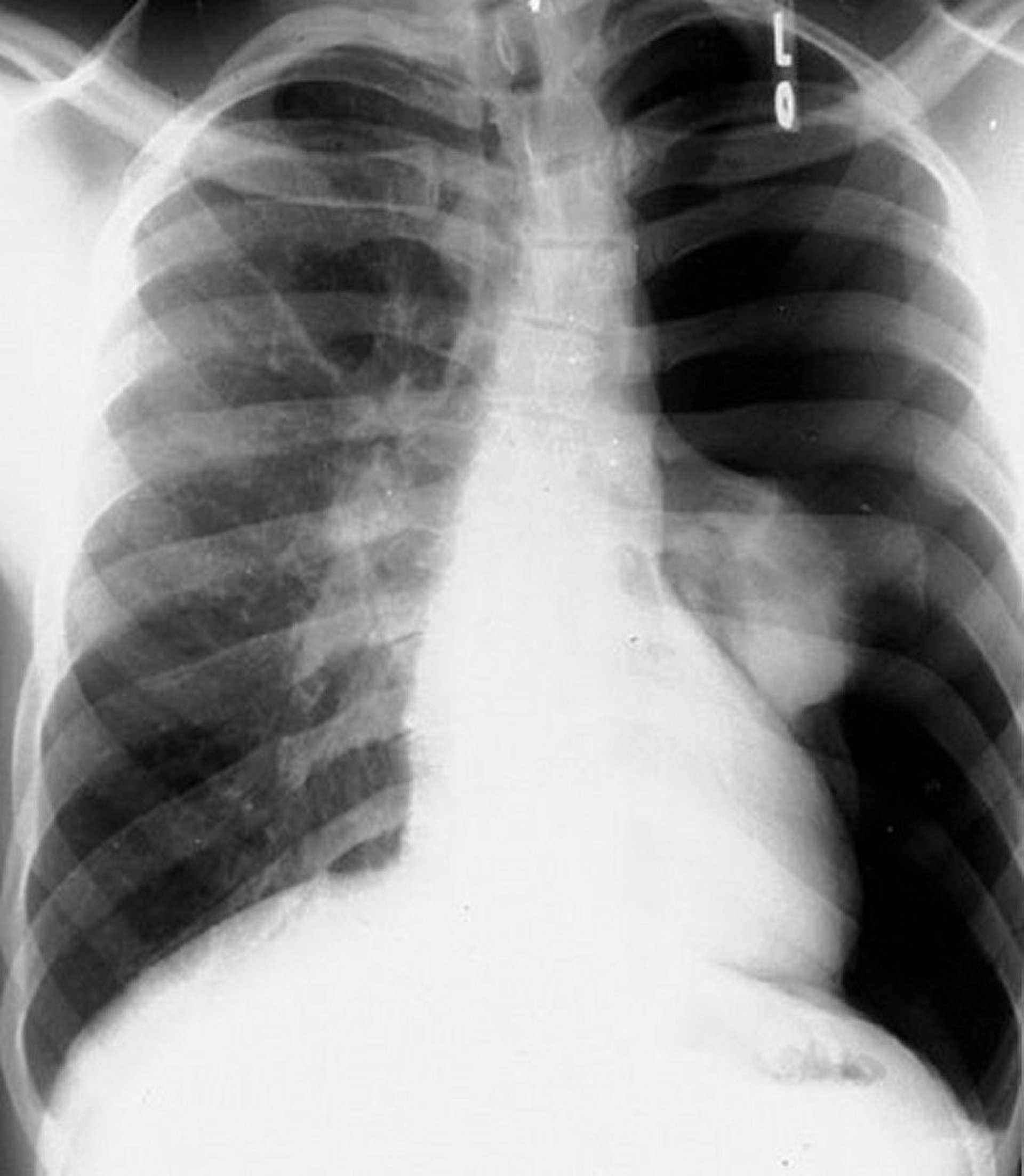
DU CANE MEDICAL IMAGING LTD/SCIENCE PHOTO LIBRARY
The diagnosis is suspected in patients whose condition is stable but who have dyspnea or pleuritic chest pain and is usually confirmed with upright inspiratory chest x-ray. Radiolucent air and the absence of lung markings juxtaposed between a shrunken lobe or lung and the parietal pleura are diagnostic of pneumothorax. Tracheal deviation and mediastinal shift occur with large pneumothoraces. The diagnosis can also be made using bedside ultrasonography in the absence of underlying lung disease.

By permission of the publisher. From Berman L. In Atlas of Anesthesia: Critical Care. Edited by R Miller (series editor) and RR Kirby. Philadelphia, Current Medicine, 1997.
The size of a pneumothorax is defined as the percentage of the hemithorax that is vacant. This percentage is estimated by taking 1 minus the ratio of the cubes of the width of the lung and hemithorax. For example, if the width of the hemithorax is 10 cm and the width of the lung is 5 cm, the ratio is 53/103= 0.125. Thus, the size of the pneumothorax is about 1 minus 0.125, or 87.5%. If adhesions are present between the lung and the chest wall, the lung does not collapse symmetrically, the pneumothorax may appear atypical or loculated, and the calculation is not accurate.
Small pneumothoraces (eg, < 10%) are sometimes overlooked on chest x-ray. In patients with possible pneumothorax, lung markings should be traced to the edge of the pleura on chest x-ray. Conditions that mimic pneumothorax radiographically include emphysematous bullae, skinfolds, folded bed sheets, and overlap of stomach or bowel markings on lung fields.
Pearls & Pitfalls
|

Treatment of Pneumothorax
Immediate needle decompression for tension pneumothoraces
Observation and follow-up x-ray for asymptomatic, primary spontaneous pneumothoraces regardless of size
Catheter aspiration or ambulatory treatment devices for symptomatic primary spontaneous pneumothoraces
Tube thoracostomy for secondary and traumatic pneumothoraces
Treatment depends on the type, size, and effects of the pneumothorax.
Primary spontaneous pneumothorax that does not cause respiratory or cardiac symptoms can be safely observed without treatment if follow-up chest x-rays done at 4 hours show no progression and if the patient is physiologically stable, regardless of pneumothorax size.
Symptomatic primary spontaneous pneumothoraces should be evacuated by catheter aspiration or by ambulatory treatment devices (drainage device connected to a one-way valve, with which the patient can ambulate, eg, Heimlich valve). Tube thoracostomy with hospital admission is an alternative.
Catheter aspiration is accomplished by insertion of a small-bore (about 7 to 9 French) IV or pigtail catheter into the chest in the 2nd intercostal space at the midclavicular line. The catheter is attached to a 3-way stopcock and syringe. Air is withdrawn from the pleural space through the stopcock into the syringe and expelled into the room. The process is repeated until the lung re-expands or until 4 L of air are removed. If the lung expands, the catheter can be removed or kept in place attached to a one-way Heimlich valve (thus permitting ambulation), and the patient need not be hospitalized. If the lung does not expand, a chest tube should be inserted, and the patient should be hospitalized. Primary spontaneous pneumothoraces can also be managed initially with a chest tube attached to a water seal without or with suction. Patients with primary spontaneous pneumothoraces should also undergo smoking cessation counseling.
Tube thoracostomy using a small bore (< 14 French) drain is generally used to treat secondary and traumatic pneumothoraces. Symptomatic patients with iatrogenic pneumothoraces are best managed initially with aspiration.
Tension pneumothorax is a medical emergency and should be diagnosed clinically; time should not be wasted confirming the diagnosis with a chest x-ray. It should be treated immediately by needle thoracostomy, which involves inserting a 14- or 16-gauge needle deep enough to fully penetrate the chest wall with a catheter through the chest wall in the 2nd intercostal space at the midclavicular line. The sound of high-pressure air escaping confirms diagnosis. The catheter can be left open to air or attached to a Heimlich valve. Emergency decompression must be followed immediately by tube thoracostomy, after which the catheter is removed.

Complications of Pneumothorax
The 3 main problems encountered when treating pneumothorax are
Air leaks
Failure of the lung to expand
Re-expansion pulmonary edema
Air leaks are usually due to the primary defect—ie, continued leakage of air from the lung into the pleural space—but can be due to air leaking around the chest tube insertion site if the site is not properly sutured and sealed. Air leaks are more common in secondary than in primary spontaneous pneumothorax. Most resolve spontaneously in < 1 week.
Failure of the lung to re-expand is usually due to one of the following:
Persistent air leak
Endobronchial obstruction
Trapped lung
Malpositioned chest tube
Blood pleurodesis (a blood patch), endobronchial valves, thoracoscopy, or thoracotomy should be considered if an air leak or an incompletely expanded lung persists beyond 1 week.
Re-expansion pulmonary edema occurs when the lung is rapidly expanded, as occurs when a chest tube is connected to negative pressure after the lung has been collapsed for > 2 days. Treatment is supportive, with oxygen, diuretics, and cardiopulmonary support as needed.
Prevention of Pneumothorax
Recurrence rates in large studies ranged from 19% to 29% at 1 year after initial primary spontaneous pneumothorax (1, 2), but higher in cases of secondary pneumothorax.
The best preventive procedure is video-assisted thoracic surgery (VATS) in which blebs are stapled and pleurodesis is done with pleural abrasion, parietal pleurectomy, or talc insufflation; in some medical centers, thoracotomy is still used. (VATS) in which blebs are stapled and pleurodesis is done with pleural abrasion, parietal pleurectomy, or talc insufflation; in some medical centers, thoracotomy is still used.
These procedures are recommended in primary pneumothorax after a second occurrence, in some cases after a first episode (eg, tension pneumothorax, at-risk profession [eg, pilots, diving]), in secondary pneumothorax, or when initial treatment fails to resolve the pneumothorax with ongoing air leak. Recurrence after these procedures is reduced (3). If thoracoscopy cannot be done or is contraindicated, chemical pleurodesis through a chest tube may be done; this procedure, though much less invasive, reduces the recurrence rate.
Prevention references
1. Hallifax RJ, Goldacre R, Landray MJ, Rahman NM, Goldacre MJ. Trends in the Incidence and Recurrence of Inpatient-Treated Spontaneous Pneumothorax, 1968-2016. JAMA 2018;320(14):1471-1480. doi:10.1001/jama.2018.14299
2. Walker SP, Bibby AC, Halford P, Stadon L, White P, Maskell NA. Recurrence rates in primary spontaneous pneumothorax: a systematic review and meta-analysis. Eur Respir J 2018;52(3):1800864. Published 2018 Sep 6. doi:10.1183/13993003.00864-2018
3. Lin Z, Zhang Z, Wang Q, Li J, Peng W, Ge G. A systematic review and meta-analysis of video-assisted thoracoscopic surgery treating spontaneous pneumothorax. J Thorac Dis 2021;13(5):3093-3104. doi:10.21037/jtd-21-652
Key Points
Primary spontaneous pneumothorax occurs in patients without underlying pulmonary disease, classically in tall, thin young men in their teens and 20s.
Secondary spontaneous pneumothorax occurs in patients with underlying pulmonary disease; it most often results from rupture of a bleb or bulla in patients with severe chronic obstructive pulmonary disease.
Diagnosis is by upright chest x-ray or ultrasonography, except for tension pneumothorax, which is diagnosed clinically as soon as suspected.
Primary spontaneous pneumothorax that does not cause respiratory or cardiac symptoms can be safely observed without treatment if follow-up chest x-rays done at about 4 hours show no progression, with follow up regularly over the subsequent weeks.
Symptomatic primary spontaneous pneumothoraces should be evacuated by catheter aspiration, ambulatory devices, or tube thoracostomy.
Secondary and traumatic pneumothoraces are generally treated with tube thoracostomy.
Video-assisted thoracic surgery (VATS) and other procedures can help prevent recurrences of spontaneous pneumothorax .







