



- Overview of Heart Defects
- Aortopulmonary Window
- Aortic Valve Stenosis in Children
- Atrial and Ventricular Septal Defects
- Atrioventricular Septal Defects
- Bicuspid Aortic Valve
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Double Outlet Right Ventricle
- Ebstein Anomaly
- Hypoplastic Left Heart Syndrome
- Patent Ductus Arteriosus
- Persistent Truncus Arteriosus
- Pulmonary Valve Stenosis in Children
- Tetralogy of Fallot
- Total Anomalous Pulmonary Venous Return (TAPVR)
- Transposition of the Great Arteries
- Other Birth Defects of the Heart
Aortic valve stenosis is a narrowing of the valve that opens to allow blood to flow from the left ventricle into the aorta and then to the body.
Topic Resources

This defect makes the heart work harder to pump blood to the rest of the body.
When valve narrowing is mild, most children have no symptoms.
When valve narrowing is more severe, children may gradually develop symptoms such as fatigue, chest pain, or shortness of breath or fainting during exercise.
Infants with severe aortic valve stenosis usually become very ill within the first weeks of life.
The diagnosis is suspected when a heart murmur is noticed during a doctor's examination and confirmed by echocardiography (ultrasonography of the heart).
Surgery or a catheter procedure may be needed to fix the valve. Very abnormal valves may need to be replaced.
(See also Overview of Heart Defects. For this disorder in adults, see Aortic Stenosis.)
To propel blood through the narrowed aortic valve, the left ventricle must pump under very high pressures. Sometimes, not enough blood is pumped to supply the body with oxygenated blood. In newborns, the left ventricle may be suddenly stressed after birth and may not pump well. The aortic valve obstruction is sometimes progressive and, if it becomes severe, may lead to the heart failing to pump adequately at any age.
The most common cause of aortic valve stenosis is bicuspid aortic valve. The aortic valve is the valve that opens with each heartbeat to allow blood to flow from the heart to the body. A normal aortic valve has three cusps, or leaflets. When the valve is bicuspid, it has only two cusps instead of three.
Symptoms of Aortic Valve Stenosis in Children
Infants with severe aortic valve stenosis become irritable and have poor food intake, sweating while they are eating, difficulty breathing, an unnatural pale or gray color to the skin, cool hands and feet, decreased number of wet diapers, and a rapid heartbeat.
Most older children with aortic valve stenosis do not have any symptoms. As the narrowing becomes more severe, however, they may develop fatigue, shortness of breath, palpitations (sense of racing heart beat), fainting, or chest pain during sports or other vigorous activity.
In adolescents, severe aortic valve stenosis may lead to sudden death, most often during exercise, presumably because of an erratic heart rhythm caused by poor blood flow through the coronary arteries to the heart.
Diagnosis of Aortic Valve Stenosis in Children
Echocardiography
A doctor suspects aortic valve stenosis after detecting a particular heart murmur and sometimes a clicking sound when listening to the heart. A heart murmur is a sound created by turbulent blood flow through narrowed or leaking heart valves or through abnormal heart structures.
The pulses in the arms and legs may be weaker than normal. Infants may have signs of shock, including very poor or absent pulses, poor blood flow to the body with cold hands and feet and grayish pallor of the skin, breathing distress, and an enlarged liver.
Echocardiography (ultrasonography of the heart) shows the abnormal aortic valve and can measure the "tightness" of the valve. Valve leakage (in which some blood flows back from the aorta into the heart) may also be present. Echocardiography also shows whether the left ventricle is thickened, stretched, or weakened due to the stress of pumping blood through the narrowed valve.
Cardiac catheterization may be used to determine the severity of the narrowing.
Treatment of Aortic Valve Stenosis in Children
Surgery to widen or replace the valve
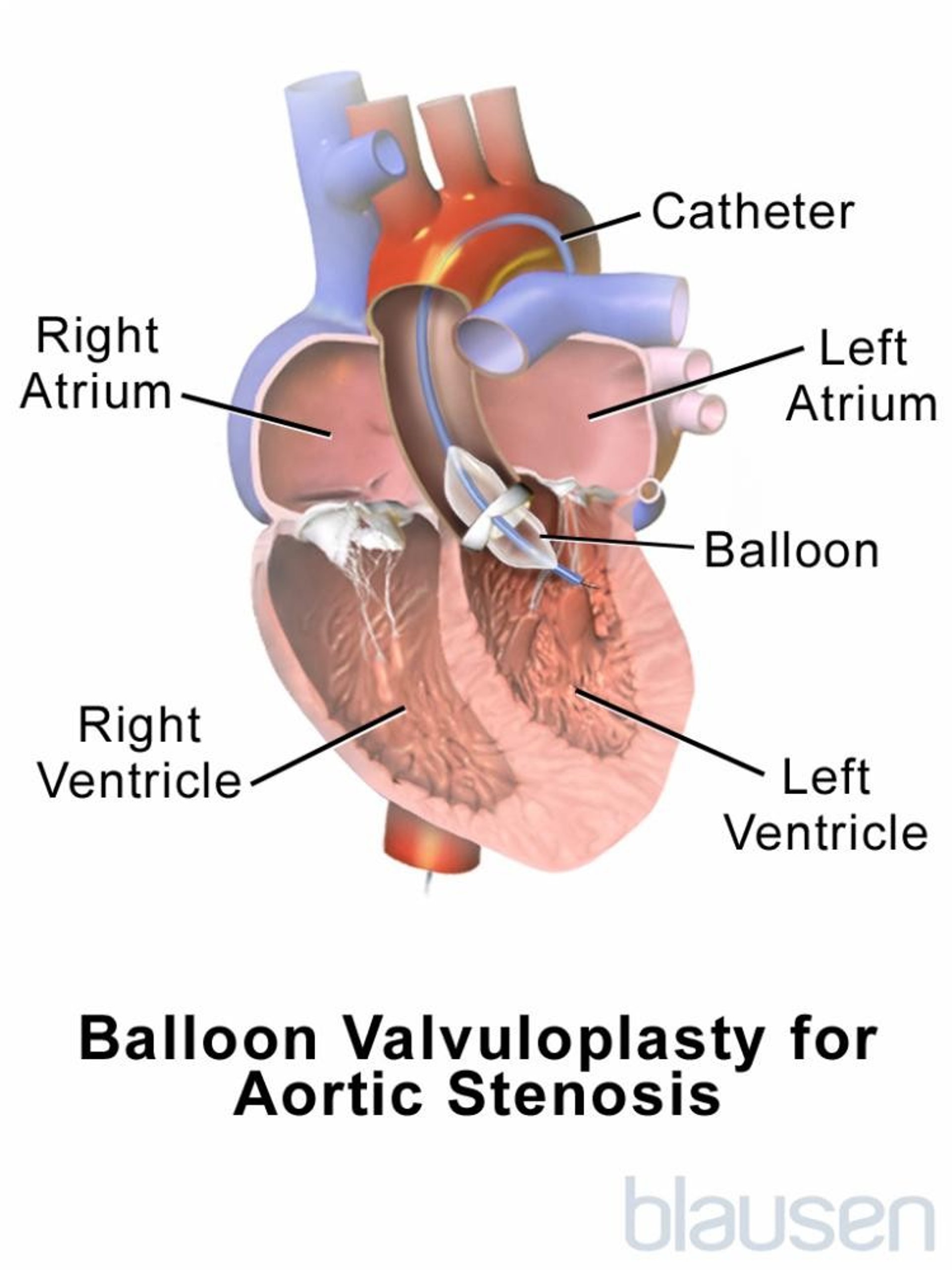
Cardiac catheterization with balloon valvuloplasty (using a balloon at the end of a catheter to widen the stiffened valve)
In infants with severe aortic valve stenosis, doctors may need to immediately give a medication, a prostaglandin, that will reopen or keep open the ductus arteriosus, a blood vessel that connects the pulmonary artery and the aorta (see also Normal Fetal Circulation). Normally, the ductus arteriosus closes soon after birth. A widely opened ductus can temporarily help supply blood to the body when too little is getting through the tight aortic valve. The medication is given by vein (intravenously). Urgent surgery or balloon valvuloplasty is needed soon after diagnosis.
For children with severe narrowing or symptoms, the aortic valve must be widened or replaced. Widening the valve can be done during cardiac catheterization by a procedure called balloon valvuloplasty, or by surgery. For balloon valvuloplasty, a thin tube (catheter) with a balloon at its tip is passed through a blood vessel in the groin into the narrowed valve. The balloon is inflated and used to stretch the narrowed opening of the valve.

Surgery is needed instead of a catheterization procedure when the valve is unusually small or is both leaky and narrowed. Surgery is also done if the child has additional heart problems that must be treated surgically. It is desirable to fix the valve if possible. If the valve cannot be fixed, it can be replaced with a metal artificial valve, with a tissue valve, or with the child's own good pulmonary valve (this is called the Ross procedure).
Children with a metal artificial valve must take an anticoagulant medication, such as warfarin, to prevent blood clots from forming.Children with a metal artificial valve must take an anticoagulant medication, such as warfarin, to prevent blood clots from forming.
Children who have valve replacement need to take antibiotics before visits to the dentist and before certain surgeries (such as on the respiratory tract). These antibiotics are used to prevent a serious heart infection called endocarditis.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides an overview of common birth defects of the heart for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing antibiotic use, for parents and caregivers







