



Pneumocystis jirovecii, an atypical fungus, is a common cause of pneumonia in immunosuppressed patients, especially in those infected with human immunodeficiency virus (HIV) and in those receiving systemic corticosteroids. Symptoms include fever, dyspnea, and dry cough. Diagnosis requires demonstration of the organism in an induced sputum specimen or bronchoscopic sample. Treatment is with antibiotics, usually trimethoprim/sulfamethoxazole or dapsone plus trimethoprim, clindamycin/primaquine, atovaquone, or pentamidine. Patients with PaO2 or dapsone plus trimethoprim, clindamycin/primaquine, atovaquone, or pentamidine. Patients with PaO2< 70 mm Hg or oxygen saturation < 92% receive systemic corticosteroids. Prognosis is generally good with timely treatment.
Topic Resources



(See also Overview of Pneumonia and Pneumonia in Immunocompromised Patients.)
Pneumocystis jirovecii is a ubiquitous organism transmitted by aerosol route and causes no disease in immunocompetent patients. However, some patients are at risk of developing P. jirovecii pneumonia:
Patients with HIV infection and CD4+ T cell counts < 200/microL or < 14%
Organ transplant recipients
Patients with hematologic cancers
Patients taking corticosteroids or other immunosuppressive medications
With the advent of effective antiretroviral therapy, the incidence of Pneumocystis jiroveciiinfection has dramatically declined in patients with HIV infection. However, patients who are not aware that they have HIV or not taking antiretroviral therapy remain at high risk for developing P. jirovecii pneumonia.
Most patients have fever, dyspnea, and a dry, nonproductive cough that evolves over several weeks (HIV infection) or over several days (other causes of compromised cell-mediated immunity). Dyspnea is common.
Diagnosis of Pneumocystis jirovecii Pneumonia
Chest x-ray
Pulse oximetry
Histopathologic confirmation
Physical examination reveals fever and tachypnea in most patients. To diagnose Pneumocystis jirovecii pneumonia, patients should have chest x-ray and assessment of oxygenation by pulse oximetry.
Chest x-ray characteristically shows diffuse, bilateral perihilar infiltrates, but 20 to 30% of patients have normal x-rays. A CT scan often shows ground glass infiltrates, even when the chest x-ray is normal.
Hypoxemia may be present even when chest x-ray shows no infiltrate; this finding can be an important clue to diagnosis. If pulse oximetry is normal, arterial blood gas (ABG) measurements are often obtained to assess for an increase in the alveolar-arterial oxygen gradient.
Pearls & Pitfalls
|
If done, pulmonary function tests show altered diffusing capacity (although pulmonary function tests are rarely done as a diagnostic test for Pneumocystis jirovecii pneumonia).

Elevated levels of serum beta-D glucan and lactate dehydrogenase (LDH) are nonspecific but can support the diagnosis.
Demonstration of Pneumocystis jirovecii in a respiratory specimen is needed for confirmation of the diagnosis. Polymerase chain reaction (PCR)–based detection has the highest diagnostic yield. Direct fluorescent antibody staining with a monoclonal antibody is often used. Methenamine silver, Giemsa, Wright-Giemsa, modified Grocott, or Weigert-Gram stains can be used but are less sensitive. Appropriate respiratory specimens include sputum specimens (usually induced) and bronchoalveolar lavage or endotracheal aspirates (in intubated patients). If induced sputum is negative, bronchoscopy with lavage should be done as it has a much higher sensitivity. in a respiratory specimen is needed for confirmation of the diagnosis. Polymerase chain reaction (PCR)–based detection has the highest diagnostic yield. Direct fluorescent antibody staining with a monoclonal antibody is often used. Methenamine silver, Giemsa, Wright-Giemsa, modified Grocott, or Weigert-Gram stains can be used but are less sensitive. Appropriate respiratory specimens include sputum specimens (usually induced) and bronchoalveolar lavage or endotracheal aspirates (in intubated patients). If induced sputum is negative, bronchoscopy with lavage should be done as it has a much higher sensitivity.

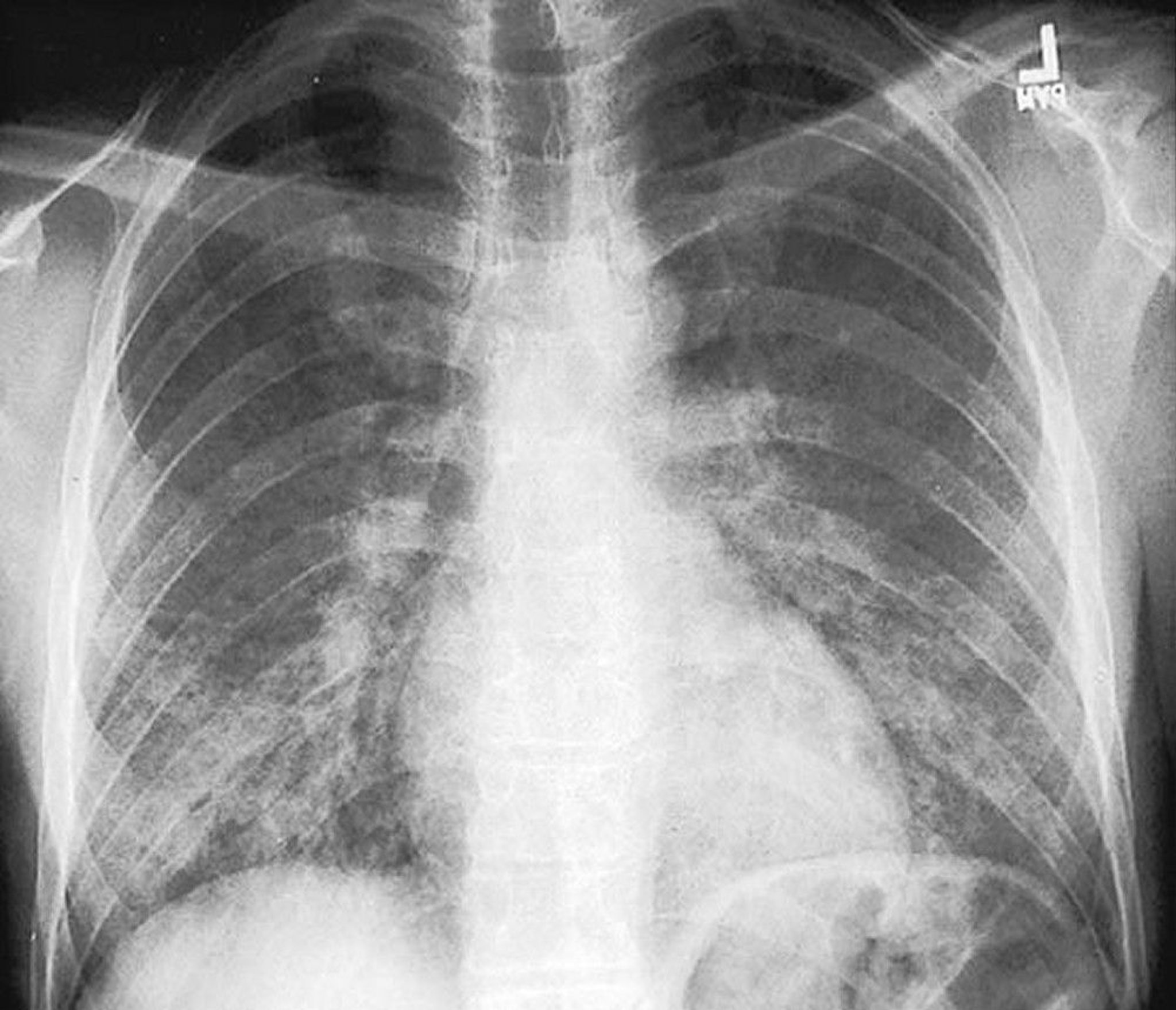
By permission of the publisher. From Huang L, Piliero P. In Bone's Atlas of Pulmonary and Critical Care Medicine. Edited by J Crapo. Philadelphia, Current Medicine, 2005.
Treatment of Pneumocystis jirovecii Pneumonia
Trimethoprim/sulfamethoxazole
Corticosteroids if partial pressure of arterial oxygen (PaO2) is < 70 mm Hg or pulse oximetry is < 92% while breathing room air
Treatment is with trimethoprim/sulfamethoxazole (TMP/SMX). Treatment can be started before diagnosis is confirmed because P. jirovecii cysts persist in the lungs for weeks. Adverse effects of treatment are more common among patients with acquired immunodeficiency syndrome (AIDS) and include rash, neutropenia, hepatitis, and fever.
Alternative regimens, which are also given for 21 days, use
Trimethoprim with dapsoneTrimethoprim with dapsone
Clindamycin plus primaquineClindamycin plus primaquine
PentamidinePentamidine
Atovaquone (for mild pneumonia)Atovaquone (for mild pneumonia)
The major limitation of pentamidine is the high frequency of toxic adverse effects, including acute kidney injury, hypotension, and hypoglycemia. The major limitation of pentamidine is the high frequency of toxic adverse effects, including acute kidney injury, hypotension, and hypoglycemia.
Adjunctive therapy with corticosteroids is recommended for patients with a PaO2 < 70 mm Hg or pulse oximetry < 92% while breathing room air. Corticosteroid doses are decreased over 21 days.
Prognosis for Pneumocystis jirovecii Pneumonia
Overall mortality is high for patients hospitalized with P. jirovecii pneumonia. Risk factors for death may include previous history of P. jirovecii pneumonia, older age, and, in patients with HIV infection, CD4+ T cell count < 50 cells/microL.
Prevention of Pneumocystis jirovecii Pneumonia
Patients with HIV infection who have had P. jirovecii pneumonia or who have a CD4+ T cell count < 200 cells/microL should receive prophylaxis with TMP/SMX; if this antibiotic is not tolerated, dapsone or aerosolized pentamidine can be used. These prophylactic regimens are also indicated for many patients without HIV infection who are at risk of 200 cells/microL should receive prophylaxis with TMP/SMX; if this antibiotic is not tolerated, dapsone or aerosolized pentamidine can be used. These prophylactic regimens are also indicated for many patients without HIV infection who are at risk ofP. jirovecii pneumonia.
Key Points
Consider P. jirovecii pneumonia in patients who are immunosuppressed, even if they have mild respiratory symptoms and even if the chest x-ray is normal.
Do histopathologic examination on induced sputum or bronchoscopically obtained samples.
Treat patients with trimethoprim/sulfamethoxazole, adding a corticosteroid if PaO2 is < 70 mm Hg.







